
Abstract
Objective:
We investigated the incidence of sensorineural hearing loss (SNHL) after chronic otitis media (COM) surgery and determined the associated factors.
Methods:
Data were collected via retrospective medical chart review.
Results:
Of the 192 patients, 82 underwent tympanoplasty, 26 underwent canal wall up mastoidectomy with tympanoplasty, and 84 underwent canal wall down mastoidectomy with tympanoplasty. After surgery, the average air conduction (AC) hearing threshold improved significantly, from 125 to 1000 Hz, but the average high-frequency AC and bone conduction (BC) hearing thresholds deteriorated significantly. In 21 (11%) cases, the BC hearing threshold worsened by more than 15 dB at 4000 Hz. When we compared these 21 cases to patients in whom hearing was preserved, the former group was found to be significantly younger and had a higher frequency of cholesteatomatous otitis media. However, when comparing the severity of inflammation in patients with temporal bone computed tomography, there was no significant difference between the 2 groups.
Conclusions:
High-frequency SNHL may develop after surgery to treat COM, especially in young patients with cholesteatoma.
Introduction
After surgery to treat chronic otitis media (COM), patients sometimes experience sensorineural hearing loss (SNHL), which is profound in about 1% of cases. 1 Unlike other complications of COM surgery, profound SNHL poses significant problems for both patients and surgeons, and recovery is not possible. Ossicular damage and mastoid drilling are associated with SNHL, but the mechanisms remain unknown. 1 -3 Few relevant reports have appeared, SNHL is relatively uncommon, and traditional COM surgery attracts less research interest than newer surgeries such as cochlear implantation. We determined the rate of SNHL in patients after COM surgery and identified associated factors, where the ultimate aim is to prevent SNHL.
Patients and Methods
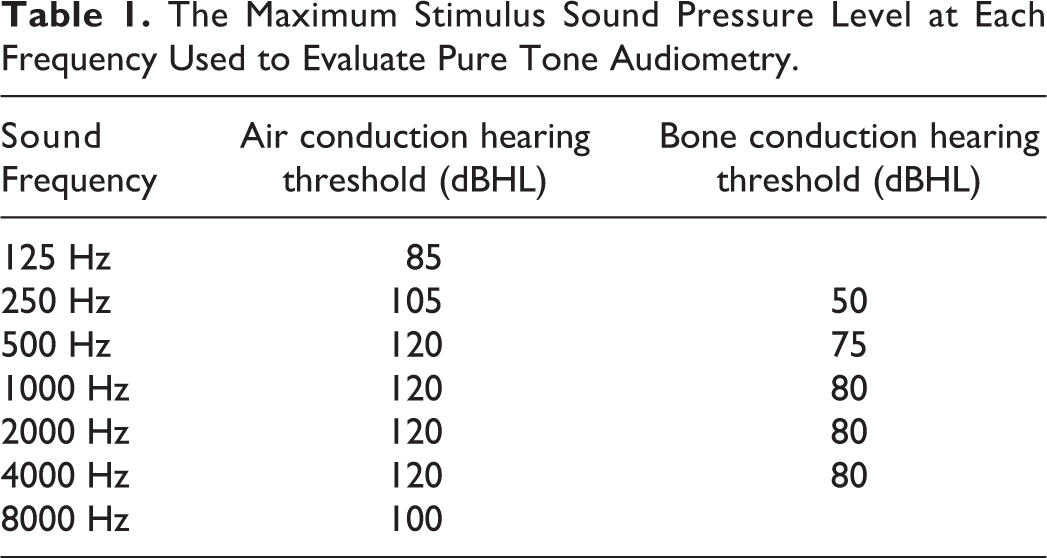
