
Abstract
Objective:
To investigate the changes in tinnitus among patients with chronic otitis media (COM) before and after tympanoplasty.
Methods:
A literature search was conducted using the PubMed, EMBASE, and Web of Science electronic databases. Patients with COM alone and preoperative tinnitus who underwent tympanoplasty (with or without ossiculoplasty) and had their tinnitus outcomes evaluated using the Tinnitus Handicap Inventory (THI), the Visual Analogue Scale (VAS), or self-reported symptom changes were included. Patients with concurrent cholesteatoma or those who underwent mastoidectomy were excluded. Meta-analyses of THI scores and self-reported symptom changes were performed using the random-effects model.
Results:
Out of the 134 articles identified, 9 studies with 483 patients were included. Ossiculoplasty was performed when necessary in 3 studies. The THI was used in 5 studies, with mean changes in scores ranging from −24.00 to +1.40. Three studies were included in the meta-analysis, which showed a mean difference of −3.93 (95% confidence interval (CI): −8.61 to 0.76; P = .10). The VAS was used in 3 studies, with mean changes in scores ranging from −3.35 to −0.10. Self-reported symptom changes were recorded in 4 studies, involving 231 patients. After surgery, tinnitus disappeared in 77 (33.33%) patients, was alleviated in 96 (41.56%) patients, remained unchanged in 45 (19.48%) patients, and deteriorated in 13 (5.63%) patients. In the meta-analysis, the weighted proportions were 42.63% (95% CI: 20.43%-66.52%), 41.17% (95% CI: 27.26%-55.85%), 13.28% (95% CI: 4.36%-26.06%), and 3.86% (95% CI: 0.70%-9.41%), respectively.
Conclusion:
Although the majority of patients with COM and concurrent tinnitus experienced a reduction in tinnitus severity following tympanoplasty, the meta-analysis did not demonstrate a significant improvement in THI scores. Further multicenter prospective studies are needed to identify the prognostic factors, given the high heterogeneity in patient characteristics and operative methods across the current studies.
Introduction
Chronic otitis media (COM) is an inflammatory disease affecting the middle ear and mastoid. Persistent infections can lead to tympanic membrane perforation and even ossicular chain disruption, resulting in conductive hearing loss. 1 COM may also cause symptoms such as tinnitus, vertigo, and otorrhea, and is sometimes associated with cholesteatoma. 2 Tinnitus is defined as the perception of sound without an external source and is often closely associated with hearing loss. 3 Lesions in the peripheral auditory pathway—such as the tympanic membrane or middle ear—can influence central auditory processing, potentially leading to tinnitus. 4 Therefore, resolving peripheral lesions may help alleviate tinnitus. 5 Tympanoplasty should be considered when tympanic membrane perforation persists despite medical treatment or when hearing loss is present. 4 Its primary goal is to reconstruct the tympanic membrane and restore middle ear function. 6 Recent studies report hearing improvement in over 70% of COM patients following tympanoplasty. 7 Erkorkmaz et al also found that patients whose tinnitus decreased or disappeared after surgery reported significantly higher satisfaction. 2 Several studies have demonstrated tinnitus improvement after tympanoplasty or middle ear surgery in patients with COM or cholesteatoma, using questionnaires such as the Tinnitus Handicap Inventory (THI) and Visual Analogue Scale (VAS).4,6,8-16 However, systematic reviews investigating tinnitus changes before and after tympanoplasty in COM patients are lacking. Therefore, this systematic review and meta-analysis aimed to identify the impact of tympanoplasty on tinnitus improvement in patients with COM.
Materials and Methods
Search Strategy
This systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO; ID: CRD42024629050) and conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 17 As this study involved a review of previously published data, institutional review board approval and informed consent were not required. Two authors (K.-T.Y. and T.-W.Y.) performed an electronic literature search across 3 databases—PubMed, EMBASE, and Web of Science—to identify articles for inclusion on December 20, 2024. The following keywords were used in the search: “tinnitus,” AND “chronic otitis media,” AND “tympanoplasty” OR “middle ear surgery.” Titles and abstracts were independently screened by K.-T.Y. and T.-W.Y., with any discrepancies resolved through discussion with the other 2 authors (B.-Y.Z. and K.-C.C.).
Eligibility Criteria
Inclusion criteria were as follows: (1) prospective or retrospective studies involving COM patients with preoperative tinnitus who underwent tympanoplasty; (2) tinnitus outcomes assessed using the THI, VAS, or self-reported symptom changes (including tinnitus disappearance, alleviation, no change, or deterioration), and (3) articles published in English. Exclusion criteria were as follows: (1) review articles or case reports, (2) patients with concurrent cholesteatoma or those who underwent mastoidectomy, and (3) studies with non-extractable or insufficient tinnitus outcome data.
Data Extraction
Full-text reviews were conducted for all eligible articles. The following data were extracted and analyzed: first author, year of publication, number of tinnitus patients in the original study and in this review, diagnosis, operative methods, preoperative and postoperative THI and VAS scores, and self-reported symptom changes. Audiological outcomes—including preoperative and postoperative air-bone gaps (ABGs), air conduction (AC), and bone conduction (BC) thresholds—were also collected.
Statistical Analysis
In this review, clinically meaningful change was defined as 7.0 points for the THI and 1.5 points for the VAS. 18 A meta-analysis comparing mean preoperative and postoperative THI scores was performed using RevMan version 5.4.1 (Cochrane Collaboration, London, UK) with a random-effects model, reporting the mean difference and 95% confidence interval (CI). In addition, a meta-analysis of proportions for self-reported symptom changes was conducted using MedCalc Statistical Software version 23.0.2 (MedCalc Software Ltd, Ostend, Belgium), calculating weighted proportions with 95% CIs under a random-effects model. Heterogeneity was assessed using the I2 statistic for both analyses.
