
Abstract
Objective:
Hyponatremia occurs in patients with nasopharyngeal cancer (NPC) on chemoradiotherapy and causes prolonged hospitalization, low quality of life, and increased mortality. This study aimed to determine the associated factors of hyponatremia in patients with NPC on chemoradiotherapy and investigate changes in hyponatremic events over time.
Methods:
We retrospectively reviewed patients with NPC who underwent complete concurrent chemoradiotherapy between 2014 and 2024. Hyponatremia was defined as serum sodium levels <130 mmol/L. The median follow-up time was reported in person-months (pm); the incidence rate was defined as the number of events per 1000 pm. The Poisson regression model was used to estimate the incident density ratios and identify hyponatremia predictors.
Results:
A total of 381 patients were included in this study. The total follow-up time was 59 354 pm; the median follow-up time was 164 pm (interquartile range 135-193). There were 259 patients (68%) who never had hyponatremia. Hyponatremia was common in the first 2 months of treatment. Significant factors shown on univariate and multivariate regression analyses were age >50 years, tube feeding alone, advanced nodal metastasis, distant metastasis, carboplatin use, high-grade mucositis, and skin complications.
Conclusions:
Hyponatremia frequently occurs in the first 2 months of NPC treatment. Advanced age, tube feeding alone, advanced nodal metastasis, distant metastasis, carboplatin use, high-grade mucositis, and skin complications are significantly associated with hyponatremic events.
Introduction
Nasopharyngeal cancer (NPC) is an epithelial malignancy distinct from other head and neck tumors. According to the GLOBOCAN database, the worldwide incidence of new NPC cases was 129 079, accounting for 0.7% of all cancer diagnoses, with 72 987 deaths predicted in 2018. 1 For a decade, the NPC incidence has steadily declined; however, histological subtype classification showed that the incidence of non-keratinizing carcinoma (types II and III) remained relatively constant. 2 The incidence rates also vary across the regions, with East and Southeast Asia, the Middle East, North Africa, and the Arctic region having increased incidences compared with the worldwide rates. According to the National Comprehensive Cancer Network guidelines, most patients are diagnosed at an advanced stage of the disease that requires concurrent chemoradiotherapy. Radical-dose radiation covering the nasopharynx and regional neck nodes with platinum-based chemotherapy has been the standard treatment regimen for more than 20 years. Complications of treatment remain one of the challenges in improving survival and quality of life.
Hyponatremia is typically observed in 5% to 30% of patients with active cancer, causing extended hospitalization with low quality of life, and is a leading cause of increased healthcare costs. 3 Although many patients with hyponatremia are asymptomatic, serum sodium level rapidly decreases to a substantial extent and may cause abnormal neurological functions such as lethargy, drowsiness, muscle cramps, seizures, or even coma. The hazard ratio for death occurring within 90 days in patients with hyponatremia is almost 3-fold higher than that in normonatremic patients with cancer. 4 Moreover, the presence of hyponatremia in patients with cancer is a determinant prognostic biomarker that predicts the response to treatment in some cancer types. 5 The incidence of hyponatremia varies depending on patient status, type of cancer, and treatment regimen. Among patients with head and neck cancers, hyponatremia in NPC cases is a common cause of hospital readmission in our institute. Head and neck cancer with hyponatremia significantly increases all-cause mortality compared with other cancers. 6 Recently, hyponatremia among patients with head and neck cancer, who undergo surgical resection, was found to be associated with an increased risk of perioperative morbidity of all types, such as the need for blood transfusion, longer intensive care unit stay, and renal and cardiac complications compared with those with normonatremia. 7 Patients are at high risk of this condition due to cancer itself or complications after chemoradiotherapy, such as mucositis, dysphagia, or cachexia from poor oral intake. In addition, all levels of patients presenting with hyponatremia are related to a level-dependent 2- to 5-fold increased risk of being diagnosed with head and neck cancers. 8
NPC treatment continues to advance, with an increasing emphasis on decreasing morbidity, improving the quality of life, and increasing overall survival. Until now, few studies have investigated the incidence and prediction of the development of hyponatremia in patients with NPC following treatment. Understanding the risk of hyponatremia is crucial for optimizing treatment outcomes. Therefore, the present study aimed to assess the factors associated with hyponatremia in patients with NPC who underwent concurrent chemoradiotherapy and determine hyponatremic events with trend changes over time during treatment.