We reviewed the medical records of patients who underwent COM surgery at Daejeon St. Mary’s Hospital between 2012 and 2016 and were followed-up for more than 1 year. Patients with an unmeasurable hearing threshold for any frequency in preoperative hearing data because of severe hearing loss were excluded. In addition, during the postoperative follow-up period, patients with events that could damage the patient’s hearing, including chemotherapy, were excluded from the study. We ultimately enrolled 192 patients. All patients were diagnosed with cholesteatomatous otitis media (ChOM) or noncholesteatomatous otitis media (NChOM) based on otoscopy, temporal bone computed tomography (CT), and cholesteatoma status during surgery. We decided what kind of surgery to perform on the patient, considering the following. When the preoperative temporal bone CT showed a soft tissue density of 25% or more in the air cells of the mastoid and the antrum, mastoidectomy was performed. In NChOM patients, when the contracted mastoid was shown and the entire antrum and aditus ad antrum were filled with soft tissue density in temporal bone CT, the patient’s Eustachian tube function was judged to be very poor and a canal wall down mastoidectomy (CWDM) was performed. And in ChOM patients, the type of surgery was determined according to the degree of cholesteatoma involvement. Pure-tone audiometry tests were performed before and at 3 months after surgery, and the differences were quantified. If a patient’s hearing threshold at some frequencies became unmeasurable after surgery, the unmeasurable hearing threshold was recorded after adding 5 dB to the maximum output level of the audiometer at that frequency. The maximum output levels at each frequency are shown in Table 1. For example, if the patient’s air conduction hearing threshold became unmeasurable at 1000 Hz, it was actually recorded as 125 dBHL. We determined differences in hearing parameters before versus after surgery (especially any decrease in the bone conduction [BC] hearing threshold) and explored the clinical factors involved, including cholesteatoma status, the operation method and time, ossiculoplasty and first/revision surgery status, and inflammation severity (as determined by temporal bone CT). The extent of inflammation was scored from 0 to 2 in the middle ear, aditus ad antrum, and antrum (0, 1, and 2 for 25%, 50%, and >50%, respectively); the maximum score was 6 points (Figure 1).
