
Abstract
Objective:
This study aimed to investigate whether the anatomical location of the globus sensation influences treatment outcome in patients with globus pharyngeus.
Methods:
A prospective cohort study was conducted between March 2023 and May 2024 with 55 patients who presented with globus sensation. The participants were categorized into the upper and lower globus groups based on the anatomical location of globus sensation relative to the upper esophageal sphincter. All patients received proton pump inhibitor (PPI) therapy for up to 12 weeks, and treatment response was assessed using the Reflux Symptom Index (RSI) and Reflux Finding Score (RFS). Log-rank tests and logistic regression analysis were performed to identify the factors associated with treatment response.
Results:
Patients with upper globus showed a significantly-higher rate of symptom improvement (78.6%) than those with lower globus (40.7%). Symptom severity (measured by the RSI) was higher in the lower globus group, while posterior commissure hypertrophy (measured by the RFS) was more prevalent in the upper globus group. Factors positively associated with symptom improvement included the location of the upper globus and coffee cessation. The lower globus group showed resistance to PPI therapy.
Conclusion:
Patients with upper globus respond better to PPI therapy, whereas those with lower globus do not. The anatomical location of the globus sensation may affect treatment outcomes.
Introduction
Globus pharyngeus (GP) is defined as a sensation of a lump or foreign body in the throat. GP is a common condition, affecting up to 45.6% of healthy adults in community-based studies and accounting for ~4% of all consultations in otorhinolaryngology departments. 1 Despite its common occurrence, the etiology of GP remains unclear and multifactorial, including reflux diseases, psychological factors, and local structural abnormalities. 2
Emerging evidence suggests a significant role of reflux in the pathogenesis of GP. 3 However, the response to reflux suppression therapy varies widely; therefore, identifying factors predictive of treatment success is essential for optimizing patient care.
The location of globus sensation is most often in the midline and primarily in the lower neck below the hyoid bone.4,5 However, this region contains various anatomical structures. Notably, the hypopharynx and cervical esophagus are the primary structures in this area. Therefore, it raises the question of whether all patients with GP share a single pathophysiology. For instance, there has been a report of globus sensation occurring due to high pressure in the upper esophageal sphincter (UES), even in the absence of evidence of reflux. 6
The pathophysiology of globus sensation may differ depending on its location, potentially leading to variations in treatment response. In particular, the UES serves as a key anatomical landmark that separates the esophagus from the hypopharynx, making it a relevant boundary for understanding symptom distribution. Therefore, this study aimed to compare treatment responses between patients with globus sensation localized above versus below the UES, providing insights into potential pathophysiological differences and refining therapeutic strategies.
Materials And Methods
The authors obtained approval from the Institutional Review Board of Hallym University Sacred Heart Hospital.
Study Design and Population
This prospective cohort study was conducted at an otolaryngology outpatient clinic of a tertiary hospital between March 2023 and May 2024. The study enrolled patients aged 18-80 years who presented with the primary complaint of a persistent or intermittent, nonpainful sensation of a lump or foreign body in the throat. 5 To be eligible, patients were required to have experienced symptom onset at least 6 months prior and to have reported symptoms occurring at least once per week over the past 3 months. 5 Patients were excluded if they had definitive structural lesions identified on physical examination, laryngoscopy, ultrasonography, or neck imaging studies. All patients underwent flexible fiberoptic laryngoscopy, which was performed and interpreted by a single board-certified otolaryngologist, and the Reflux Finding Score (RFS) was recorded accordingly. 7 Patients with objective dysphagia, odynophagia, or a gastric inlet patch in the proximal esophagus were excluded. Additionally, patients with a documented psychiatric history, including a prior diagnosis of anxiety, depression, or somatization disorder, or those receiving psychiatric or neurological medications at the time of enrollment, were excluded. Furthermore, patients with a history of upper aerodigestive tract surgery or radiation therapy were not included in the study. All patients received empirical double-dose proton pump inhibitors (PPI) treatment with esomeprazole 20 mg twice daily for 4-12 weeks, with an extended treatment duration based on symptom persistence.5,8 Lifestyle modification was emphasized as part of the treatment protocol. Cessation of coffee, alcohol, and smoking was recommended.
