
Abstract
Metastasis to the clivus and sphenoid sinus from breast cancer is exceedingly rare, with few cases documented in the literature. This case report presents a 68-year-old female with a history of breast cancer who developed metastasis to the clivus extending into the sphenoid sinus. The clinical presentation, diagnostic challenges, and therapeutic interventions are discussed, with a review of similar cases in the literature to highlight the importance of early recognition and multidisciplinary management.
Introduction
Breast cancer is the most common malignancy affecting women worldwide, with an incidence of greater than 11% according to GLOBOCAN estimates in 2020. 1 It is the leading cause of cancer-associated mortality in women, with mortality rates ranging anywhere from 6% to 14%, causing approximately 685,000 deaths globally in 2020.1-3 Metastatic disease is responsible for the vast majority of cancer-related deaths, and it is estimated that 30% of patients diagnosed with early-stage disease will progress to develop metastases. 4
The most common sites of metastasis for breast cancer include the bones, lungs, liver, and brain. 5 However, metastasis to the clivus and paranasal sinuses, particularly the sphenoid sinus is exceedingly rare. Primary clivus and sphenoid masses are uncommon and can include a variety of neoplasms such as chordomas, chondrosarcomas, and meningiomas. 6 Metastatic lesions to the clivus are estimated to represent only 0.02% of all intracranial tumors. Of these, the most common primary sites of metastasis are prostate (23%), gastrointestinal (15%), lung (13%), and kidney (11%). 7 There have been minimal reports of breast cancer metastases to the clivus.
In this report, we present a case of breast cancer metastatic to the clivus and extending into the sphenoid sinus, with an extensive review of the literature. We discuss the clinical presentations, diagnostic challenges, and management strategies associated with this rare metastatic site. Data are synthesized from previously reported cases, identifying trends in patient symptom presentation and treatment responses.
Case Presentation
A 68-year-old female with a past medical history significant for homelessness, hypertension, hypercholesterolemia, chronic obstructive pulmonary disease, myocardial infarction, and left breast high-grade malignant sarcomatoid and epithelioid neoplasm presented to the emergency department with a headache after a ground level fall. The patient denied any loss of consciousness, nausea, vomiting, focal weakness, sensory deficits, vision changes, or hearing changes. Additionally, she reported chronic central chest pain, shortness of breath that worsens with exertion, and a dry cough. On physical examination, the patient had extraocular movements intact of right and left eye except for limited abduction of left eye with patient reporting diplopia with this eye movement.
The patient’s breast high-grade malignant sarcomatoid and epithelioid neoplasm was first diagnosed 3 months prior to the above-described presentation. She underwent a left mastectomy and left axillary sentinel node biopsy during the hospital admission of her initial breast cancer presentation. Final pathology demonstrated left breast high-grade malignant sarcomatoid and epithelioid neoplasm with negative margins with 3 left axillary sentinel lymph nodes negative for malignancy. The overall morphologic and immunophenotypic profile was not specific for any diagnostic entity. The differential diagnosis included a sarcoma; however, the possibility of a melanoma or carcinoma could not be entirely excluded. Outpatient chemotherapy and radiation was being coordinated by hospital case management; however, the patient never followed up with surgical oncology or oncology after discharge and never underwent adjuvant therapy.
A computed tomography (CT) scan of the patient’s head was performed that demonstrated a destructive soft tissue mass centered at the clivus measuring 3 × 2.5 by 3.5 cm with extension into the sphenoid sinus and some extension into the dural space anterior to the pons/medulla (Figure 1). A computed tomography angiogram (CTA) scan was performed of the patient’s chest that demonstrated a recurrent left chest wall mass just posterior to the posterior border of the left pectoralis major muscle measuring 2.9 cm × 3.6 cm compared to previous imaging prior to the patient’s left mastectomy.