The Maximum Stimulus Sound Pressure Level at Each Frequency Used to Evaluate Pure Tone Audiometry.
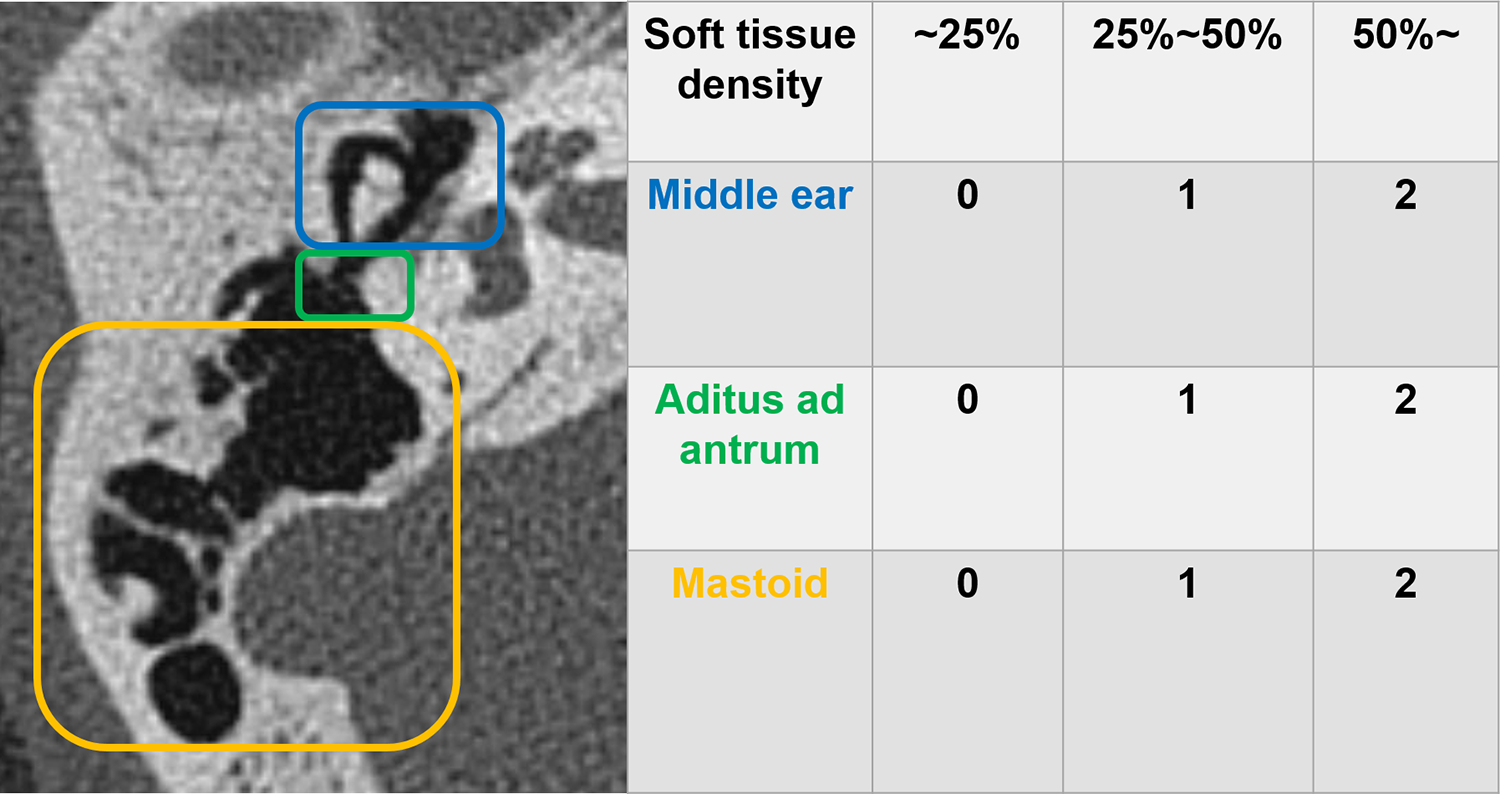
Inflammation severity score determination by temporal bone computed tomography (CT). The extent of inflammation was scored from 0 to 2 in the middle ear, aditus ad antrum, and antrum. According to the degree of soft tissue density at each site, 0 points were given for soft tissue density of less than 25%, 1 point for 25% to 50%, and 2 points for 50% or more.
Statistical Analysis
The χ2 test was used to analyze categorical variables, and the independent t test was employed to analyze continuous variables. We used SPSS software (ver. 20.0; SPSS Inc) for the analyses; P values <.05 were considered statistically significant.
Ethics Statement
The study protocol was reviewed and approved by the institutional review board of the Catholic University Hospital (DC20RISI0014); the need for informed consent was waived.
Results
The mean patient age was 51.1 ± 15.7 years and the mean follow-up duration was 2.5 ± 1.0 years (Table 2). Noncholesteatomatous otitis media (135 patients) was more common than ChOM (57 patients); 82 patients underwent tympanoplasty, 26 underwent canal wall up mastoidectomy (CWUM) with tympanoplasty, and 84 underwent CWDM with tympanoplasty. Postoperatively, low-frequency (125-1000 Hz) conduction hearing improved significantly, but at high frequencies both the air and BC thresholds deteriorated significantly, indicative of SNHL (Table 3). The worsening in BC hearing threshold was greater at 4000 than 2000 Hz; we thus explored the relationship between the hearing decrease at 4000 Hz and various clinical factors. We focused on patients with a worsened BC hearing at 4000 Hz. Among all patients, 102 exhibited no such worsening, but 69 cases showed hearing loss of 5 to 10 dB, and 21 loss of more than 15 dB (Figure 2).
Demographic and Clinical Characteristics of All Patients.
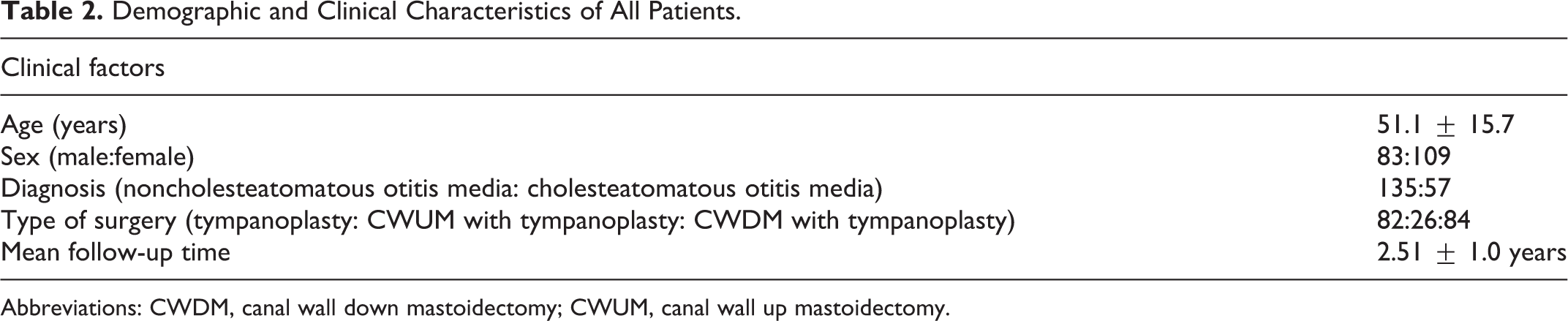
Abbreviations: CWDM, canal wall down mastoidectomy; CWUM, canal wall up mastoidectomy.