Materials and Methods
Study Setting and Populations
Following approval from the Institutional Review Board of Songkla University, this retrospective study was conducted at the Department of Otolaryngology – Head and Neck Surgery, Songklanagarind Hospital, Prince of Songkla University. The electronic medical records of all patients diagnosed with NPC who received complete treatment between January 2014 and December 2024 were extracted from the information system database of our center. The inclusion criteria were patients aged between 18 and 70 years who were diagnosed with NPC and who received complete concurrent chemoradiotherapy. Patients who underwent supportive treatment only, those with insufficient laboratory data, those diagnosed with residual or recurrent NPC, and those whose treatment was not completed were excluded.
Data Collection
Demographic and clinical variables, including age, sex, medications, presence of comorbidities, tumor stage, histopathological grade based on the World Health Organization (WHO) guidelines, blood profile, type of chemotherapeutic agent, and disease course, were collected. The patient’s performance status was measured using the Eastern Cooperative Oncology Group performance scale. Data on baseline blood tests, including complete blood count, renal function screening, and serum electrolyte testing, were also collected. The data were collected with the assistance of the Division of Digital Innovation and Data Analytics. Serum sodium and creatinine concentrations were determined using a Roche Modular P800 Chemistry analyzer (Roche Diagnostics (Thailand) Limited, the Diagnostics Division of the Roache Group, F. Hoffmann-La Roche Ltd, Switzerland). The reference level for the normal range of serum sodium was 135 to 145 mmol/L, and a serum sodium level <130 mmol/L was defined as hyponatremia. Serum sodium concentrations were obtained at baseline, before each treatment, and when the patients were cleared for discharge or upon the development of clinical symptoms. The estimated glomerular filtration rate was calculated using a simplified modification of the diet for renal disease formulations.
Complications during treatment, including mucositis (according to the WHO oral mucositis severity grading), infection, and skin complications, were also recorded. The severity of radiation-induced skin reactions, xerostomia, and mucositis was classified on a scale of 0 to 4, based on the Radiation Therapy Oncology Group/European Organization for Research and Therapy of Cancer grading system.
Treatment
All patients underwent a pretreatment baseline assessment that included a complete medical history, physical examination, complete otolaryngologic examination, tumor staging, blood tests for biochemistry and hematology profiles, plain chest radiography, magnetic resonance imaging of the nasopharynx and neck, and bone scintigraphy for metastatic cancer detection. More than 90% of patients underwent concurrent platinum-based chemotherapy. All patients were treated using 3-dimensional conformal radiation therapy; the prescribed dose was delivered to patients on 5 consecutive days/week (6000-7000 cGy, case-dependent, 2 Gy/fraction). Data on the types of nutritional support routes used were also collected. There were 3 types of nutritional support routes during treatment: oral intake (as a reference), nasogastric or percutaneous endoscopic gastrostomy tube feeding, and a combination of oral intake and feeding tube. After completing treatment, patients were followed up via clinic visits every 1 to 3 months for the first year, and then every 3 to 6 months to complete 3 years of follow-up. The intervals gradually increased from 6 months to 1 year after 3 years. The follow-up time was the duration of treatment and 1 month after the completion of treatment.
Statistical Analysis
Statistical analyses were performed using the R Statistical Software (ver. 3.6.2; Foundation for Statistical Computing, The R Foundation). The rate and incidence of hyponatremic events were calculated from the factors of interest. The median follow-up time was reported in person-months (pm) with an interquartile range (IQR). The incidence rate was calculated as the number of events per 1000 pm. To estimate the predictive value of hyponatremic events, the Poisson regression models were used to calculate incident density ratios (IDR) of hyponatremia at 95% confidence intervals (CIs) for each predictor. Univariate and multivariate Poisson regression analyses were used to investigate predictors. Predictors attaining a P ≤ .2 in the bivariate analysis were included in the multivariate analysis. Multivariate regression analysis findings are presented as adjusted P values and adjusted IDR at 95% CI.
Results
Patient Characteristics
Among patients with NPC who received concurrent chemoradiotherapy, 413 were recruited in this study, and 381 patients who met the criteria were included in this analysis. The total follow-up time was 59 354 pm, and the median follow-up time was 164 pm (IQR 135-193). There were 259 patients (68%) who had hyponatremia events. The baseline clinical characteristics of the patients and the incidence rates of hyponatremia are shown in Table 1.