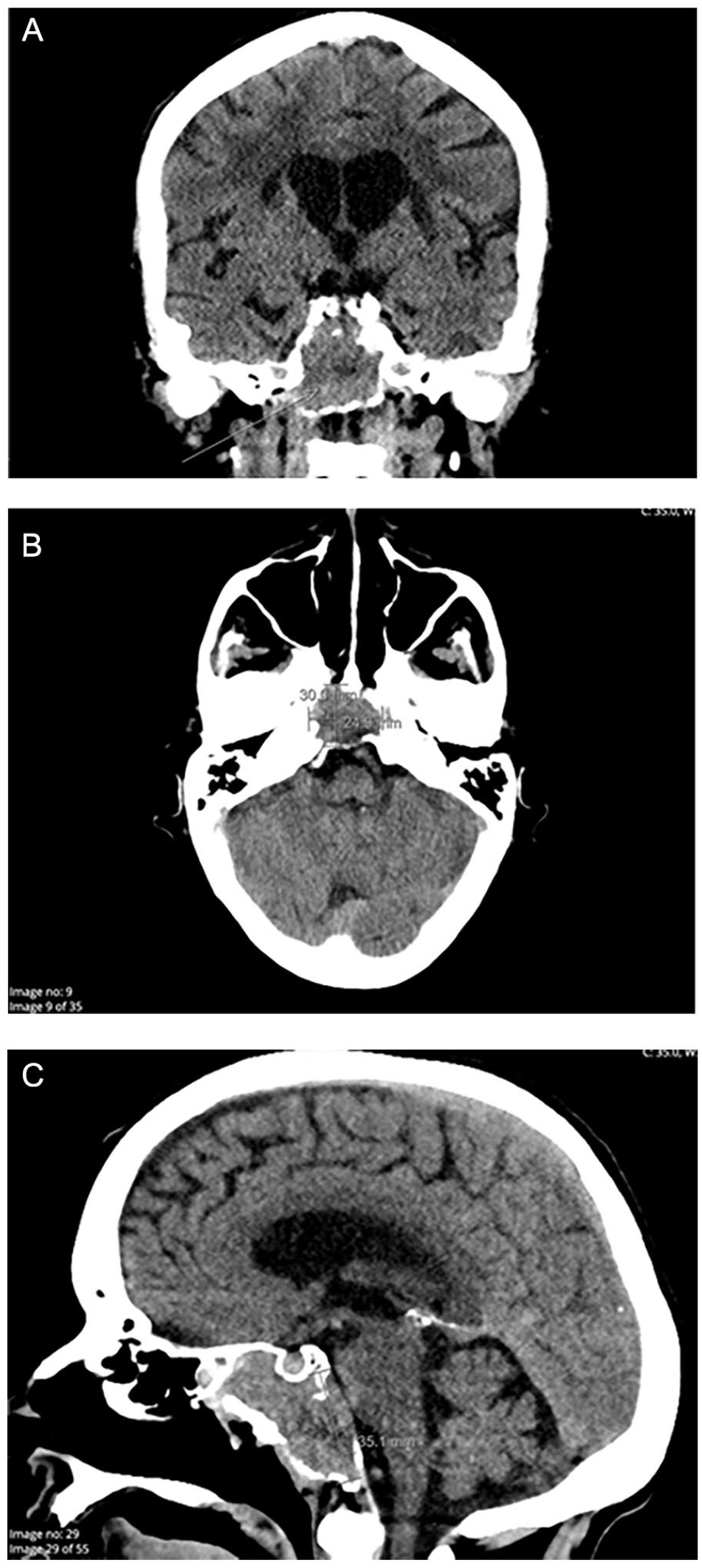
CT head demonstrating clivus mass. (A-C): CT head without contrast demonstrating a destructive soft tissue mass centered at the clivus measuring 3 × 2.5 by 3.5 cm with extension into the sphenoid sinus and some extension into the dural space anterior to the pons/medulla. Mass is delineated by an arrow or measurement. (A) Coronal view. (B) Axial view. (C) Sagittal view.
A subsequent magnetic resonance imaging (MRI) of the head with and without contrast revealed an enhancing solid mass involving the sphenoid sinus, clivus, extends into the posterior margin of the right ethmoid air cells and inferiorly into the right occipital condyle measuring about 2.6 × 4.0 cm axial by 4.2 cm in greatest craniocaudad length. Based off imaging, differential diagnosis included chordoma, metastatic focus, skull base chondrosarcoma, or plasmacytoma (Figure 2). A CT sinus with and without contrast was performed demonstrating a soft tissue mass involving the posterior right sphenoid sinus with erosion of the clivus, basiocciput on the right side and minimal extension into the retroclival region. There was also expansion into the bilateral parasellar regions with erosion of the right petrous apex with questionable involvement of the right pterygopalatine fossa (Figure 3).