Changes in Mean Air and Bone Conduction Hearing Thresholds After Surgery for Chronic Otitis Media.a
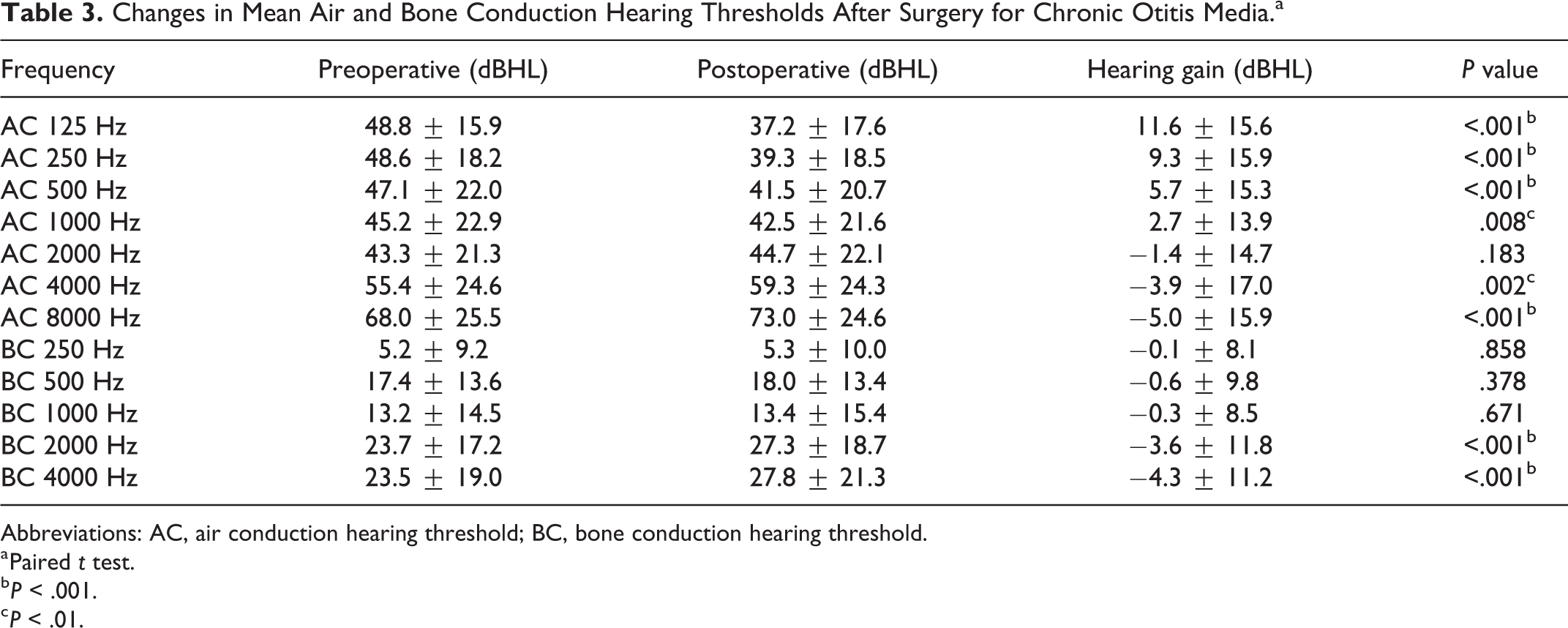
Abbreviations: AC, air conduction hearing threshold; BC, bone conduction hearing threshold.
a Paired t test.
b P < .001.
c P < .01.