Assessments of Risk of Bias and Quality of Evidence
Two authors (K.-T.Y. and T.-W.Y.) independently assessed risk of bias using the ROBINS-I V2 tool for non-randomized studies and the RoB 2 tool for randomized controlled trials. ROBINS-I V2 evaluates 7 domains, with judgments categorized as “low,” “moderate,” “serious,” or “critical” risk. 19 RoB 2 evaluates 5 domains, rated as “low risk of bias,” “some concerns,” or “high risk of bias.” 20 Overall risk of bias was also determined for each study. In addition, the quality of evidence for each outcome was independently evaluated using the GRADE approach, with certainty rated as “high,” “moderate,” “low,” or “very low.” 21 Disagreements were resolved through discussion with the other 2 authors (B.-Y.Z. and K.-C.C.).
Results
Study Selection and Characteristics
A total of 172 articles were identified through searches of PubMed, EMBASE, and Web of Science, with 38 duplicates removed. After screening titles and abstracts, 98 articles were excluded, and 2 could not be retrieved despite extensive efforts. Of the remaining 34 articles, 14 were excluded for not being in English, 1 for being a review article, 7 due to the presence of cholesteatoma, 2 for non-extractable data, and 1 for insufficient data. Ultimately, 9 articles were included in the analysis (Figure 1).4-6,11,13-16,22 The characteristics of these 9 studies are summarized in Table 1.
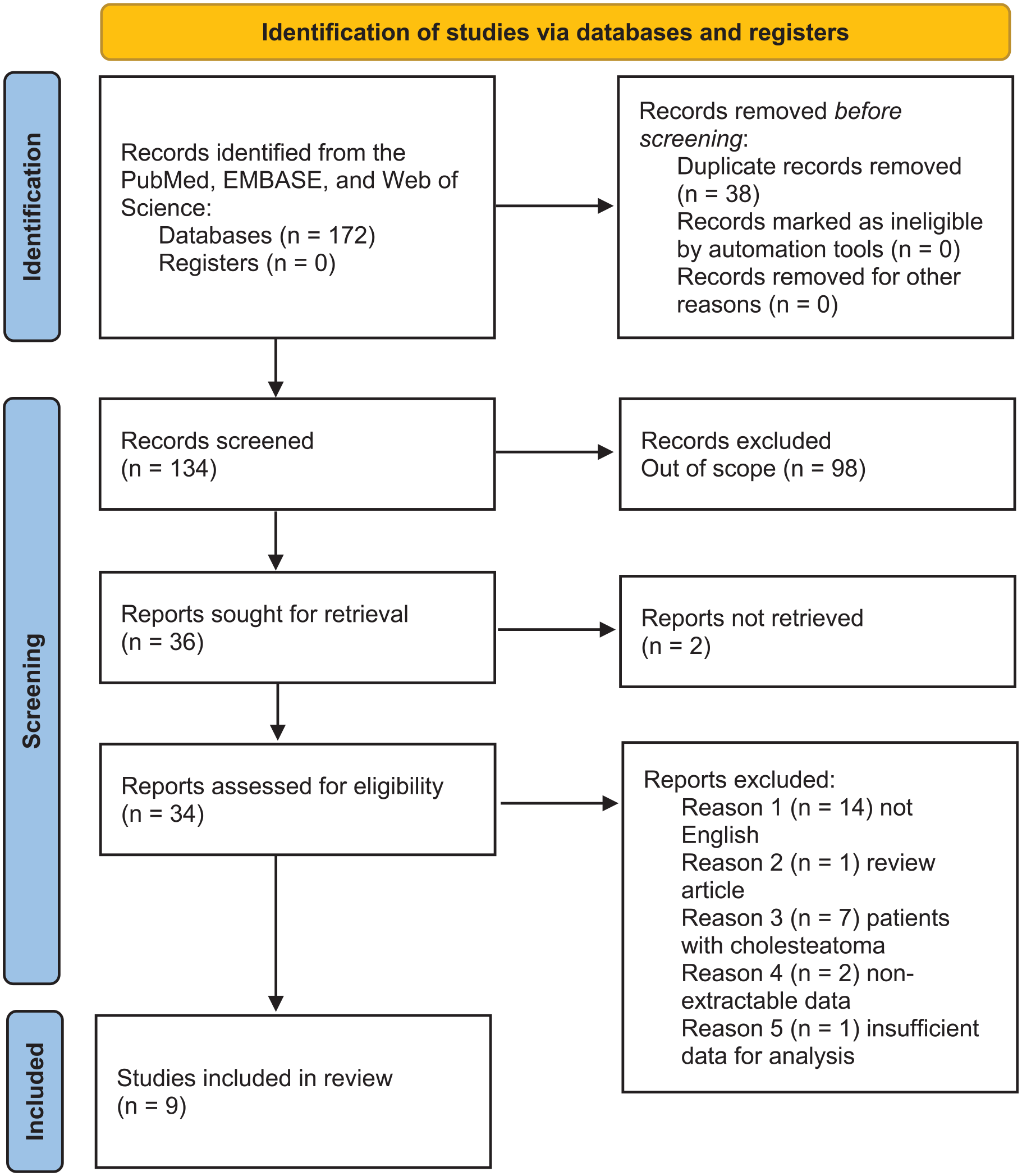
PRISMA flow diagram illustrating the study selection process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of the Included Studies.