Patient Selection
The patient selection process is illustrated in Figure 1. Of the 195 patients initially screened for globus symptoms, 35 were excluded owing to symptoms located off the midline or above the hyoid bone, regions sometimes associated with non-reflux conditions such as tonsillitis or hyoid bone syndrome. Additionally, 49 patients with the Reflux Symptom Index (RSI) score <13 were excluded, resulting in 111 patients with an RSI score of ≥13. Patients were categorized based on the anatomical location of the globus sensation relative to UES level, using the cricoid cartilage as a landmark: 53 patients were classified as having a lower globus below the cricoid and 58 patients as having an upper globus between the hyoid bone and cricoid (Figure 2). Following a 3 month follow-up, 26 patients with lower globus and 30 patients with upper globus were lost to follow-up, resulting in a final cohort of 27 patients with lower globus and 28 patients with upper globus. Follow-up loss was defined as cases in which symptom improvement was not confirmed within 3 months, but the patients discontinued outpatient visits on their own.
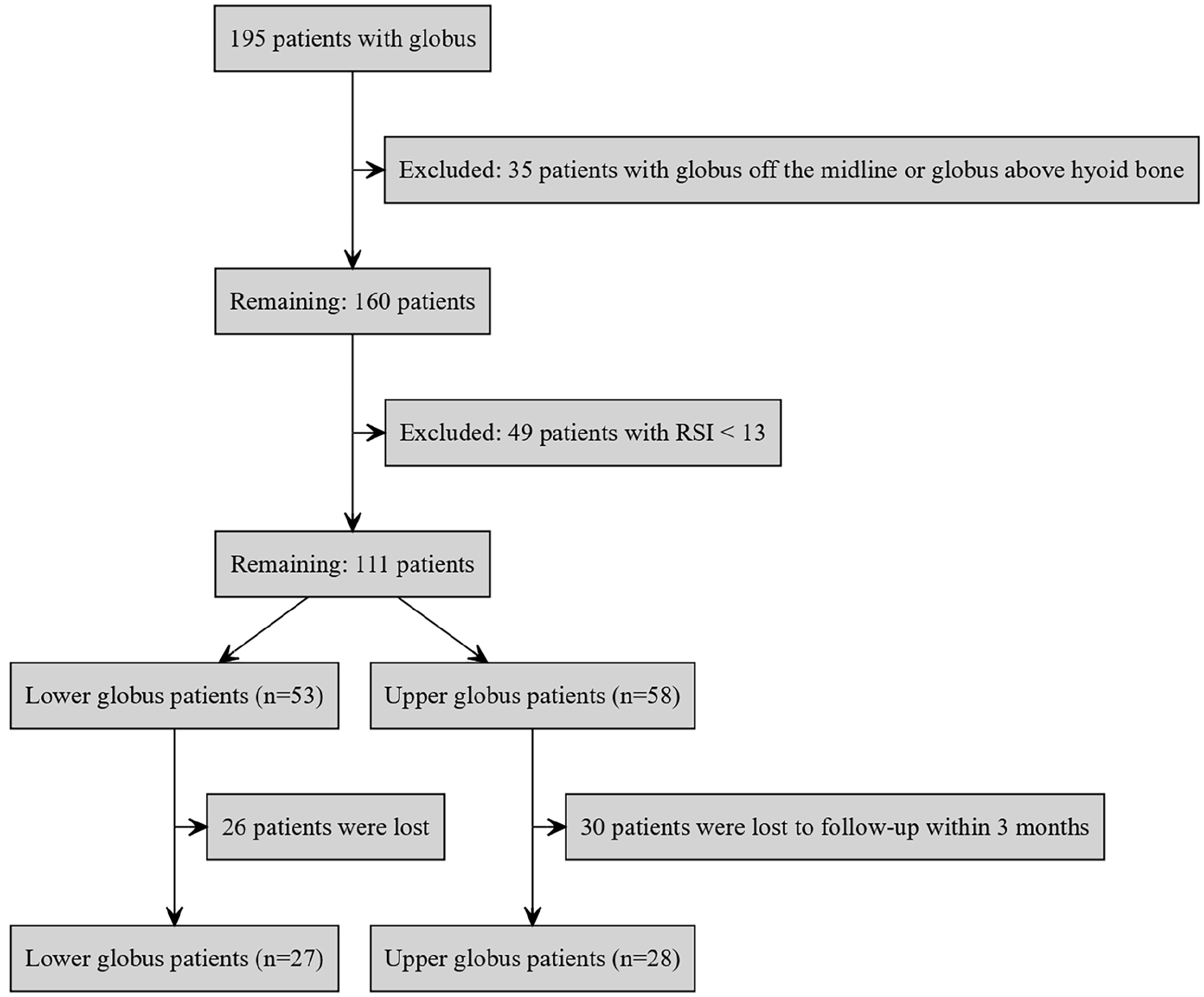
Patient selection flowchart.
