
Abstract
Purpose:
Laryngeal schwannoma is a rare condition with limited research. This case series presents cases of laryngeal schwannoma in our department with details on the surgical approaches and prognosis of patients, in order to add more evidence for this setting.
Methods:
The patients presented with symptoms that suggested diseases in the throat. These patients were examined by laryngoscopy, magnetic resonance imaging (MRI), and computed tomography (CT). Depending on the tumor size and location, trans-oral endoscopic (laser-assisted) resection, or open laryngeal surgery was applied. The open surgery was modified by splitting the thyroid cartilage plate in the middle (not entering the larynx) and separating the inner surface of the thyroid cartilage plate on the affected side.
Results:
The tumors of all patients were successfully removed. Then, these patients were followed up at the 1st, 3rd, and 6th month after surgery through clinic visits. Laryngoscopy, MRI, and CT were performed to examine the patients, and no recurrences were detected.
Conclusion:
The changes applied for the procedure presented in the present study have the potential to reduce recovery time and scarring, and help preserve throat function. The investigators consider these as potential alternatives to existing methods for treating laryngeal schwannomas. However, more research is required to refine the methods used to treat schwannomas and to ensure that patients receive the best care.
Introduction
Schwannomas are tumors that emerge from benign neoplastic Schwann cells surrounding the nerve fibers. 1 Not much is known on the risk factors for this condition, and the only known factors are radiation exposure and genetics.2,3 In addition, 25% to 45% of schwannomas occur in the head and neck regions.4,5 Furthermore, tumors are often located in the parapharyngeal spaces, while those in the larynx are much more uncommon. Laryngeal schwannomas most frequently occur in women in their fourth or fifth decade of life.6,7 Symptoms associated with laryngeal schwannomas include dysphagia, odynophagia, dysphonia, hoarseness, globus sensation, lateral neck lump, and dyspnea. 6
Once diagnosed, laryngeal schwannomas are commonly treated by completely extirpating the mass, and covering the mucosa using conservative surgery, with the main goal of minimizing the injury to the surrounding regions.8,9 The crucial decision that every surgeon must make when tackling a laryngeal schwannoma is the approach toward the operation, which involves choosing the route of entry, and determining whether to perform a tracheostomy. 10 Some outcome measures for surgery include the presence of postoperative complications or persistent diseases. Unfortunately, due to the rarity of this disease, there is lack of evidence surrounding laryngeal schwannomas, and most of the studies are case reports. In addition, the details of these 2 operation procedures are seldom reported.7,8,11 Therefore, there are almost no established guidelines for treating this disease from which clinicians can refer to. 10 Based on the clinical experience of the investigators, the traditional open surgery therapy was modified, which led to less damage to the regional construction, and a better prognosis. However, there is a need to provide more data on this disease, in order to help future reviewers and policymakers establish scientific and evidence-based guidelines for its management.
In the present study, a surgical approach that differed from traditional procedures was applied. The objective of the present study was to describe the details of the surgical approaches and prognosis of patients under the modified surgery, in order to add more evidence for this setting.
Methods
The present multicenter study conducted a retrospective analysis of consecutive laryngeal schwannoma cases. The present case series was reported in line with the Preferred Reporting of Case Series in Surgery guidelines. 12
Patients
Medical records obtained from the Department of Otolaryngology—Head and Neck Surgery of our hospital were reviewed. Then, consecutive laryngeal schwannomas treated from March 2011 to May 2021 were screened. Since laryngeal schwannoma is an exceedingly-rare disease, all available cases with confirmed pathological diagnosis were included for the case series. The baseline characteristics were collected after the patients were administrated to the ward of our department before the operation. The main items of the collected information are present in Table 1.