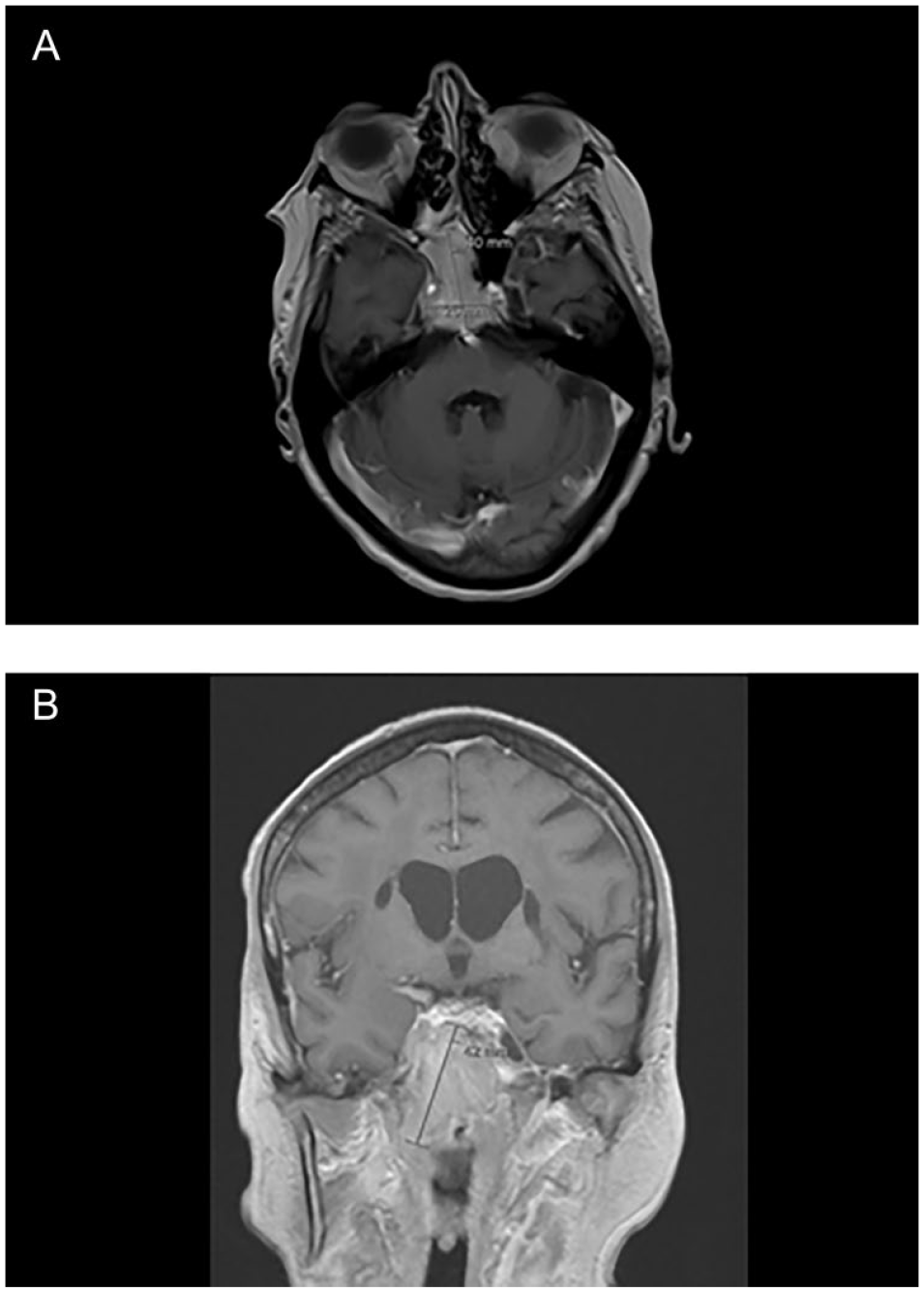
MRI brain demonstrating clival mass.