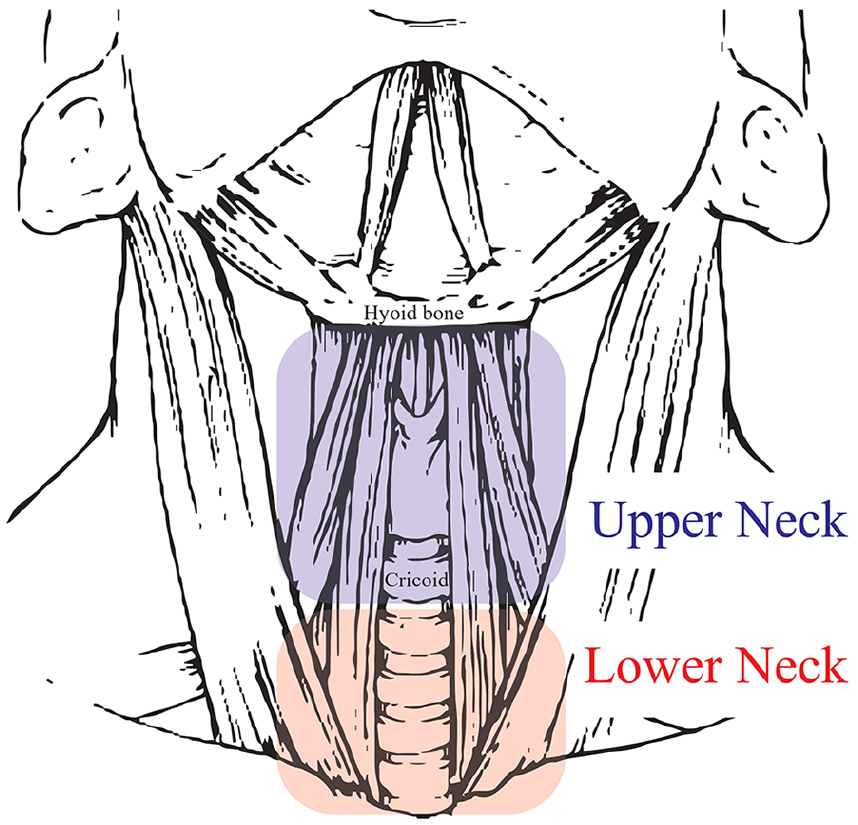
Anatomical division of globus symptom.
Covariates
Data were collected on demographic and lifestyle characteristics (Table 1), including age, sex, presence of hypertension and diabetes mellitus, alcohol and coffee consumption, and smoking status. The severity of globus symptoms was assessed using the RSI, as described by Belafsky et al, which consists of 9 items rated on a scale of 0 to 5, with a total score range of 0 to 45. 9 A score of 13 or higher was considered indicative of laryngopharyngeal reflux (LPR). Additionally, the RFS was used to evaluate laryngeal findings associated with reflux. The RFS is an 8-item scale with a total score ranging from 0 to 26, based on endoscopic findings. 7 A higher RFS score suggests greater laryngeal irritation due to reflux, with a score of 7 or higher commonly used as an indicator of LPR.
Demographic and Lifestyle Characteristics.