Baseline Patient Characteristics and the Incident Rate of Hyponatremia in Patients With NPC.
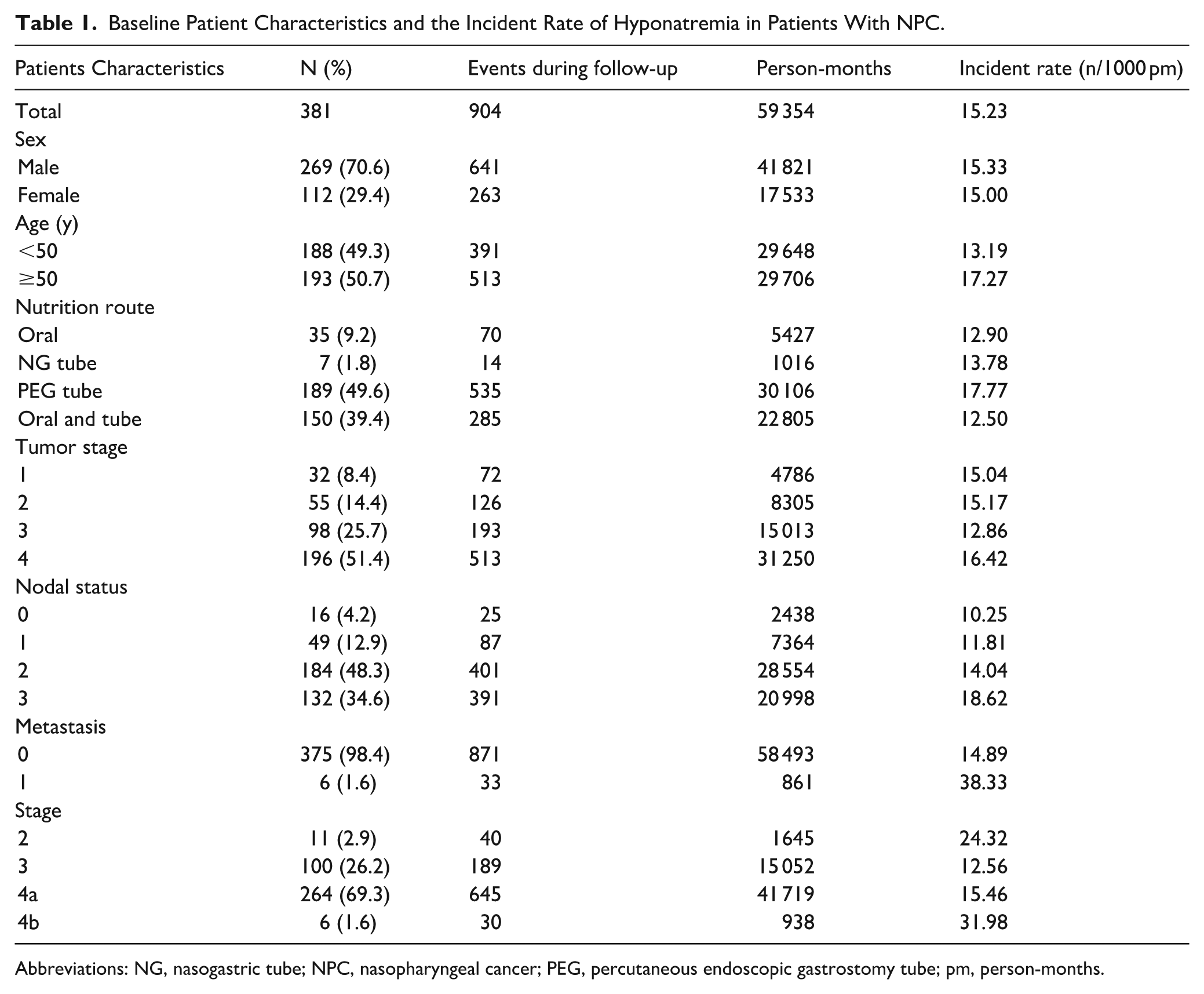
Abbreviations: NG, nasogastric tube; NPC, nasopharyngeal cancer; PEG, percutaneous endoscopic gastrostomy tube; pm, person-months.
Monitoring Hyponatremic Changes Over Time
An analysis of the changes in hyponatremic events over time was conducted, and the findings are shown in Figure 1. The incidence of hyponatremia was the highest within the first 2 months after treatment initiation, with the event density gradually decreasing in subsequent months (Figure 1). The mean serum sodium levels, evaluated at multiple time points following the initiation of treatment, demonstrated an early decline, which was subsequently followed by a progressive increase throughout the treatment course (Figure 2).