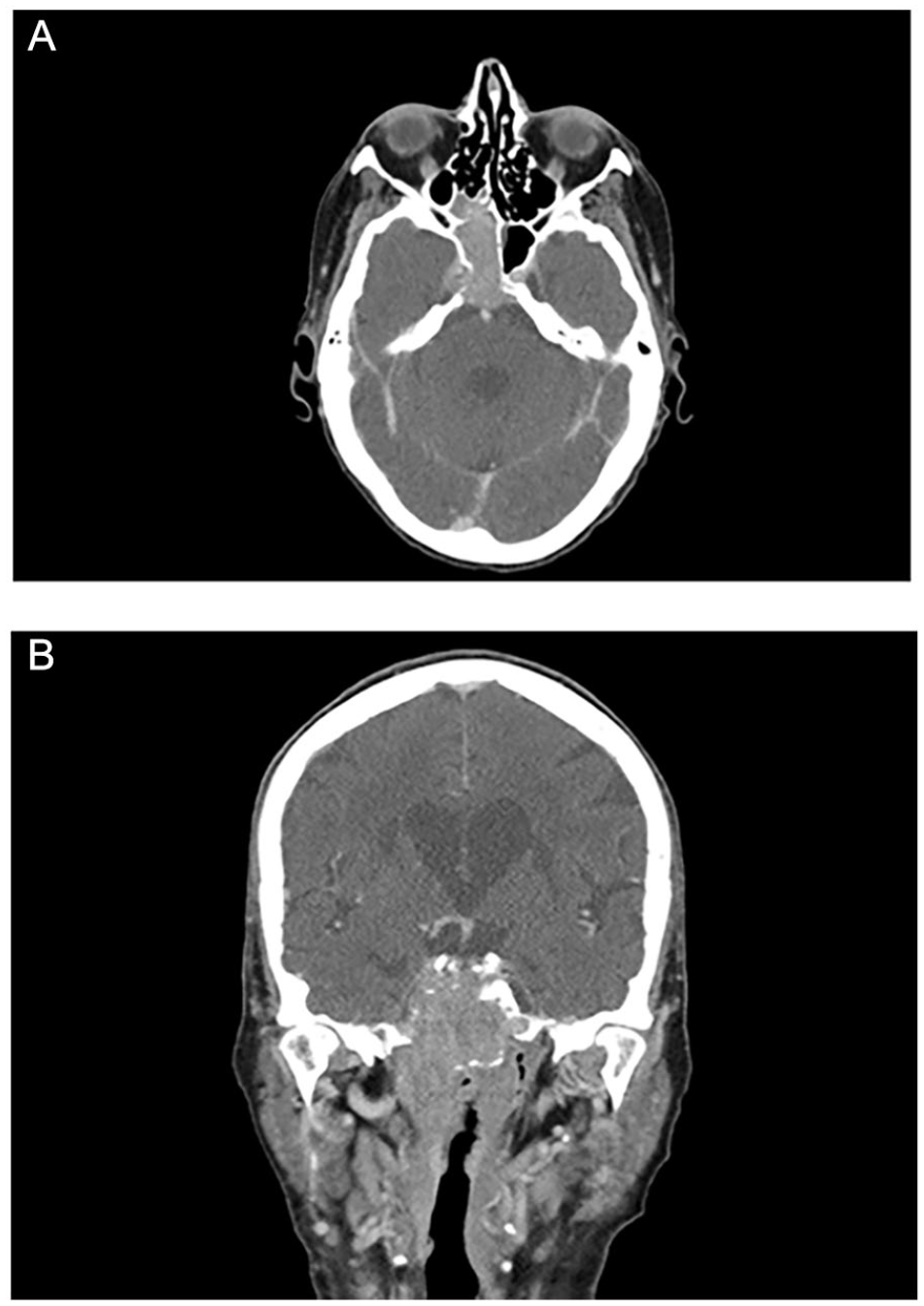
CT sinus demonstrating clival mass.