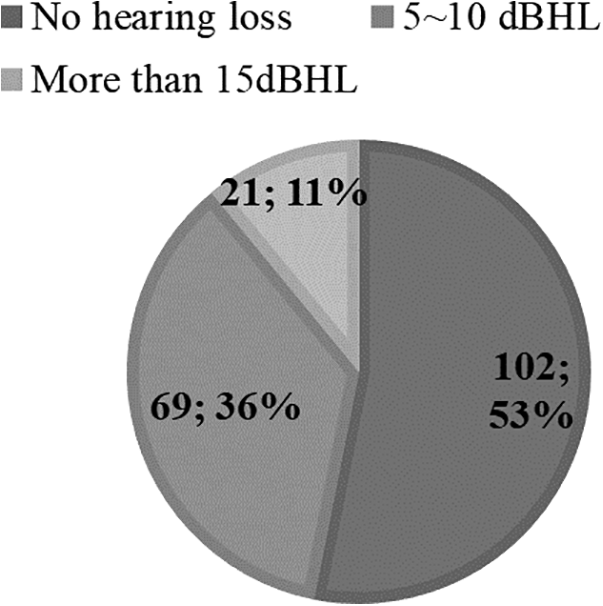
The numbers and proportions of patients with reduced bone conduction hearing at 4000 Hz.
We compared the clinical characteristics of the 21 patients with clinically meaningful hearing impairment (>10 dBHL at 4000 Hz) to those of the remaining 171 patients because there may be patient errors within 10 dBHL in repeated tests. 4 The former group was significantly younger and more likely to have ChOM (Table 4); this was also the case in multiple regression analysis (Table 5). We also compared the characteristics of the ChOM and NChOM patients (Table 6). Significantly, more ossiculoplasties and mastoidectomies were performed in the ChOM group, which also exhibited significantly longer operation times and more severe inflammation on CT than did NChOM patients.
Factors Associated With Preserved and Poorer Hearing.
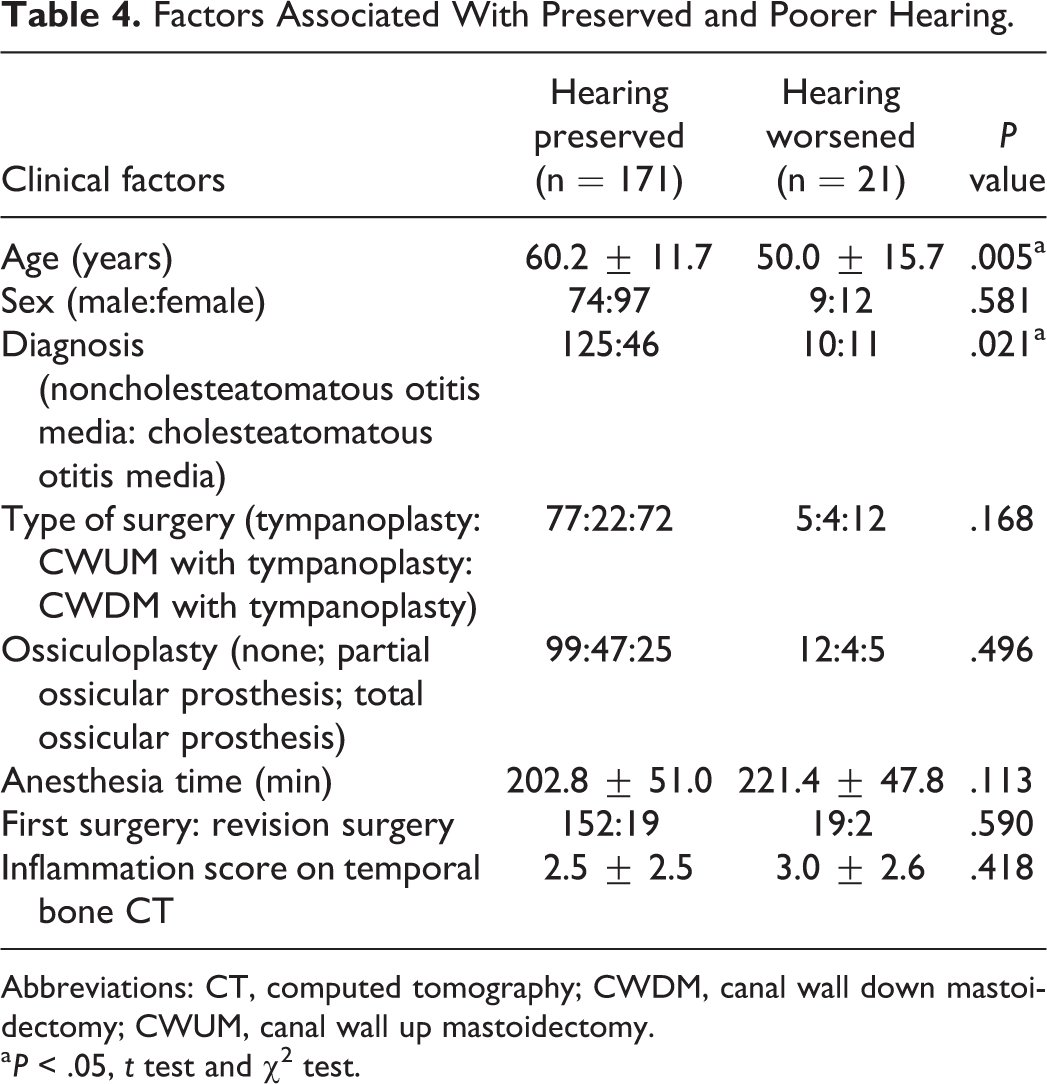
Abbreviations: CT, computed tomography; CWDM, canal wall down mastoidectomy; CWUM, canal wall up mastoidectomy.