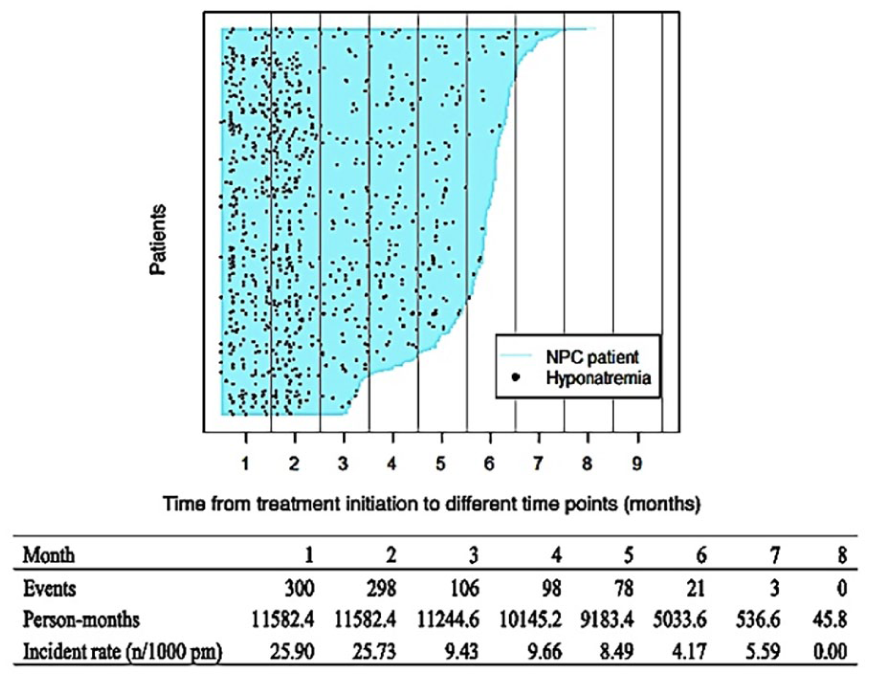
Hyponatremia events in patients with NPC who underwent curative treatment. The patient follow-up time from treatment initiation (blue line) is arranged in descending order. Black dots represent hyponatremia events. NPC, nasopharyngeal cancer; n/1000 pm; number/1000 person-months.
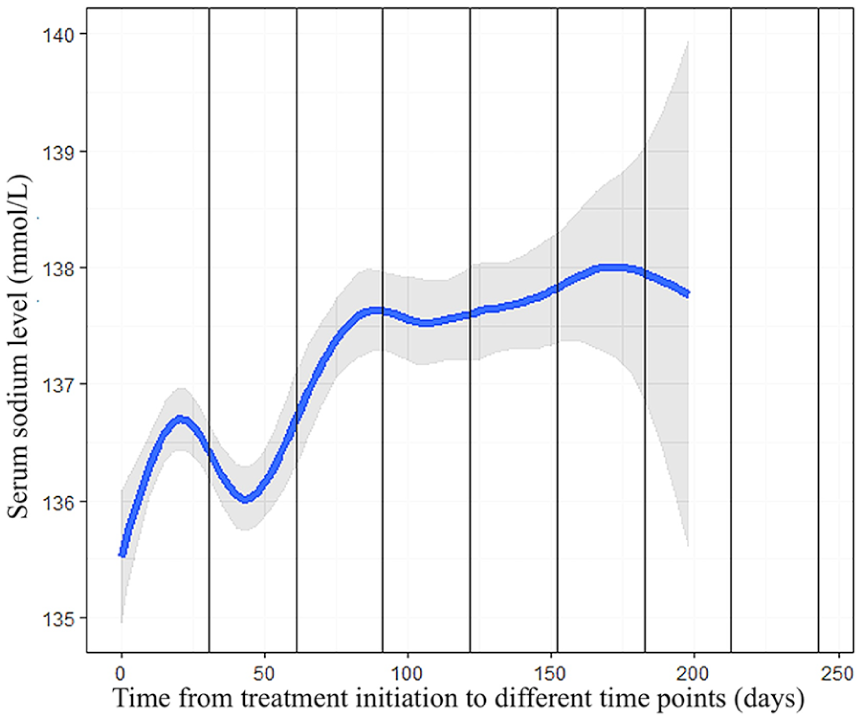
Mean serum sodium levels in nasopharyngeal cancer patients undergoing concurrent chemoradiation, assessed at various time points after treatment initiation.