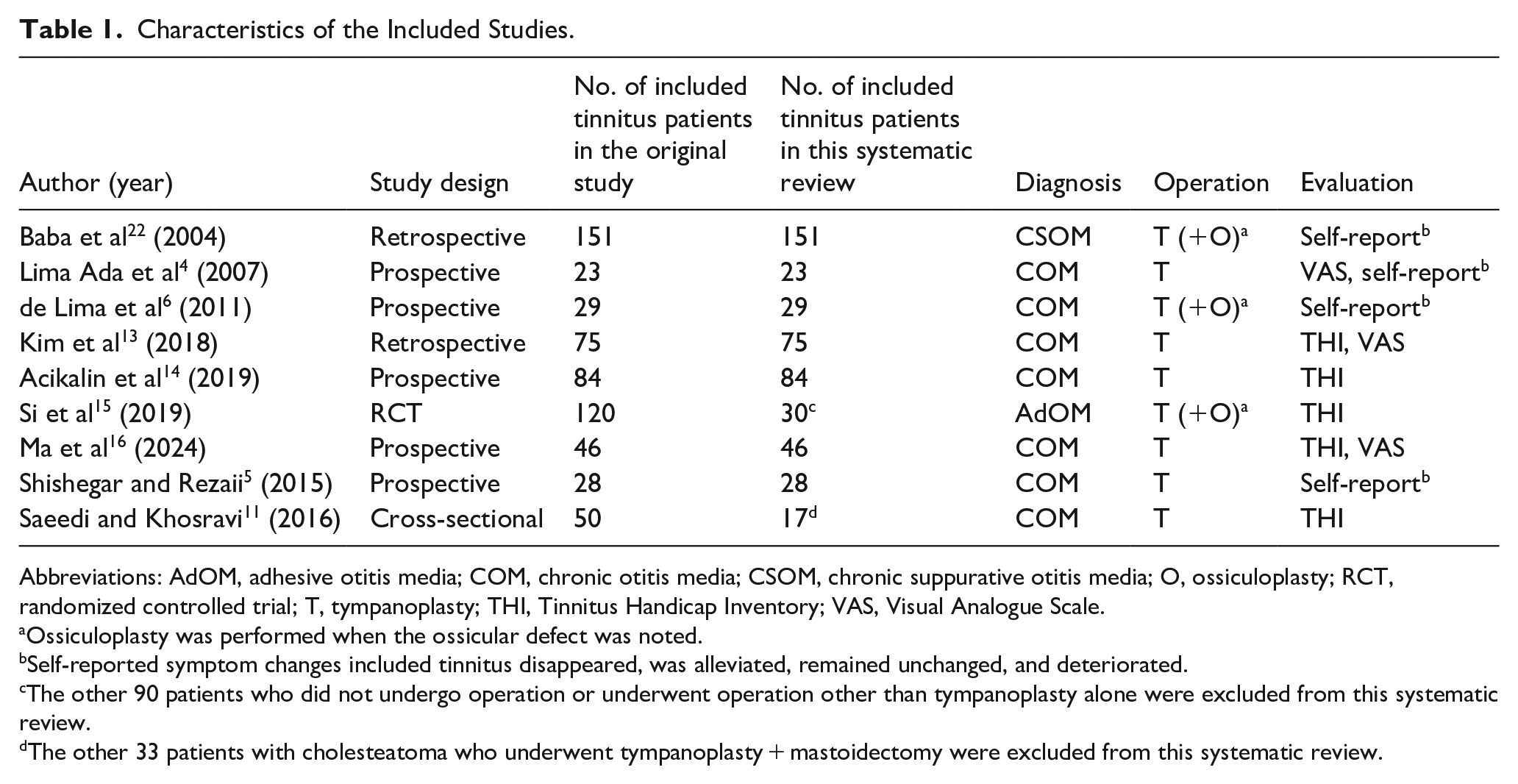
Abbreviations: AdOM, adhesive otitis media; COM, chronic otitis media; CSOM, chronic suppurative otitis media; O, ossiculoplasty; RCT, randomized controlled trial; T, tympanoplasty; THI, Tinnitus Handicap Inventory; VAS, Visual Analogue Scale.
Ossiculoplasty was performed when the ossicular defect was noted.
Self-reported symptom changes included tinnitus disappeared, was alleviated, remained unchanged, and deteriorated.
The other 90 patients who did not undergo operation or underwent operation other than tympanoplasty alone were excluded from this systematic review.
The other 33 patients with cholesteatoma who underwent tympanoplasty + mastoidectomy were excluded from this systematic review.
Tinnitus Outcomes
This systematic review included 483 patients with preoperative tinnitus and COM who underwent tympanoplasty. Among them, 151 had chronic suppurative otitis media (CSOM) 22 and 30 had adhesive otitis media (AdOM). 15 Ossiculoplasty was performed when necessary and reported in 3 studies.6,15,22 Follow-up durations ranged from 2 months to 2 years. The THI and VAS were used in 511,13-16 and 34,13,16 studies, respectively, with the VAS specifically assessing tinnitus-related discomfort, intensity, disturbance, or severity. All studies reported significant postoperative improvement in tinnitus (P < .05) using the THI or VAS, except 1 that found no improvement in patients (n = 23) with a preoperative ABG ≤15 decibels (dB). 13 Four studies reported mean changes in THI scores, ranging from −24.00 to +1.40 (Table 2).11,13,15,16 In a randomized controlled trial, Si et al found significantly lower postoperative THI scores in the tympanoplasty group compared to controls. 15 Two studies did not provide both preoperative and postoperative THI scores.11,14 A meta-analysis of the remaining 3 studies showed a numerical improvement in THI scores, with a mean difference of −3.93 (95% CI: −8.61 to 0.76; I2 = 46%), though this was not statistically significant (P = .10; Figure 2).13,15,16 Three studies reported mean changes in VAS scores, ranging from −3.35 to −0.10 (Table 3).4,13,16 However, 1 study did not provide standard deviations for preoperative and postoperative VAS scores, 4 and due to limited data, a meta-analysis could not be performed on the remaining 2 studies.13,16 Self-reported symptom changes were documented in 4 studies, involving 231 patients (Table 4).4-6,22 Postoperatively, tinnitus disappeared in 77 (33.33%), was alleviated in 96 (41.56%), remained unchanged in 45 (19.48%), and deteriorated in 13 (5.63%) patients. Meta-analysis showed weighted proportions of 42.63% (95% CI: 20.43%-66.52%; I2 = 90%) for disappearance, 41.17% (95% CI: 27.26%-55.85%; I2 = 73%) for alleviation, 13.28% (95% CI: 4.36%-26.06%; I2 = 78%) for no change, and 3.86% (95% CI: 0.70%-9.41%; I2 = 55%) for deterioration (Figure 3).
THI Outcomes of the Included Studies.