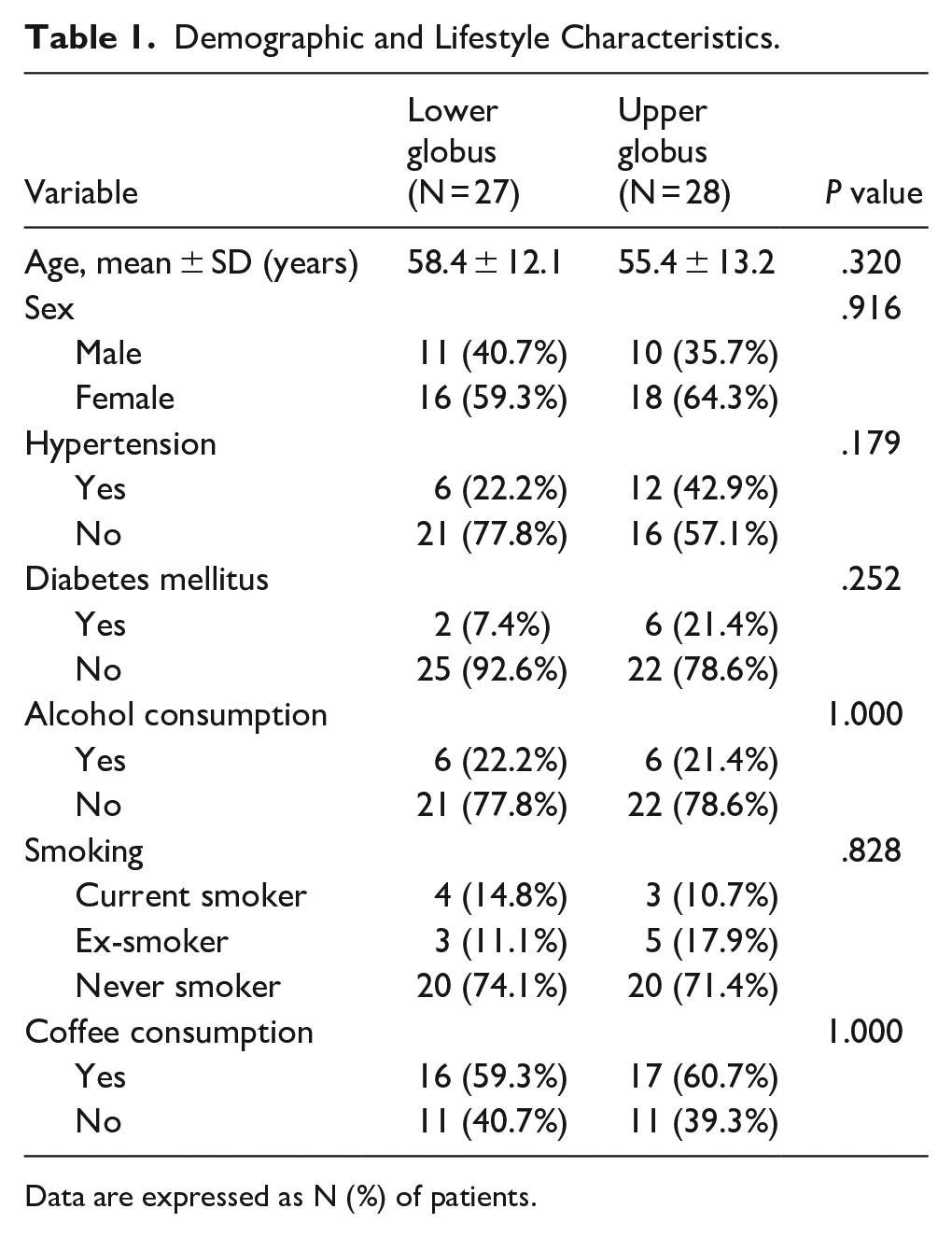
Data are expressed as N (%) of patients.
Definition of Symptom Improvement
In this study, symptom improvement was primarily evaluated based on the RSI score. Symptom improvement or treatment response was defined as a decrease in the RSI score to <13 points within 3 months of treatment. 9 The RFS was used as a secondary measure to evaluate objective changes in the throat after treatment.
Statistical Analysis
All statistical analyses were performed using the R statistical software (R Foundation for Statistical Computing, Vienna, Austria). Statistical analysis was performed to compare baseline and posttreatment RSI and RFS scores between the upper and lower globus groups. Continuous variables were analyzed using t-tests or Mann-Whitney U tests, depending on the normality of the data distribution. Categorical variables were analyzed using chi-squared tests or Fisher’s exact tests, where appropriate. A significance level was set at P < .05. Kaplan-Meier plots were used to analyze symptom persistence over time between the 2 groups, and the log-rank test was employed to compare survival curves. Logistic regression analysis was conducted to identify factors associated with symptom improvement, with odds ratios (OR) and 95% confidence intervals (CI) reported.
Results
The demographic and lifestyle characteristics of the study population are presented in Table 1. No significant differences were observed between the lower and upper globus groups in terms of age, sex, hypertension, diabetes mellitus, alcohol consumption, smoking status, or coffee consumption. Specifically, the proportion of female patients was slightly higher in both groups, and the average age was similar (58.4 ± 12.1 years for lower globus vs 55.4 ± 13.2 years for upper globus, P = .320). The incidence of hypertension and diabetes mellitus showed no significant difference between the groups (P = .179 and P = .252, respectively). Other lifestyle factors, such as alcohol consumption, smoking status, and coffee consumption, did not differ significantly between the 2 groups (P > .8).