Poisson Regression Analysis Findings
In the univariate analysis, age, nodal metastasis, distant metastasis, nutritional route, severity of mucositis, and skin complications were significantly associated with hyponatremia in patients with NPC (Table 2). In the multivariate analysis, age, nodal metastasis, distant metastasis, type of chemotherapeutic agent, nutritional route through total tube feeding, severity of mucositis, and skin complications were also independently associated with the development of hyponatremia in patients with NPC (Table 2). Figure 3 shows the trend in serum sodium levels based on the period of NPC treatment according to tumor staging and mucositis grading.
Univariate and Multivariate Poisson Regression Analyses of Hyponatremia in Patients on NPC Treatment.
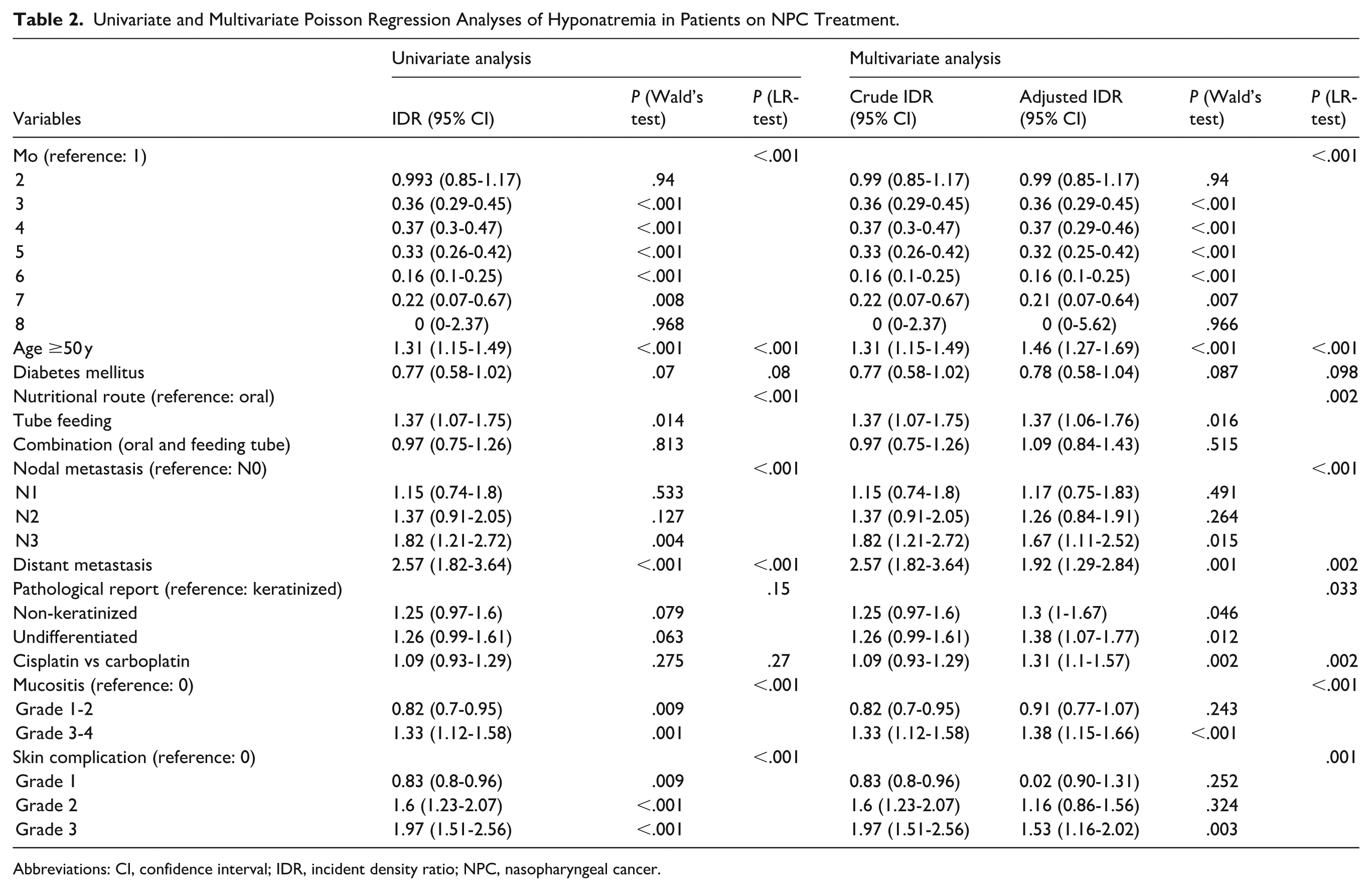
Abbreviations: CI, confidence interval; IDR, incident density ratio; NPC, nasopharyngeal cancer.