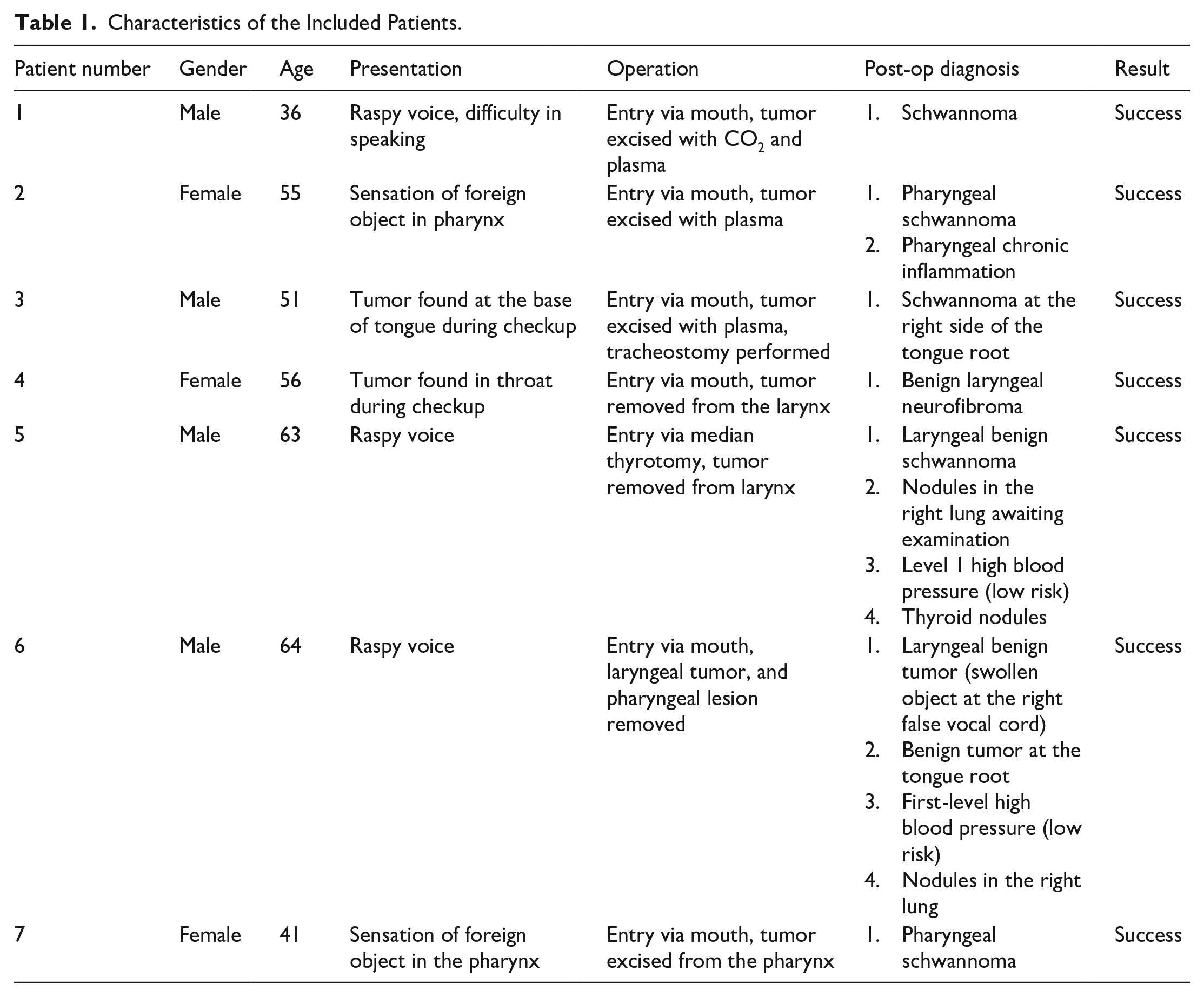
Characteristics of the Included Patients.
Diagnosis
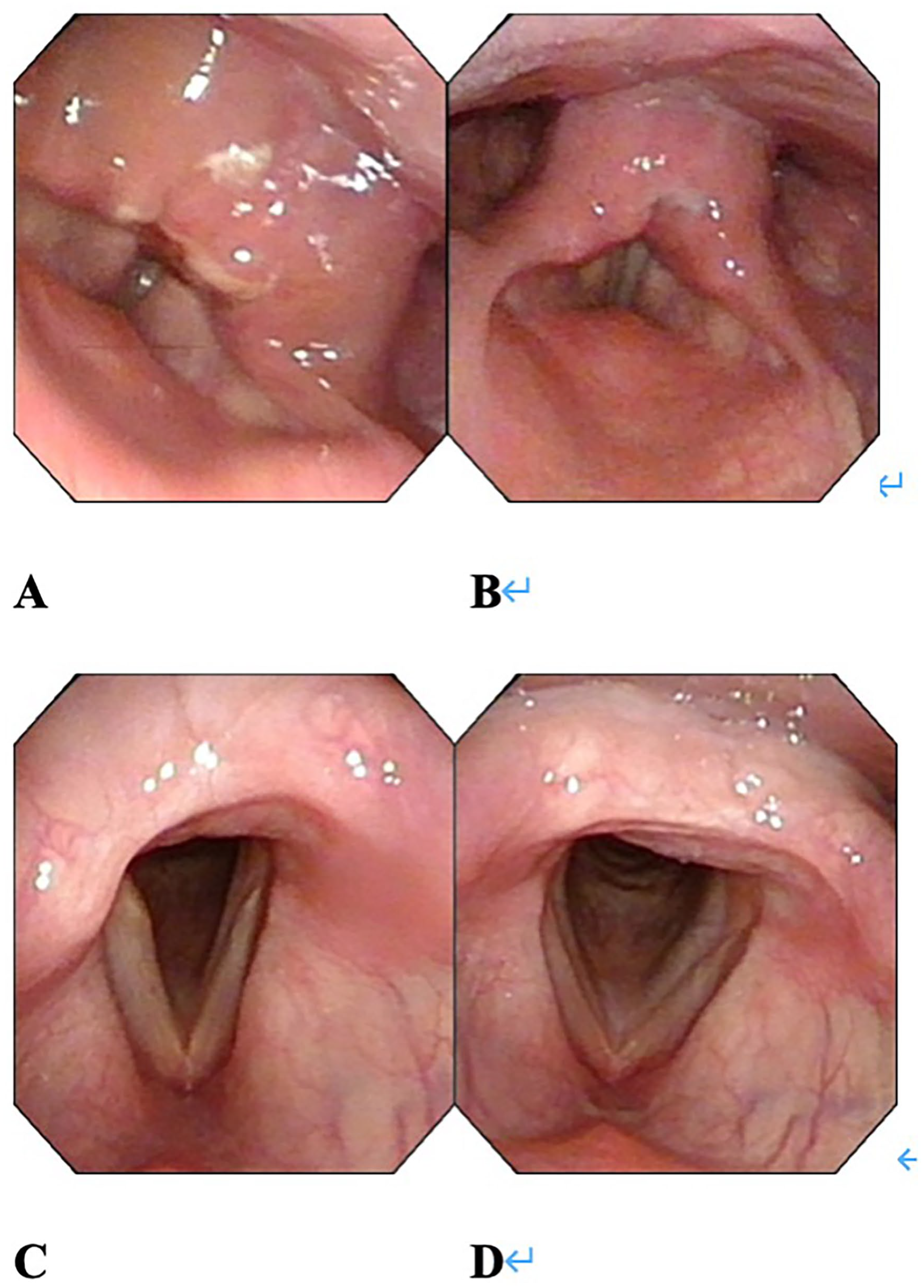
The patient’s initial symptoms (eg, hoarseness, foreign object sensation when swallowing, dyspnea on exertion, and/or dysphagia) were noted on presentation. Then, laryngoscopy was initially performed (Figure 1A and B). Afterward, the patients were scanned by computed tomography (CT) and magnetic resonance imaging (Figure 1C and D). These procedures were performed to locate the tumor and describe its characteristics.
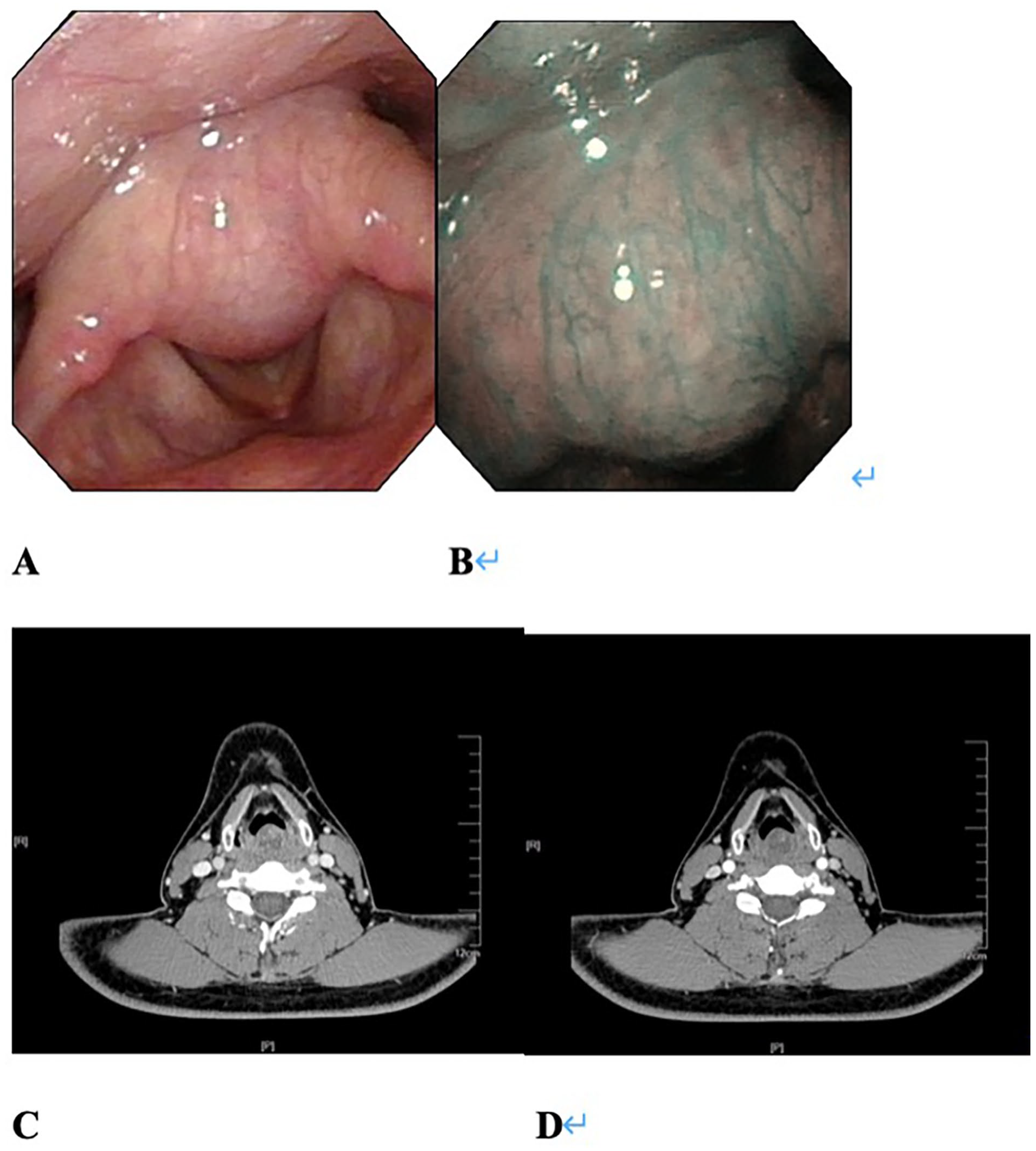
The 36 year-old male patient diagnosed with schwannoma after surgery. (A, B) Taken 3 days before the surgery using an electronic laryngoscope. (B, C) Taken 