After thorough discussion with the patient of the risks, benefits, and alternatives to further diagnostic work up of this clival mass, it was decided to proceed with biopsy of the mass. Written consent was obtained, and the patient underwent nasal endoscopy with biopsy to determine if this mass was metastasis from the patient’s breast cancer or if it was a separate entity. Final pathology confirmed metastatic breast carcinoma, consistent with the patient’s known high-grade malignant sarcomatoid and epithelioid neoplasm of the breast (Figure 4).
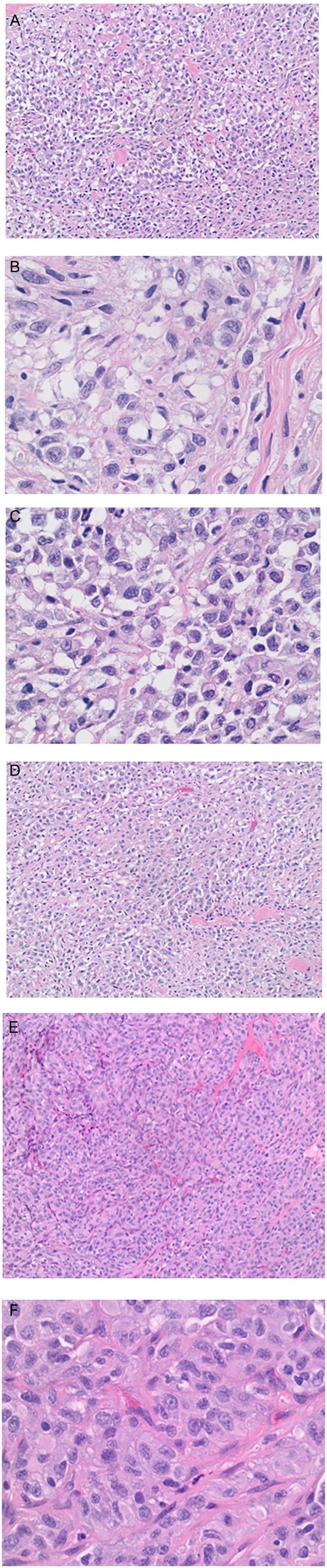
Key histology images.
Per surgical oncology, there was no plan for further palliative resection of the recurrent left chest wall mass as it was asymptomatic with no overlying wound or tenderness. Given the patient’s metastatic disease, there was determined to be no therapeutic goal in resecting the mass as well. The patient elected to be category II do not intubate and do not resuscitate. She progressively became more drowsy and altered during this hospital stay and she eventually expired about 1 month after pathology results finalized for the sphenoid biopsy.
Discussion
Metastasis to the clivus and sphenoid sinus from breast cancer is exceedingly rare, comprising only 0.02% of all intracranial tumors. 7 Metastasis of primary tumors to the paranasal sinuses is also an uncommon event, with only 8% originating from primary breast cancer. 8 Recent studies have elucidated the mechanism of breast cancer metastasis through induction of epithelial-mesenchymal transition (EMT) as well as cytokines secreted by the tumor microenvironment (TME) and epigenetic modifications. 9 Although rare, different sites of the head and neck may be involved including the temporal bone, parotid gland, nasopharynx, larynx, nose, and paranasal sinuses. 10
The clinical presentation of clival metastases often includes nonspecific symptoms such as headaches, cranial nerve deficits, and sinusitis-like symptoms, which complicate the diagnosis. 11 Literature review indicates that the most commonly affected cranial nerve is the abducens nerve, leading to symptoms such as diplopia and lateral rectus palsy.12,13 Additionally, visual disturbances are common due to the involvement of the cavernous sinus and sphenoid sinus, affecting cranial nerves III, IV, and VI.14,15 Diplopia, particularly due to sixth cranial nerve involvement, is a frequent presenting symptom in patients with clival metastasis. 16
Neck pain is another symptom that has been reported in patients with clival metastasis, often resulting from the mass effect of the tumor on surrounding structures and possible spinal involvement. Persistent neck pain was a significant symptom in our patient, highlighting the extent of metastatic involvement. 17 Headaches are also a common symptom of clival metastasis, often due to increased intracranial pressure or direct invasion of pain-sensitive structures. The severity and persistence of headaches in our patient, combined with other neurological deficits, were key indicators of the metastatic spread. 7
This case of a 68-year-old female with metastatic breast cancer underscores the importance of considering metastatic disease in patients with a history of breast cancer, even when lesions appear in atypical locations like the clivus and sphenoid sinus. The patient’s initial presentation with a fall, followed by persistent neck pain and headache and incidental finding of a clival mass in the setting of previous breast cancer highlights the diagnostic challenges associated with such rare occurrences.