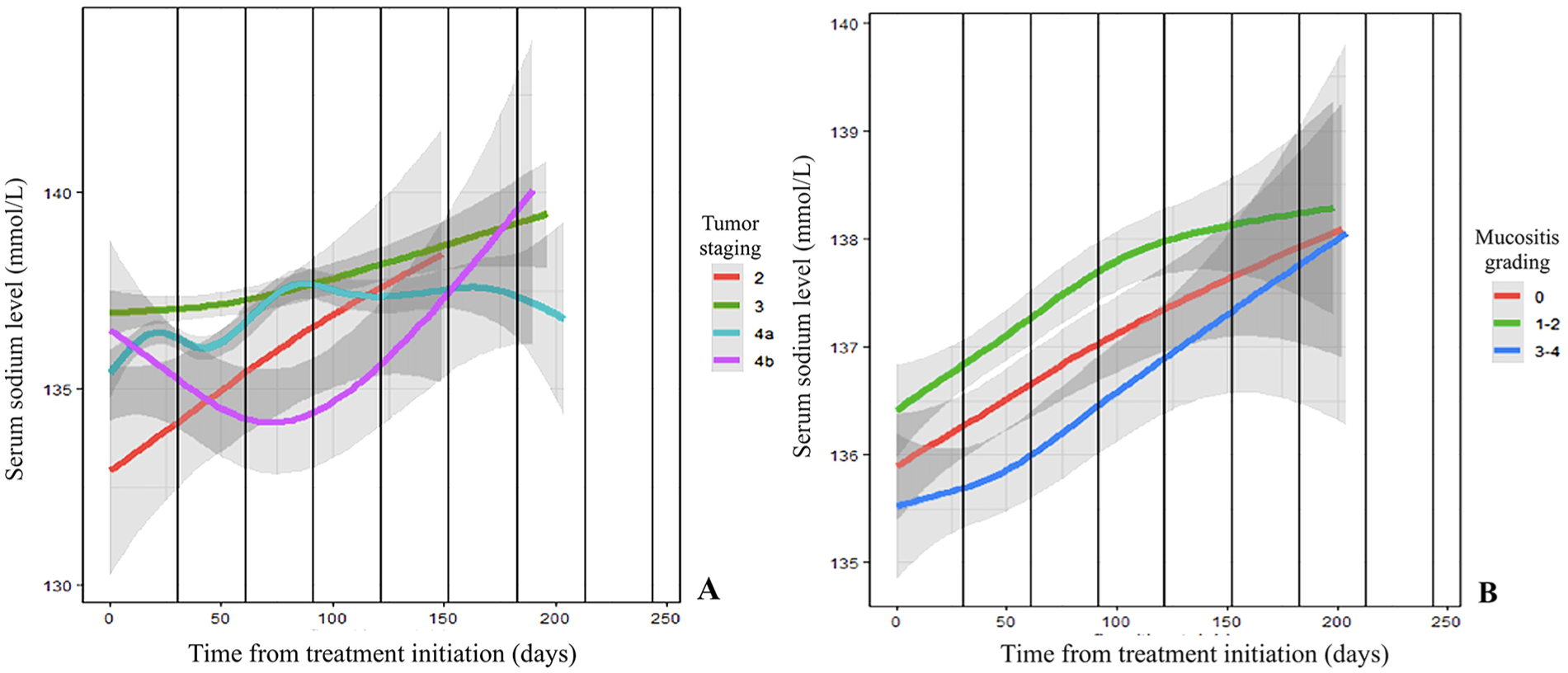
Trend in serum sodium levels based on the period of NPC treatment according to tumor staging and mucositis grading. The regression line indicates serum sodium level based on NPC treatment from initiation, and the shaded areas indicate their 95% confidence intervals according to (A) tumor staging and (B) mucositis grading. NPC, nasopharyngeal cancer.