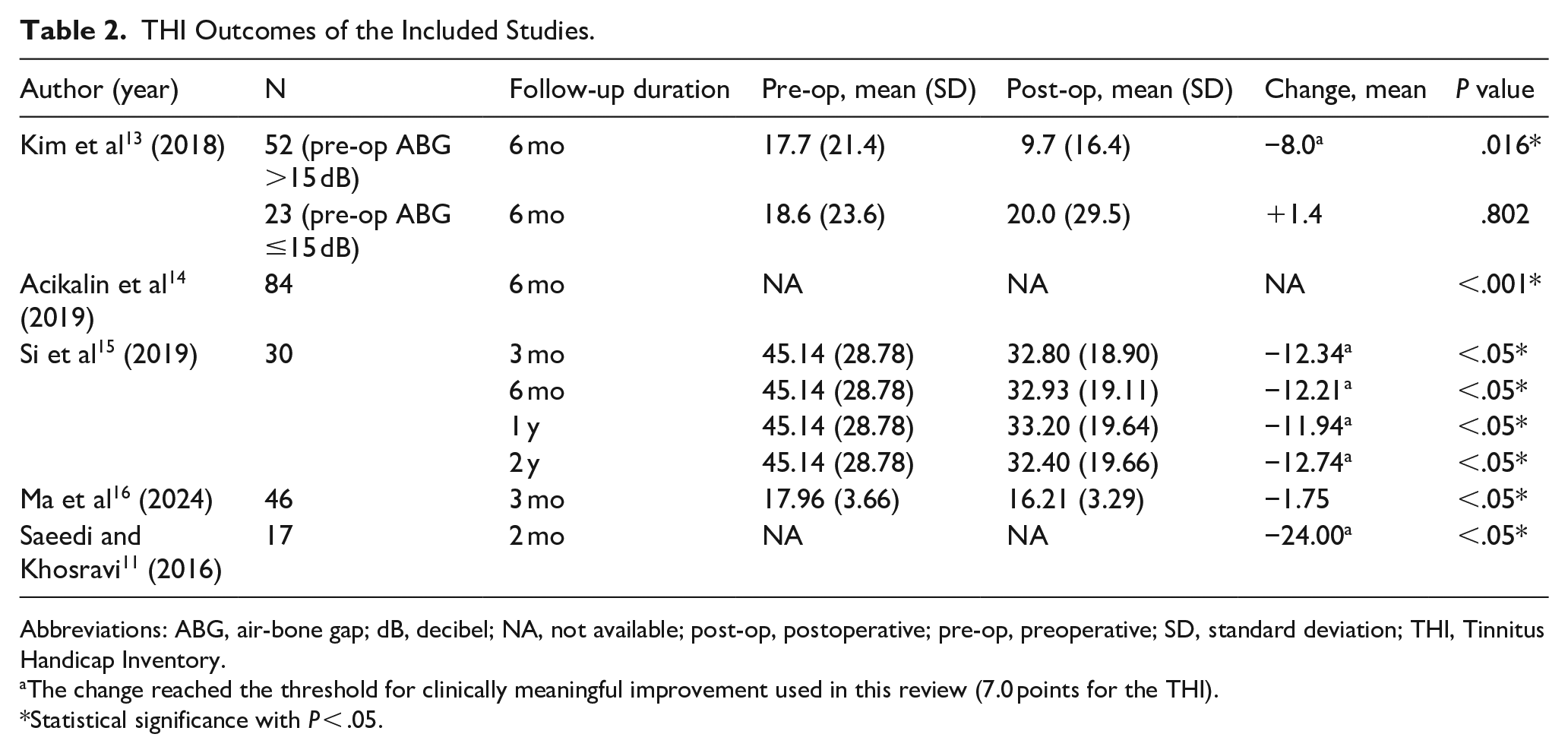
Abbreviations: ABG, air-bone gap; dB, decibel; NA, not available; post-op, postoperative; pre-op, preoperative; SD, standard deviation; THI, Tinnitus Handicap Inventory.
The change reached the threshold for clinically meaningful improvement used in this review (7.0 points for the THI).
Statistical significance with P < .05.

Forest plot of the meta-analysis comparing preoperative and postoperative THI scores. CI, confidence interval; IV, inverse variance; post-op, postoperative; pre-op, preoperative; THI, Tinnitus Handicap Inventory.
VAS Outcomes of the Included Studies.
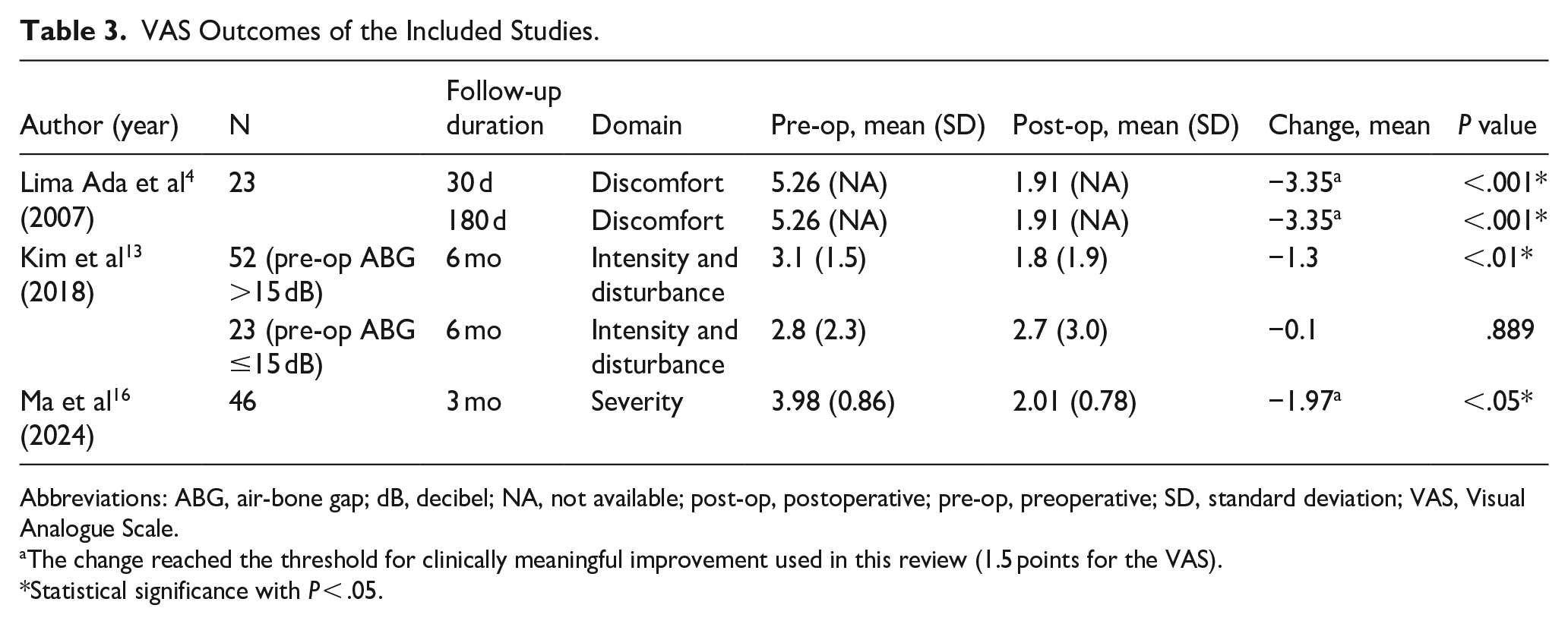
Abbreviations: ABG, air-bone gap; dB, decibel; NA, not available; post-op, postoperative; pre-op, preoperative; SD, standard deviation; VAS, Visual Analogue Scale.