3 days before the surgery by CT. (A) Presents the large growth in the interarytenoid fold with a smooth surface, as observed using an electronic laryngoscope. Hemorrhage can be observed in the vocal cords, which are mobile. No new growth was observed in the pyriform sinuses. (B) Presents growth with no visible angiogenesis, as observed by narrow band imaging. The growth was ~1.0 × 1.8 cm. (C, D) Presents the growth in the laryngeal cavity, with a diameter of 1.8 cm. The front and sides of the growth were smooth. Radiology notes: growth occupying space in the throat, needs to be combined with laryngoscopy for full diagnosis. CT, computed tomography.
The enhanced CT continuously revealed a rounded lesion with expansive growth and clear boundaries, without the destruction of bone or cartilage structures. The lesions mainly presented as low-density with infiltrative growth and incomplete cystic changes. Occasionally, small flakes of enhancement were observed. The most common sites of laryngeal schwannomas were in the aryepiglottic folds, interarytenoid region, and ventricular zone, but rarely in the vocal cords. This presented with a smooth and raised appearance, and no obvious abnormality with the surrounding mucosa.
It is very difficult to obtain a definite pre-op diagnosis for laryngeal tumors, such as schwannoma. Therefore, the formal diagnosis of schwannoma was only made at post-op, after the biopsy was taken, or after the excised tissue was analyzed (Figures 2 and 3).