Discussion
Hyponatremia is one of the most common electrolyte abnormalities in patients with cancer in clinical practice and is associated with advanced or severe disease. 9 Hyponatremia can have several significant consequences in patients with cancer, including longer hospital stay, increased 90-day mortality, 4 and negative prognostic indicator for survival. 10 In case of severe hyponatremia, the symptoms such as lethargy, mental status changes, confusion, seizures, cardiac arrhythmias, or even death can occur. 11 In this study, we mainly focused on hyponatremia in patients with NPC undergoing curative treatment and found that it was observed in 68% of patients. To the best of our knowledge, this is the first study to investigate the changes in hyponatremic events over time in a specific group of patients with NPC. Hyponatremia drastically occurred in the first 2 months after initiating chemotherapy. Physicians must promptly recognize this adverse event; thus, careful monitoring of serum sodium levels with early intensive treatment for hyponatremia can substantially improve patients’ quality of life and avoid several complications. Further investigations are warranted to identify the pathophysiological mechanisms underlying this condition. In our practice, the initial management of hyponatremia prompts the administration of oral sodium tablets and intravenous fluids; fluid restriction; and recommendations for dietary supplements, considering which food has appropriate ingredients that may prevent and recover electrolyte disturbance. However, intractable hyponatremia justifies a nephrologist consultation for further investigation of other hyponatremia etiologies.
Hyponatremia in the context of NPC can arise owing to several factors; some potential causes and considerations are as follows. First, nutritional factors such as malnutrition or dehydration due to disease or treatment can also cause electrolyte disturbances. Optimizing nutrients can help tolerate chemoradiotherapy, which is necessary to achieve the goals of cancer treatment. Enteral tube feeding is required when patients cannot obtain adequate oral nutritional support. Our findings showed that total enteral tube feeding is associated with the risk of hyponatremia, which may be due to the impact of total enteral feeding on swallowing physiology and swallowing-related outcomes, 12 and patients who cannot attain absolute oral intake may have more severe side effects. As reported in the study by Serrano Valles et al, 13 hyponatremia in patients receiving total enteral tube feeding was found to be up to twice as common among those who were malnourished. For these reasons, hyponatremia should still be considered a concern, even in patients receiving total enteral tube feeding. Additionally, oral mucositis is one of the most common side effects of head and neck radiation therapy, with an incidence of 59.4% to 100% and an effect on nutritional status.14,15 Our study found an association between mucositis and hyponatremia. Figure 3 shows the serum sodium levels related to mucositis grading. High-grade oral mucositis is associated with extreme pain, pain while swallowing, and taste alterations that subsequently decrease oral intake and result in poor nutrition, which are the effects of mucositis on nutritional status and subsequent hyponatremia. Second, NPC may lead to syndrome of inappropriate antidiuretic hormone secretion (SIADH), in which excess antidiuretic hormone causes the body to retain water owing to increased reabsorption of free water and diluting serum sodium levels. 11 Talmi et al 16 reported a 3% incidence of SIADH in patients with head and neck cancer, which is higher than previously recognized. Moreover, all reported patients with SIADH in their study had advanced head and neck cancers. This finding is consistent with the results of the present study, which found a significantly associated risk of hyponatremia in patients with advanced nodal and distant metastases.
Third, the tumor may directly or indirectly influence hormonal pathways that regulate the sodium and water balance. A common cause of SIADH is paraneoplastic syndrome, which frequently occurs in patients with lung cancer; however, the syndrome has also been associated with head and neck cancers. 17 The primary NPC tumor increases the secretion of vasopressin, neurophysin, and propressophysin, causing paraneoplastic syndrome that can be pathologically confirmed by NPC tissue testing using both molecular and immunohistochemical studies. 18 Furthermore, the incidence of SIADH following neck dissection in patients with head and neck cancer ranges from 8.14% to 30%. 19 The hypothesis is that the internal jugular vein ligation causes a significant elevation of the intracranial pressure, leading to hormonal release and an increase in serum arginine vasopressin levels. 20 Another important aspect in the association between tumor staging and serum sodium levels is the influence of advanced-stage NPC on the decreasing serum sodium level. According to our regression analysis, hyponatremic events occurred significantly in cases of nodal metastasis, distant metastasis, and advanced tumor staging.