Literature Review and Case Comparisons
A review of the literature demonstrates significant variability in the presentation and findings of breast cancer metastases to atypical sites such as the paranasal sinuses and clivus. Among the reports included, the most common presenting symptom appears to be diplopia due to cranial nerve VI involvement. The most commonly implicated of the paranasal sinuses is the sphenoid sinus, with 5 of the 8 reports documenting involvement. This is consistent with the tumor location in our patient.
Diagnostic Tools
Diagnosis of clival metastasis typically involves a combination of imaging and histopathological examination. MRI and CT are crucial for evaluating the extent of the lesion and its effects on surrounding structures. MRI is particularly valuable for its ability to differentiate between various tissue types and detect subtle changes in soft tissue. 7 For instance, chordomas typically appear as hyperintense on T2-weighted images, while metastases often exhibit more heterogeneous signal intensities due to their variable tissue composition. 22 CT scans can provide detailed images of bone structures and detect bone erosion and destruction, which is common in metastatic lesions.
Histopathological analysis is crucial in confirming the diagnosis, with immunohistochemical staining revealing markers consistent with primary breast carcinoma, including ER, PgR, and HER2. 12 In the case of our patient, histopathology was consistent with high-grade malignant sarcomatoid and epithelioid neoplasm.
Management Options
Surgical resection is typically considered in specific scenarios including solitary metastasis and reduction of tumor burden. For instance, a study by Karetta et al. details the role of surgery in both diagnosis and symptomatic relief, while balancing the risk-benefit ratio. 23 The same study reports that the majority, 79.5% of patients who underwent operation had some degree of cranial nerve palsy. 23 There is a possibility in these patients that debulking surgery may effectively decompress neural structures.
Chemotherapy or radiotherapy is often chosen when there is a necessity for systemic disease management, inoperable tumors, or palliation. For example, tumors involving critical structures that make surgical resection risky or unfeasible are often managed with radiotherapy. A majority of the literature review described in this case report concluded that radiotherapy and chemotherapy is most often employed in clinical practice, and have shown improvement in patient outcomes.12–15,18–21
In many cases documented in the literature, a combined approach of surgery followed by adjuvant therapies is adopted to maximize patient outcomes. The decision to pursue surgery versus nonsurgical options depends on various factors including the patient’s overall health, extent of disease, and symptoms. Review of the literature suggests that while surgery can be considered for symptom relief or decompression, palliative chemotherapy, and radiotherapy are often employed to control the disease.
Outcomes and Survival Rates
Outcomes and survival rates vary depending on the extent of metastasis and the patient’s overall condition. Early diagnosis and appropriate management can improve quality of life and potentially prolong survival.
Conclusion
Metastasis of breast cancer to the clivus and sphenoid sinus is a rare but important differential diagnosis for clival masses. This case report adds to the existing literature, highlighting the clinical presentations, diagnostic approaches, and management strategies. Recognizing this rare presentation can facilitate timely diagnosis and appropriate treatment, ultimately improving patient outcomes. Table 1 ellucidates different therapies used for previous cases of breast cancer metastasis to paranasal sinuses and clivus.
Case Reports of Breast Cancer Metastatic to Paranasal Sinuses and Clivus.