The change reached the threshold for clinically meaningful improvement used in this review (1.5 points for the VAS).
Statistical significance with P < .05.
Self-Reported Symptom Changes of the Included Studies.
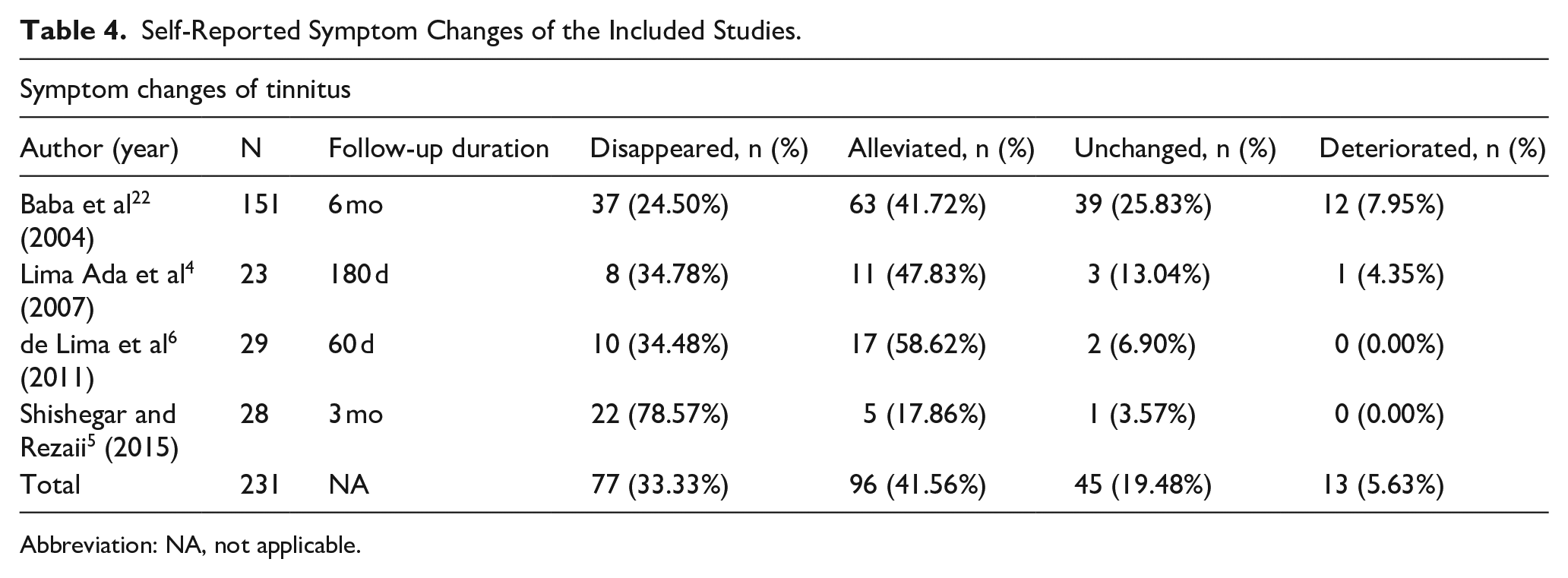
Abbreviation: NA, not applicable.
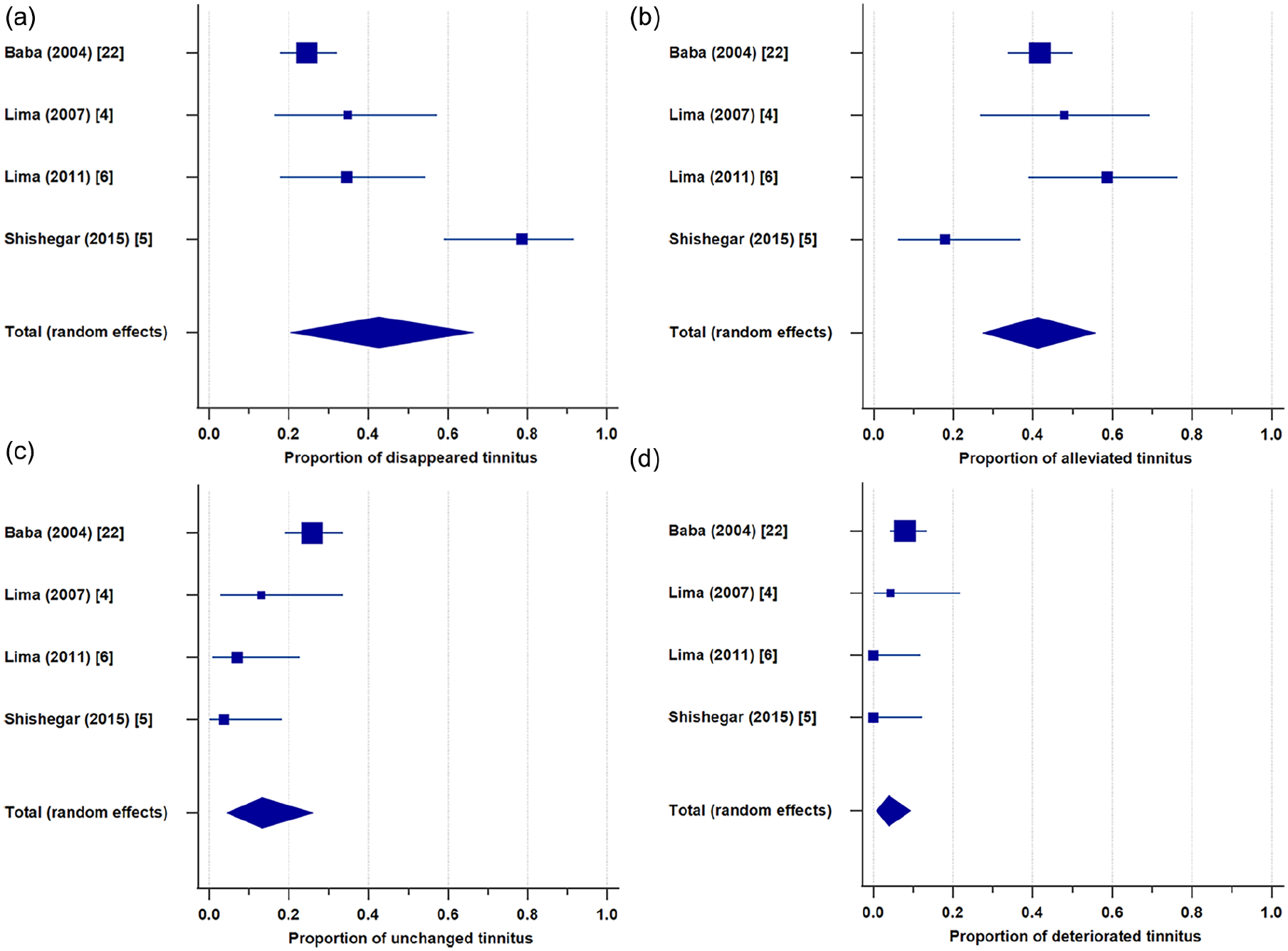
Forest plot of the meta-analysis showing weighted proportions of self-reported symptom changes in tinnitus. Tinnitus (a) disappeared, (b) was alleviated, (c) remained unchanged, or (d) deteriorated after tympanoplasty.
Audiological Outcomes
Preoperative and postoperative ABGs were collected from 6 studies,4,5,11,13,15,16 while AC and BC thresholds were available in 3.11,13,16 Detailed audiological outcomes are summarized in Table 5. Three studies examined the correlation between tinnitus and audiological outcomes.11,13,16 One study of 55 COM patients with preoperative tinnitus and ABG ≥15 dB found no significant correlation between the reduction in ABG and THI score (P = .054) or VAS score (P = .139). 