Fourth, treatment-related factors associated with radiotherapy or chemotherapy for NPC may contribute to electrolyte imbalance. Cisplatin is a platinum-based chemotherapeutic agent that is typically used and effective in several types of cancer; it is a key medication for the treatment of patients with NPC. Among the several anticancer agents, platinum-based regimens are frequently reported to be associated with chemotherapeutic agent-induced hyponatremia. The possible mechanism of cisplatin-derived hyponatremia may be the adverse events of cisplatin administration, such as nausea, vomiting, and poor oral intake; moreover, older patients who receive cisplatin with a tendency to develop decreasing renal function are prone to develop hyponatremia, in accordance with our study. 21 A more frequent side effect of cisplatin is nephrotoxicity that decreases glomerular filtration and causes tubular disorders. In addition, the possible mechanisms of cisplatin-derived hyponatremia include SIADH and renal salt-wasting syndrome.22,23 The present study revealed that patients on carboplatin treatment have a much higher associated risk of hyponatremia. Carboplatin is an alternative platinum-based chemotherapeutic regimen for patients with renal insufficiency or cisplatin-induced toxicity. Although the incidence of carboplatin as a cause of hyponatremia development is significantly lower than cisplatin, 24 hyponatremia following carboplatin administration and carboplatin-induced SIADH have also been reported.25,26 In case of cisplatin-induced adverse events, cisplatin has to be reduced in dose or discontinued and then switched to carboplatin. The carboplatin-induced hyponatremia observed in the present study may be attributed to the fact that patients who received carboplatin may have concomitant renal dysfunction or cisplatin toxicity that also increases the risk of hyponatremia, rather than the direct effect of carboplatin itself on hyponatremia. In addition, carboplatin is associated with dehydration, which may cause excess water intake, resulting in serum electrolyte disturbance from the dilutional effect. 26 Radiation therapy causes mucositis and dysphagia that result in insufficient oral intake and hyponatremia. 27 Furthermore, radiation-induced skin reaction is one of the frequent adverse effects of radiation therapy, which has an impact on the pain threshold, wet desquamation, and loss of skin elasticity, 28 exhibiting susceptibility to dysphagia, impaired nutrient intake, or infection. Our study found an association between the degree of skin complications and serum sodium levels; high-grade skin injury from radiation was related to decreased serum sodium levels. Finally, comorbid conditions such as adrenal insufficiency, hypothyroidism, or heart failure can coexist and contribute to hyponatremia.
This study investigated hyponatremia in patients with cancer and provided insights into its occurrence in NPC specifically. Although nutritional management and electrolyte evaluation of patients with NPC should be performed before, during, and after treatment, the findings of the current study help clarify the implementation of appropriate treatment strategies and precise timing for urgent hyponatremia intervention, such as monitoring sodium levels, fluid restriction, medications, sodium supplementation, or dietary recommendations. Thus, a more intense hyponatremia correction intervention is warranted to prevent serious complications. The limitations of the present study include its retrospective nature, which involved a small number of patients, and the fact that an accurate sample size calculation was not performed. Plasma vasopressin concentration, urinary osmolality, and sodium concentration, which are necessary for diagnosing SIADH, have not been fully investigated in all cases; thus, the effect of SIADH could not be evaluated. Future studies should focus on prospective real-time serum sodium monitoring with comprehensive risk identification, intensive management, and long-term follow-up outcomes to improve the care process quality.
Conclusions
Hyponatremia frequently occurs in the first 2 months of NPC treatment. Factors significantly associated with hyponatremia were advanced age, nutritional support via a total enteral feeding tube, advanced nodal metastasis, distant metastasis, carboplatin use, high-grade mucositis, and a high degree of skin injury. These results will be beneficial for the prevention, early detection, monitoring, and appropriate management of hyponatremia in patients with NPC.
Footnotes
Ethical Considerations
The institutional review board of the Faculty of Medicine, Prince of Songkla University, approved this study.
Author Contributions
Peesit Leelasawatsuk: conception, design, and supervision of the study, data analysis and interpretation, manuscript editing, corresponding author, and final approval of the study. Usaporn Prapaisit: data collection and analysis, and final approval of the study. Theepat Wongkittithaworn: data collection and analysis. Yuvatiya Plodpai: data collection and analysis, and final approval of the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Faculty of Medicine, Prince of Songkla University, Thailand; the funding organization had no role in the design or conduct of this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting this study will be available on request at the data owner’s repository via