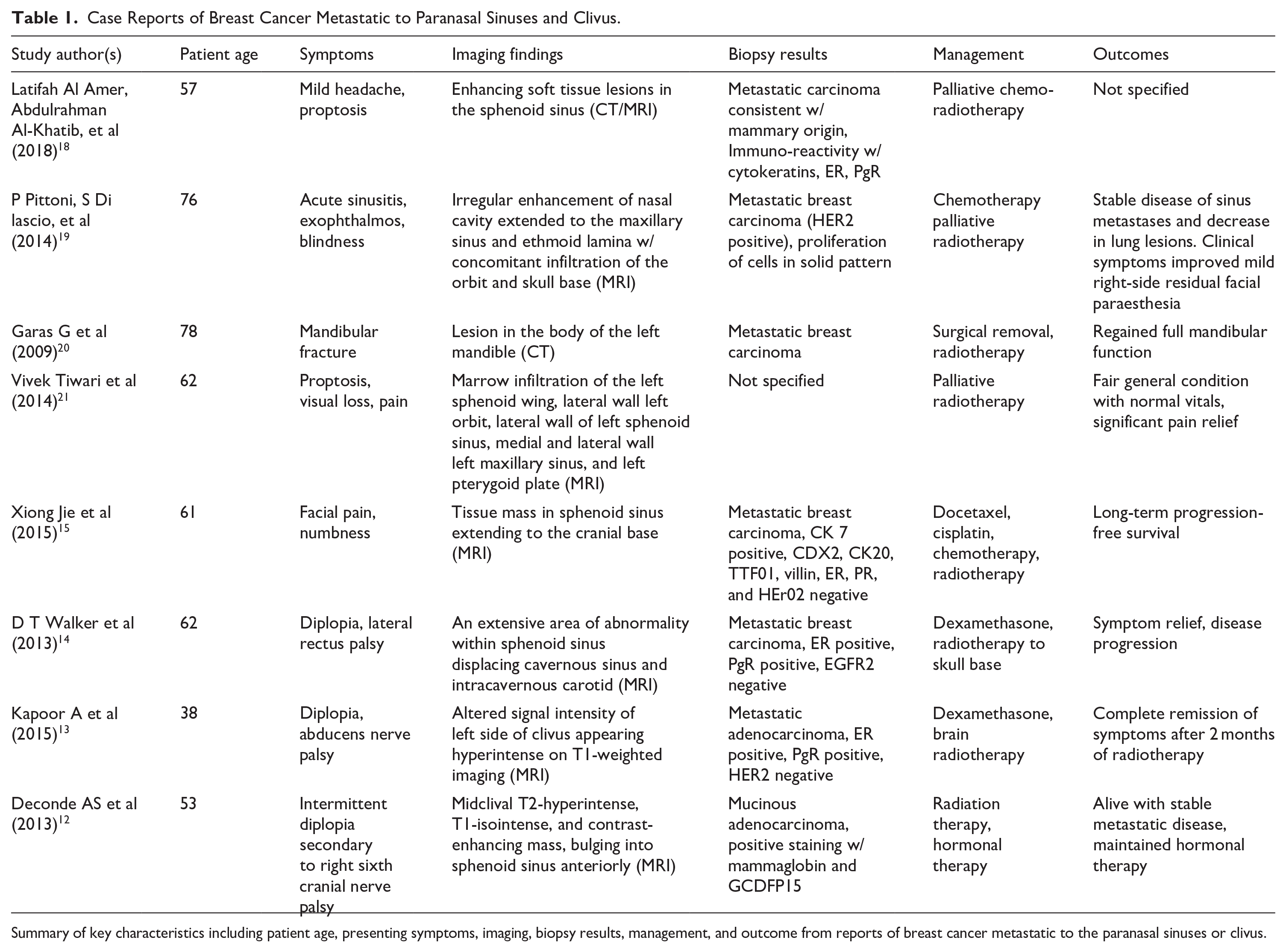
Summary of key characteristics including patient age, presenting symptoms, imaging, biopsy results, management, and outcome from reports of breast cancer metastatic to the paranasal sinuses or clivus.
Footnotes
Ethical Considerations
This case report was conducted in accordance with institutional ethical standards and the Declaration of Helsinki. Written informed consent was obtained from the patient for publication of this case report and any accompanying images. The authors affirm that this manuscript complies with all relevant ethical publication guidelines.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available within the article. No additional data are available.