13 Another study of 50 patients (17 with COM alone, 33 with cholesteatoma) found significant correlations between the reduction in ABG and THI score (P = .018), as well as between the reduction in AC threshold and THI score (P = .036). However, there was no significant correlation between the reduction in BC threshold and THI score (P = .060). 11 The other study comparing tinnitus (n = 46) and non-tinnitus (n = 40) groups found no statistically significant differences in ABGs, AC, or BC thresholds. 16 On the other hand, Si et al reported significantly lower postoperative ABG in the tympanoplasty group compared to controls in a randomized controlled trial. 15
Audiological Outcomes Collected From the Included Studies.
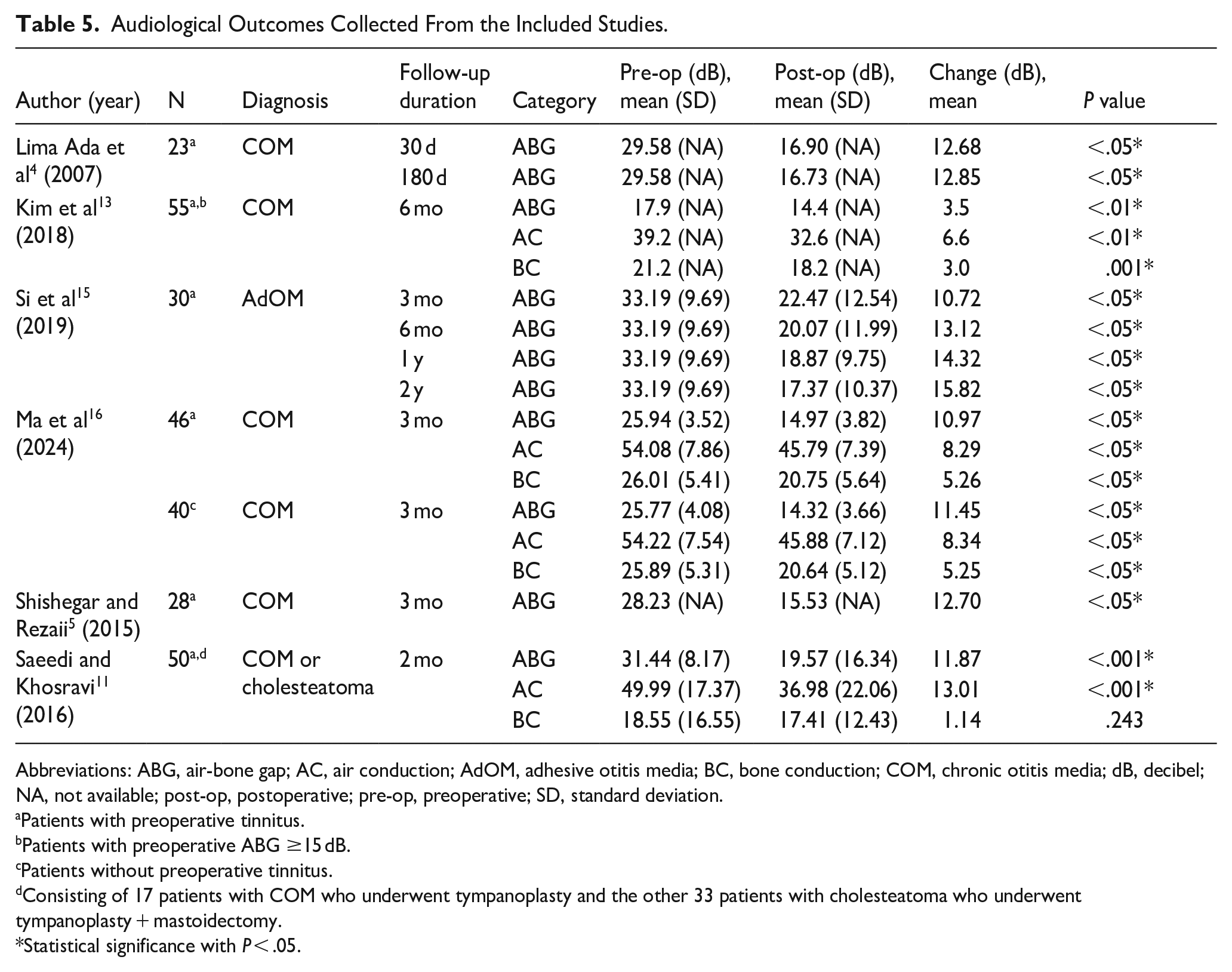
Abbreviations: ABG, air-bone gap; AC, air conduction; AdOM, adhesive otitis media; BC, bone conduction; COM, chronic otitis media; dB, decibel; NA, not available; post-op, postoperative; pre-op, preoperative; SD, standard deviation.