The baseline and final RSI and RFS values for the lower and upper globus groups are summarized in Tables 2 and 3. Table 2 shows a detailed comparison of the RSI and RFS scores between the lower and upper globus groups at baseline. Although the overall RSI scores were slightly higher in the lower globus group (22.5 ± 6.4) than in the upper globus group (20.4 ± 5.4), this difference was not statistically significant (P = .255). Further, the globus sensation was significantly more severe in the lower globus group (4.4 ± 0.7) than in the upper globus group (3.7 ± 1.2), with a P value of .014. In contrast, the RFS component of posterior commissure hypertrophy was significantly more severe in the upper globus group (P = .030).
Comparison between Baseline RSI and RFS.
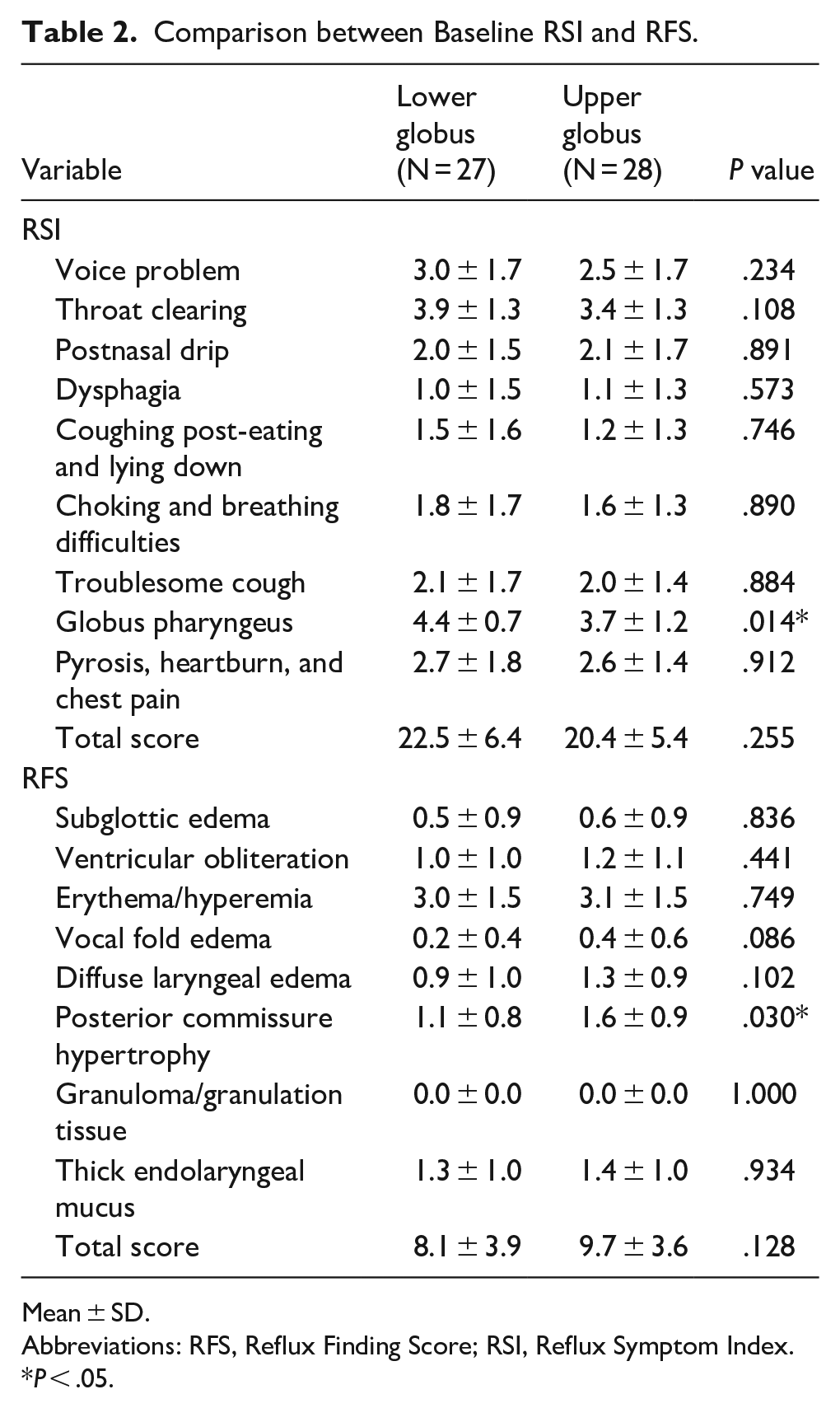
Mean ± SD.