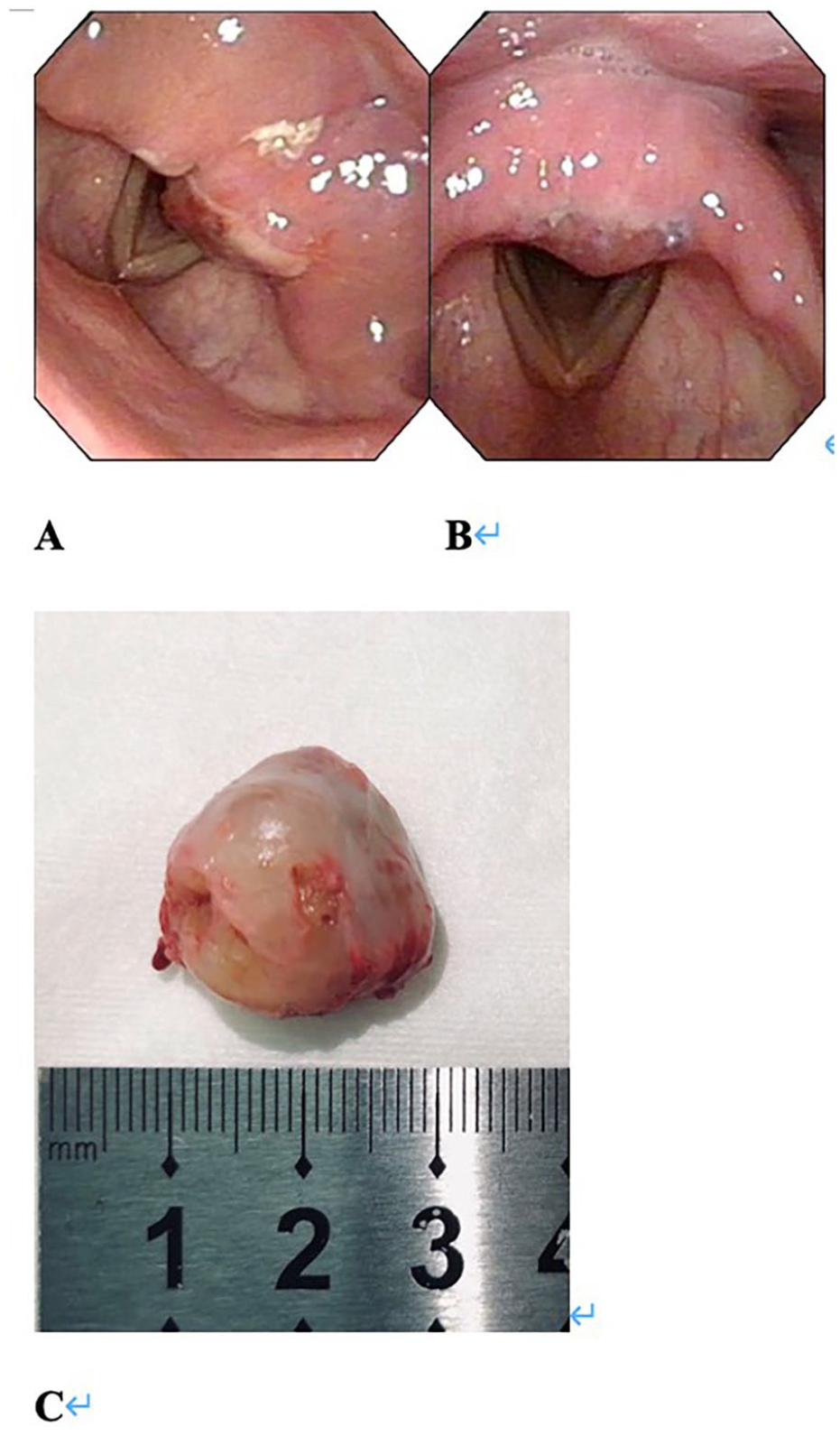
The 36 year-old male patient diagnosed with schwannoma after surgery. (A, B) Taken 1 day after the surgery using an electronic laryngoscope. Both (A, B) present the presence of a pseudomembrane in the laryngeal cavity, with no remaining growth observed. The tumor was ~1.0 × 2.0 cm. The full-excited tumor is presented in (C), with a diameter of 2.0 cm.