Patients with preoperative tinnitus.
Patients with preoperative ABG ≥15 dB.
Patients without preoperative tinnitus.
Consisting of 17 patients with COM who underwent tympanoplasty and the other 33 patients with cholesteatoma who underwent tympanoplasty + mastoidectomy.
Statistical significance with P < .05.
Assessments of Risk of Bias and Quality of Evidence
All 8 non-randomized studies were rated as having a moderate overall risk of bias, primarily due to the observational study design, which led to a moderate risk of bias arising from measurement of the outcome.4-6,11,13,14,16,22 Baba et al 22 and de Lima et al 6 did not specify the number of patients who underwent both tympanoplasty and ossiculoplasty, while Lima Ada et al 4 and de Lima et al 6 reported that procedures were performed by different surgeons. These 3 studies were thus classified as having a moderate risk of bias due to confounding. The only randomized controlled trial was rated as having some concerns due to the lack of information on whether the analysis followed a pre-specified plan. 15 Detailed risk of bias assessments are presented in Supplementary Tables 1 (non-randomized studies) and 2 (randomized controlled trials). The THI and VAS outcomes were graded as low quality of evidence due to serious risk of bias, serious inconsistency, and serious imprecision. The outcomes of self-reported symptom changes were graded as very low quality of evidence due to serious risk of bias, very serious inconsistency, and serious imprecision. Detailed quality of evidence assessments are presented in Supplementary Table 3.
Discussion
This systematic review demonstrated the tinnitus outcomes in patients with COM alone who underwent tympanoplasty, excluding those with concurrent cholesteatoma or who underwent mastoidectomy to reduce variability in patient characteristics and surgical procedures. Most included studies reported significant improvements in THI and VAS scores postoperatively. However, meta-analysis of THI scores did not show a statistically significant reduction, and VAS data were insufficient for meta-analysis. The relationship between hearing improvement and changes in THI or VAS scores also remained unclear. While outcomes of self-reported symptom changes showed that tinnitus disappeared or was alleviated in 74.89% of patients, 5.63% reported deterioration of symptoms after tympanoplasty.
The Role of Tympanoplasty in COM Patients
COM is typically associated with conductive hearing loss due to tympanic membrane perforation or ossicular chain disruption. 23 However, it can also lead to sensorineural hearing loss, as inflammatory mediators from the middle ear may damage the inner ear. 24 Although COM patients often present with hearing loss and otorrhea, 4 tinnitus may sometimes be their most troubling symptom. 11 The incidence of tinnitus in COM patients has been reported to range from 32.65% to 56.76%.2,8,10,12,14,16,22,25 Several mechanisms may explain the relationship between hearing restoration and tinnitus improvement. One theory suggests that hearing loss reduces afferent input to the central auditory pathways, leading to hypersensitivity in the cochlear nuclei and the perception of tinnitus. Tympanoplasty may reduce tinnitus by restoring the tympanic membrane and middle ear function, thereby enhancing afferent stimulation. 4 Another explanation is that improved hearing increases ambient sound levels, which may partially or fully mask tinnitus. 26 Kalaycık et al also found that both tinnitus and vertigo improved after middle ear surgery in COM patients, likely due to the resolution of middle ear inflammation. 10 Baba et al used the VAS to assess overall satisfaction in CSOM patients after tympanoplasty and found it was associated with improvements in hearing, tinnitus, vertigo, and otorrhea. 22 Similarly, Erkorkmaz et al reported that hearing restoration and the resolution of tinnitus, vertigo, and otorrhea significantly influenced patient satisfaction. 2 In addition, Acikalin et al found that COM patients whose tinnitus did not improve postoperatively had significantly higher levels of depression. 14 These findings suggest that alleviating associated symptoms through tympanoplasty can enhance quality of life in COM patients.
THI and VAS
All included studies that used the THI or VAS to assess tinnitus outcomes reported significant score reductions after tympanoplasty,4,11,14-16 except 1, which found no significant changes in patients with a preoperative ABG ≤15 dB. 13 Reported mean improvements ranged from 1.75 to 24.00 for THI and 1.30 to 3.35 for VAS scores. Several other studies—including those with cholesteatoma patients or COM patients who underwent mastoidectomy—also examined the effects of middle ear surgery (eg, myringoplasty, tympanoplasty, ossiculoplasty, or mastoidectomy) on tinnitus using the THI or VAS.8,11,12 All 3 reported significant postoperative improvement in tinnitus (P < .05) when comparing preoperative and postoperative scores. The mean improvement in THI ranged from 12.10 to 36.69, and in VAS from 1.50 to 4.16. Saeedi and Khosravi compared the THI score reduction between COM patients who underwent tympanoplasty and those who underwent tympanoplasty + mastoidectomy. They found a significantly smaller reduction in THI scores in the tympanoplasty group, though the reason for this was unclear. 11 By contrast, another study involving COM and cholesteatoma patients—excluded from this review—found no significant difference in THI improvement among the simple tympanoplasty, tympanoplasty + canal-wall-up mastoidectomy, and tympanoplasty + canal-wall-down mastoidectomy groups. 12
In summary, most studies reported significant tinnitus improvement after tympanoplasty or middle ear surgery in patients with COM or cholesteatoma, as measured by the THI or VAS. However, the degree of THI and VAS score reduction varied widely across studies. In this review, the meta-analysis showed a numerical reduction in THI score (−3.93) but did not reach statistical significance. Several factors may explain this result. First, only 3 studies were included in the meta-analysis, limiting the number of participants and reducing the ability to detect significant differences. In addition, Saeedi and Khosravi reported a substantial THI reduction (−24.00), 11 greater than the range seen in the included studies (−12.74 to +1.40).13,15,16 However, their data were excluded due to insufficient preoperative and postoperative details, which may have affected the overall result. Heterogeneity was another contributing factor, as indicated by an I2 value of 46%. Variations in patient characteristics and operative methods likely led to inconsistent outcomes. Therefore, larger and more standardized studies are needed to clarify the effect of tympanoplasty on tinnitus and to identify which patients are most likely to benefit.