a P < .05, t test and χ2 test.
Independent Risk Factors for SNHL at 4000 Hz After Surgery for Chronic Otitis Media.a
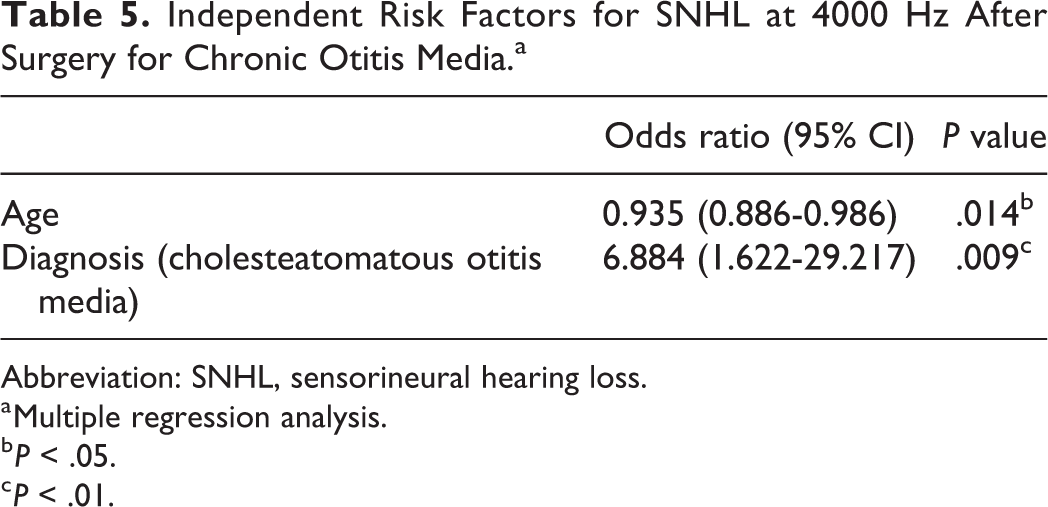
Abbreviation: SNHL, sensorineural hearing loss.
a Multiple regression analysis.
b P < .05.
c P < .01.
Comparison of Patients With Cholesteatomatous Otitis Media and Noncholesteatomatous Otitis Media.a
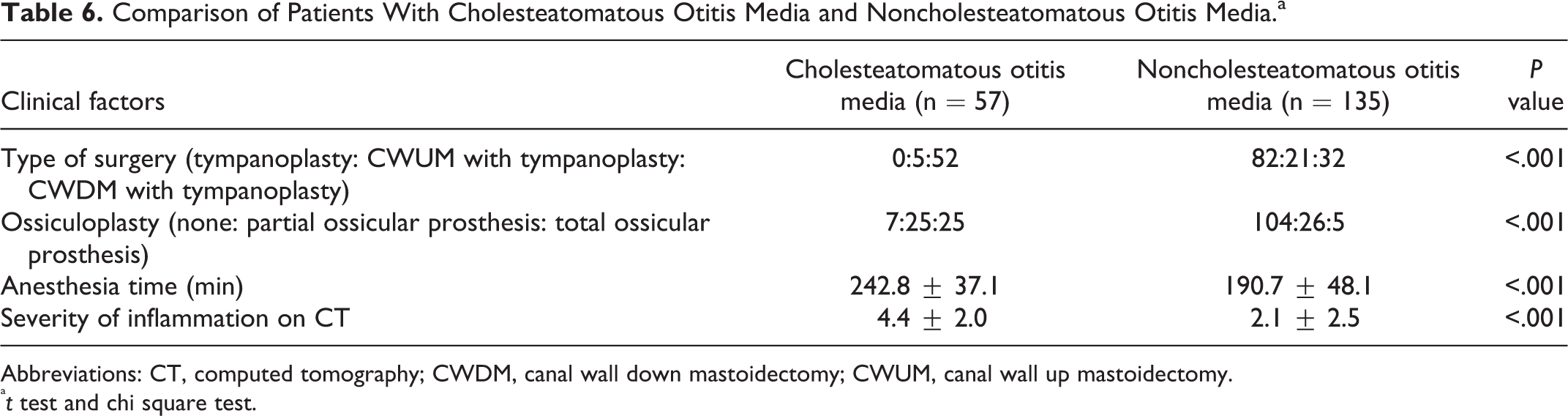
Abbreviations: CT, computed tomography; CWDM, canal wall down mastoidectomy; CWUM, canal wall up mastoidectomy.