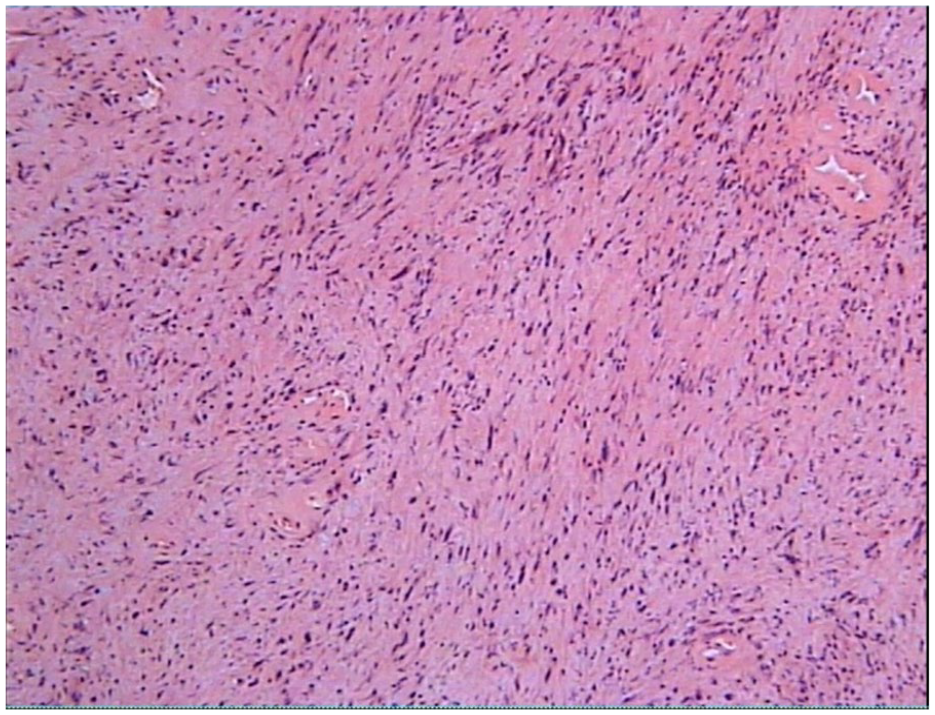
Microscopy: spindle cell neoplasm, localized edema. Laryngeal growth: diagnosed as schwannoma when existing observations were combined with the immunology results. Tumor size: 2.0 × 1.5 × 1.2 cm. Immunology: spindle cell expression; SMA (−), Desmin (−), EMA (−), CD34 (+), CD31 (+), S100 (+++), SOX10 (+++), Ki67 (~5%+).
Interventions
The choice of surgical method depended on the size and location of the tumor, exposure conditions, surgical instruments, and patient preference. There are 2 general surgical approaches: trans-oral endoscopic (laser-assisted) resection, and open laryngeal surgery. For patients with small tumors (size <2 cm) located in the aryepiglottic fold and interarytenoid region of the larynx, endoscopic resection using CO2 laser or/and plasma cutting was generally applied. For patients with small tumors (size <2 cm) located on the vocal cords and above the laryngeal ventricle level, endoscopic resection was applied. For other tumor locations (especially those located near the paraglottic space) or large tumors, open laryngeal surgery was applied.
The patients were operated by different senior surgeons in our department. All involved surgeons were specialized in head, neck, and nose surgery, and all surgeons were in posts equivalent to or higher than a deputy department director. These surgeons had 15 to 20 years of surgery experience, and followed the same rigorous operation instructions in the present study.
No drugs were specifically prescribed to the patients before the operation. Patients with hoarseness and a sensation of a foreign object when swallowing were prescribed with a semi-liquid diet. The remaining patients were allowed to eat in the usual manner. For all cases in the present study, the mucosal membrane that covered the tumor was initially cut open and peeled back, allowing the tumor to be removed alone. Then, the membrane was stitched together using a microsurgical suture to conclude the surgery.
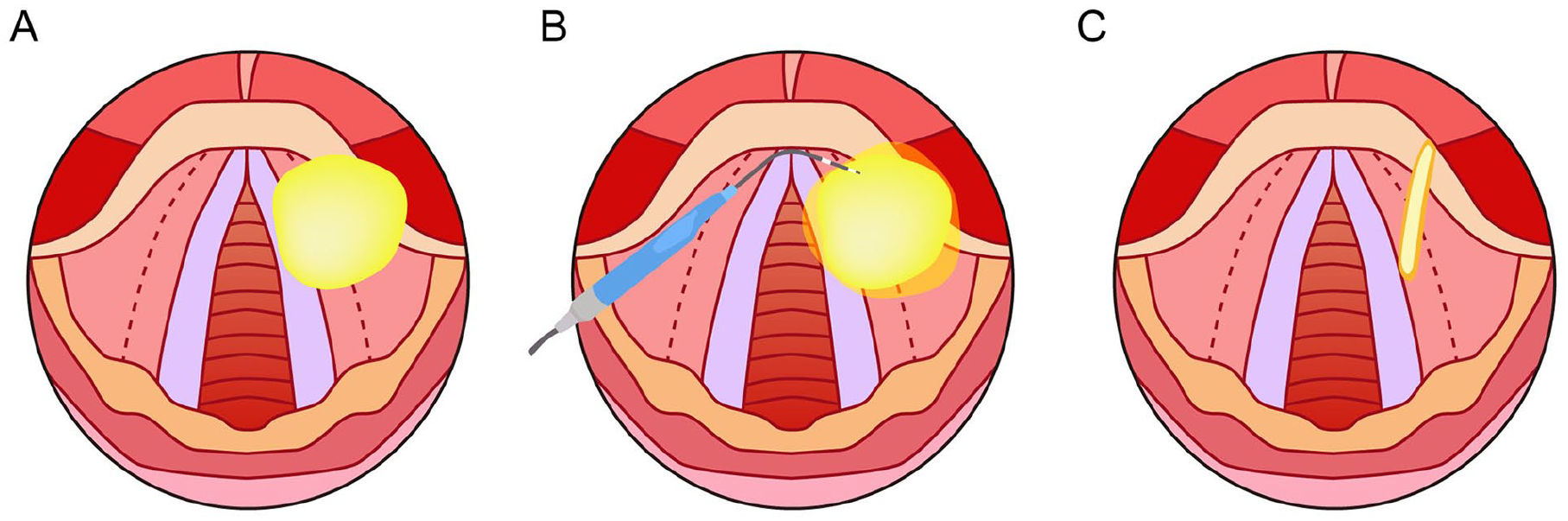
Trans-oral endoscopic (laser-assisted) resection: The patients were placed under general anesthesia at the beginning of the surgery. Then, the laryngoscope was allowed to slowly pass down the throat of the patient, and over the oropharyngeal isthmus, in order to examine the area where the abnormal growth was located. Afterward, the covering of the mucosal membrane was cut open and peeled back before extirpating the tumor (the modification). At this point, the operator has the option of taking a tumor biopsy or excising the entire tumor using cold excision. The obtained tissue was immediately sent for pathological examination for both cases. The operator may decide to excise the tumor only after a biopsy is taken, and this can be performed by entering through the mouth or using an external approach. When the operator visually confirmed that no abnormal tissue was left at the site, the bleeding was stopped using the high-frequency electrosurgical equipment. Then, the mucosa was stitched together using a microsurgical suture to conclude the surgery.