Self-Reported Symptom Changes
Four studies included in this review, totaling 231 patients, reported self-reported symptom changes.4-6,22 Tinnitus disappeared in 33.33%, was alleviated in 41.56%, remained unchanged in 19.48%, and deteriorated in 5.63% of patients. Several other studies—including those with cholesteatoma patients or COM patients who underwent mastoidectomy—also recorded self-reported symptom changes after middle ear surgery, with a combined total of 173 patients.2,11,12,27 Among them, tinnitus disappeared in 26.59%, was alleviated in 52.02%, remained unchanged in 20.23%, and deteriorated in 1.16%. The data suggest that ~75% to 80% of COM or cholesteatoma patients experienced either disappearance or alleviation of tinnitus following tympanoplasty or middle ear surgery. This trend was further supported by the meta-analysis in this review, which showed that over 80% of patients reported reduced tinnitus severity. However, the high heterogeneity (I2 = 55%-90%) warrants cautious interpretation. Such variability may stem from differences in patient characteristics, surgical techniques, or follow-up durations across studies. Future research should aim to standardize these factors to improve comparability and reliability. In addition, subgroup analyses or sensitivity testing may help identify patient populations most likely to benefit from tympanoplasty.
Audiological Outcomes and Tinnitus Improvement
Si et al conducted a randomized controlled trial in patients with AdOM and found that both the mean postoperative ABG and THI scores were significantly lower in the tympanoplasty group compared to the control group. They also concluded that medical treatment alone was ineffective in relieving tinnitus symptoms. 15 Kim et al suggested that preoperative ABG might predict tinnitus outcomes after tympanoplasty in COM patients. However, they found no significant correlation between ABG reduction and changes in either THI or VAS scores. Their findings also indicated that patients with COM and mild hearing loss may have a lower likelihood of tinnitus improvement, and they recommended alternative treatments such as sound therapy for these individuals. 13 Saeedi and Khosravi found significant correlations between reductions in ABG and THI scores, as well as between reductions in AC threshold and THI score; however, these results included patients who underwent tympanoplasty with mastoidectomy. 11 Two additional studies—excluded from this review—also examined the relationship between audiological outcomes and tinnitus improvement in patients with COM or cholesteatoma who underwent middle ear surgery.8,12 Both studies divided patients into 2 groups based on THI score reduction, using cutoff values of 10 and 20, respectively. They found that greater THI reduction was significantly associated with improved AC thresholds, but not with ABG. Neither study found significant differences in preoperative or postoperative ABGs, AC, or BC thresholds between groups. Kim et al further explored the correlation between hearing improvement and THI score reduction but found no significant association, attributing the result to the multifactorial nature of tinnitus generation, detection, and perception. 8 On the other hand, Ma et al reported no significant differences in preoperative or postoperative audiological outcomes between the tinnitus and non-tinnitus groups. 16 Therefore, the role of audiological outcomes in predicting postoperative tinnitus improvement remains unclear based on current evidence.
Limitations
This systematic review has several limitations. The number of included studies was relatively small, and not all were prospective in design. Restricting inclusion to English-language articles introduces potential selection bias. Clinical heterogeneity across studies—such as differences in patient selection, operative methods, surgical techniques, follow-up duration, and outcome measures—also increases the risk of bias. Although tinnitus-related measures, such as the THI and VAS, were used, available data were insufficient for a meta-analysis of VAS outcomes. High heterogeneity in the meta-analyses of THI and self-reported symptom change outcomes (I2 = 46%-90%) further weakens the strength of the findings. Subgroup or sensitivity analyses to explore the sources of heterogeneity were not feasible due to the limited number of studies. These factors contributed to the GRADE assessment of low quality of evidence for THI and VAS outcomes and very low quality of evidence for self-reported symptom changes. Collectively, these limitations highlight the need for larger, multicenter, prospective studies to more accurately assess the impact of tympanoplasty on tinnitus outcomes.
Conclusions
Although ~75% of COM patients with concurrent tinnitus may experience a reduction in tinnitus severity following successful tympanoplasty, some show no change or even worsening. Moreover, the meta-analysis in this review did not find a statistically significant improvement in THI scores following surgery. To better identify prognostic factors for tinnitus outcomes and provide more reliable guidance during preoperative consultations, future research should focus on well-designed studies with larger sample sizes, longer follow-up, and clearly defined inclusion and exclusion criteria.
Supplemental Material
sj-docx-1-ear-10.1177_01455613251342954 – Supplemental material for The Impact of Tympanoplasty on Tinnitus Improvement in Patients With Chronic Otitis Media: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-ear-10.1177_01455613251342954 for The Impact of Tympanoplasty on Tinnitus Improvement in Patients With Chronic Otitis Media: A Systematic Review and Meta-Analysis by Kuan-Ting Yeh, Bang-Yan Zhang, Ta-Wei Yeh and Kai-Chieh Chan in Ear, Nose & Throat Journal
Footnotes
Ethical Considerations
Ethics approval from the institutional review board was not required for this study, as it is a systematic review of previously published data.
Consent for Publication
Informed consent was not required for this study, as it is a systematic review of previously published data.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The relevant data of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.