at test and chi square test.
Discussion
In this study, SNHL after COM surgery occurred principally in the high-frequency range; the probability of a BC hearing threshold increase of more than 15 dBHL at 4000 Hz was 11%. Other studies also found that most SNHL after COM surgery occurred in the high-frequency region (>2 kHz). 5,6 However, the incidence of SNHL differs among reports according to the way in which hearing was evaluated. Two studies reported deterioration of the average BC hearing threshold of approximately 3% (by >10 dB) from 500 to 4000 Hz. 7,8 However, as in the present study, the incidence of SNHL was 4.5% to 8% when only high-frequency SNHL was evaluated. 3,5 The “dead ear” rate after surgery was about 1%. 1,9 We found that a diagnosis of ChOM and younger age were independent risk factors for BC hearing loss at 4000 Hz. In the ChOM group, significantly more ossiculoplasties and mastoidectomies were performed, and these patients also exhibited significantly longer operation times and more severe inflammation on CT than NChOM patients (Table 6). However, after COM surgery, patients with versus without poorer did not differ in terms of these factors (Table 4), perhaps because ChOM surgery differs somewhat from NChOM surgery. During the latter surgery, small amounts of granulation tissue around the facial nerve, oval window, or stapes are sometimes preserved to avoid complications. However, ChOM surgery requires meticulous removal of the cholesteatoma, because any residual cholesteatoma may regrow. Many manipulations are performed around the ossicle, so the risk of inner ear damage is higher. Also, as an acquired cholesteatoma is always located around the ossicle, the ossicle must be at least touched, and sometimes even removed. Other studies also found that the SNHL rate in patients undergoing ChOM surgery was higher than that in those undergoing NChOM surgery. 1,8
Reports on SNHL caused by mastoidectomy (drilling) have been conflicting. 2,3,10 -12 We found that mastoidectomy status (yes or no) did not correlate significantly with the incidence of SNHL at 4000 Hz. Also, ossiculoplasty status (yes or no) did not significantly affect the likelihood of SNHL development (Table 4). Given such contradictory results, it seems that not just the type of surgery performed, but also ossicle status, iatrogenic ossicle injury, footplate mobility, and the extent of manipulation around the ossicle may be relevant. Prospective observational studies evaluating these important variables could provide more meaningful results.
Our finding that younger patients are at higher risk of SNHL after COM surgery requires confirmation. It is possible that BC hearing is relatively good in young patients; the proportional extent of deterioration after surgery is thus large. Correlation analysis showed that BC hearing was better in younger patients, but we found no correlation between the preoperative BC hearing level and extent of SNHL loss after COM surgery (data not shown).
It is difficult to offer suggestions as to how the operator could reduce the incidence of SNHL. Prinsley 1 reported that half of the “dead ears” after surgery could have been avoided, being attributable to accidental injury to the ossicle or oval window. We consider that drilling (mastoidectomy) is essential; proceeding with great care around the ossicles may reduce SNHL.
Our study had some limitations. First, a single surgeon performed all of the procedures, where outcomes may vary according to the skill of the surgeon. Also, there may have been a selection bias, because patients whose preoperative hearing threshold was unmeasurable at any frequency were excluded. However, as our results are similar to those of previous studies, we suggest that surgeons should consider the possibility of high-frequency SNHL when operating on young patients with ChOM. In particular, the surgeon should emphasize the risk of SNHL when seeking preoperative consent, and all ossicle manipulations should be performed as safely as possible.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (grant no. NRF- 2020R1C1C1003869).