Open laryngeal surgery: Conventional open (trans-cervical) laryngeal surgery usually adopts the laryngeal split and frontal split of the thyroid cartilage plate. At present, operations performed through the thyroid cartilage plate (window) is the most commonly used. The disadvantages of this traditional process are as follows: The location and size of the window needs to be calculated based on the preoperative imaging, and the window often affects the surgical operation. The present open, modified procedure involves the following: Based on the traditional procedure, the thyroid cartilage plate is split in the middle (not entering the larynx), and the inner surface of the thyroid cartilage plate on the affected side is separated, fully exposing the entire paraglottic space. This modified procedure needs to be adjusted according to the location and size of the lesion. At the end of the surgery, the thyroid cartilage plate can be accurately reset and fixed using thick wires, in order to ensure the integrity of the laryngeal stent. At the same time, part of the anterior commissure tendon can be wrapped when threading and fixing the thyroid cartilage plate, in order to provide tension to the vocal cords. This modified procedure requires better surgical instruments, including surgical bone saws and grinding drills.
In practice, the final pathological diagnosis can only be obtained after the operation. The growth found in the throat of each patient was identified as a tumor with different potential origins.
Follow-Up
Each patient was followed up via clinic visits at the department of the investigator. During the follow-up visits, electronic laryngoscope or computer tomography was performed. The visits were scheduled at the 1st, 3rd, and 6th month after the operation.
Results
Patient Characteristics
Seven patients were included for the present study, which comprised of 4 male patients and 3 female patients. The age of these patients ranged within 26 to 64 years old. Two patients presented with no symptoms, 2 patients presented with a raspy voice, 2 patients presented with a sensation of a foreign object in the throat, and 1 patient presented with both a sensation of a foreign object in throat and difficulty in breathing. Furthermore, among the 7 patients, 6 patients received endoscopic (laser-assisted) resection, and 1 patient received open laryngeal surgery.
The chart for the brief description of each individual patient’s relevant characteristics is presented in Table 1. There were no significant deviations from the initial management plan.
Outcomes and Follow-Up
All surgeries were classified as successful by the charts. The patients were followed up at the planned 1st, 3rd, and 6th month after surgery through clinic visits in the department of the investigator. The repeat laryngoscopy and medical imaging revealed no recurrences or further complications. After the sixth month clinic visit, all patients stopped the follow-up visits due to lack of symptoms. An example of the follow-up is presented in Figure 4.
The follow-up of a 36 year-old male patient diagnosed with schwannoma after surgery. (A, B) Present the follow-up images taken at 2 weeks after the surgery using an electronic laryngoscope. There was still a small amount of pseudomembrane present. (C, D) Present the follow-up images taken at the 4th month after the surgery using an electronic laryngoscope. There were no apparent abnormalities. The patient recovered well after the surgery.
Complications and Adverse Events
Besides the small amount of bleeding during the operation, none of the patients experienced any complications or adverse events after the surgery.
Discussion
Laryngeal schwannoma is a relatively-rare disease, and the literature on laryngeal schwannoma mostly consists of case reports. 6 The present cases were treated by excising the tumor using micro-laryngoscopy or open surgery approaches. All 7 patients included in the present study recovered well after the surgery without any complications. Furthermore, no recurrence or other new surgery-related adverse events occurred during the follow-up.
As discussed in the study conducted by Wong et al, 6 almost all cases of laryngeal schwannoma were treated by completely excising the tumor. There are 2 main routes of entry for excising a schwannoma: entry via the patient’s mouth and entry via an external approach. The entry route is chosen based on a variety of factors, such as tumor size, tumor location, exposure of the tumor, and patient preference.
For trans-oral endoscopic (laser-assisted) resection, when extirpating tumors, the traditional approach generally involves excising the entire tumor along with the surrounding mucosal membrane.4,13 The investigators suggest cutting open and peeling back the covering mucosal membrane before extirpating the tumor. This modification of the operation can minimize injury, decrease bleeding, and speed up recovery without compromising the long-term results. However, the changes to the procedure should be examined and considered as a potential alternative procedure.
For the open surgery approach, Wong et al presented a variety of different options when determining how to create an opening to the tumor via an excision in the neck. External approaches are frequently used on larger tumors, and generally offer “better access and better visualisation of the lesion.” 6 Different techniques for entry have been advocated, and each has its unique strengths and weaknesses. When tackling entry via the open (trans-cervical) approach, the investigators prefer an incision in the middle of the thyroid cartilage without entering the larynx. By going along the inner side of the thyroid cartilage, the tumors located at the glottis and false vocal cords can be exposed. After extirpating the tumor, the cartilage can be resecured by punching small holes in the cartilage and securing the cartilage along with the surrounding tissue using dissolvable strings. Based on the experience of the investigators, this approach can help preserve the throat’s function and structure and prevent the peeling of the mucosal membrane.
Strengths
Since laryngeal schwannoma is a relatively-rare disease, and most published literature on this subject involves case reports that feature singular cases, the present study contributes a comparatively-large block of data toward the treatment of this disease.
Weaknesses and Limitations
Although the present study features novel approaches in operating for laryngeal schwannomas, it remains difficult to establish the differences in outcome with existing approaches. As reported by Wong et al, 6 most laryngeal schwannoma patients successfully recover without recurrences or further complications. However, more minute details on surgical outcomes, such as wound size and speed of recovery, were not well-documented on the charts of patients.
Conclusion
The present case series demonstrates a procedure for treating laryngeal schwannomas that differ from traditional methods in 2 ways. The changes in the procedure have the potential to reduce recovery time and scarring and help preserve throat function. The investigators consider this approach as a potential alternative to existing methods for treating laryngeal schwannomas. Efforts should be made to provide more evidence for the treatment of laryngeal schwannomas, in order to refine the methods used to treat schwannomas and to ensure that patients receive the best care.
Footnotes
Ethical Considerations
The study protocol was approved by the Ethics Committee of Nanjing Drum Tower Hospital and was guided by local policy, national laws, and the World Medical Association Declaration of Helsinki.
Consent to Participate
Oral informed consent was obtained from all participants.
Author Contributions
Conceptualization: Xiaoyun Qian, Ao Li, and Yajun Gu; data curation: Zheng Liang, Yajun Gu, and Hao Wei; formal analysis: Zheng Liang and Yajun Gu; funding acquisition: Xiaoyun Qian and Ao Li; investigation and methodology: Yajun Gu, Junguo Wang and Hao Wu; project administration: Yajun Gu, Junguo Wang, Hao Wei and Hao Wu; resources: Xiaoyun Qian and Ao Li; software: Hui Li; supervision: Xiaoyun Qian and Ao Li; validation: Zheng Liang and Yajun Gu; visualization: Zheng Liang and Yajun Gu; roles/writing—original draft: Zheng Liang, Yajun Gu, and Hao Wei; writing—review and editing: Xiaoyun Qian, Ao Li, and Yajun Gu.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Clinical Trials from the Affiliated Drum Tower Hospital, Medical School of Nanjing University (2024-LCYJ-MS-02).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.