Abbreviations: RFS, Reflux Finding Score; RSI, Reflux Symptom Index.
P < .05.
Comparison between Pretreatment and Posttreatment Reflux-Related Characteristics.
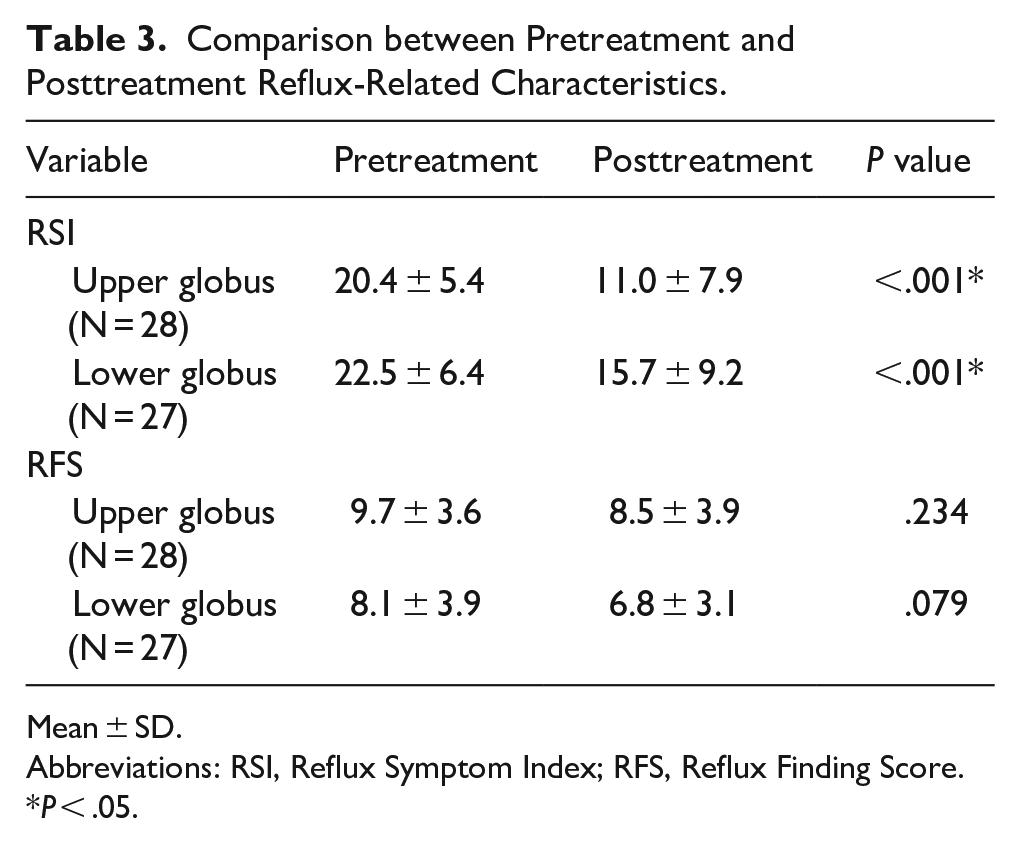
Mean ± SD.
Abbreviations: RSI, Reflux Symptom Index; RFS, Reflux Finding Score.
P < .05.
Patients in both the groups showed a significant reduction in the RSI scores after PPI treatment (P < .001 for both groups), indicating symptom improvement (Table 3). However, no significant differences were found in RFS scores before and after treatment (Table 3).
Table 4 and Figure 3 present a comparison of symptom improvement and persistence rates between the lower and upper globus groups. A significant difference in symptom improvement was observed, with a higher proportion of patients in the upper globus group showing improvement (78.6% vs 40.7%, P = .010). The probability of symptom persistence was significantly higher in the lower globus group than that in the upper globus group (Figure 3A and B). Figure 3A shows the results for patients who were not lost to follow-up within 3 months, as described in Figure 1, whereas Figure 3B shows the results for all patients, including those that were lost to follow-up.
Comparison of Symptom Improvement Ratio between the Lower and Upper Globus Groups.
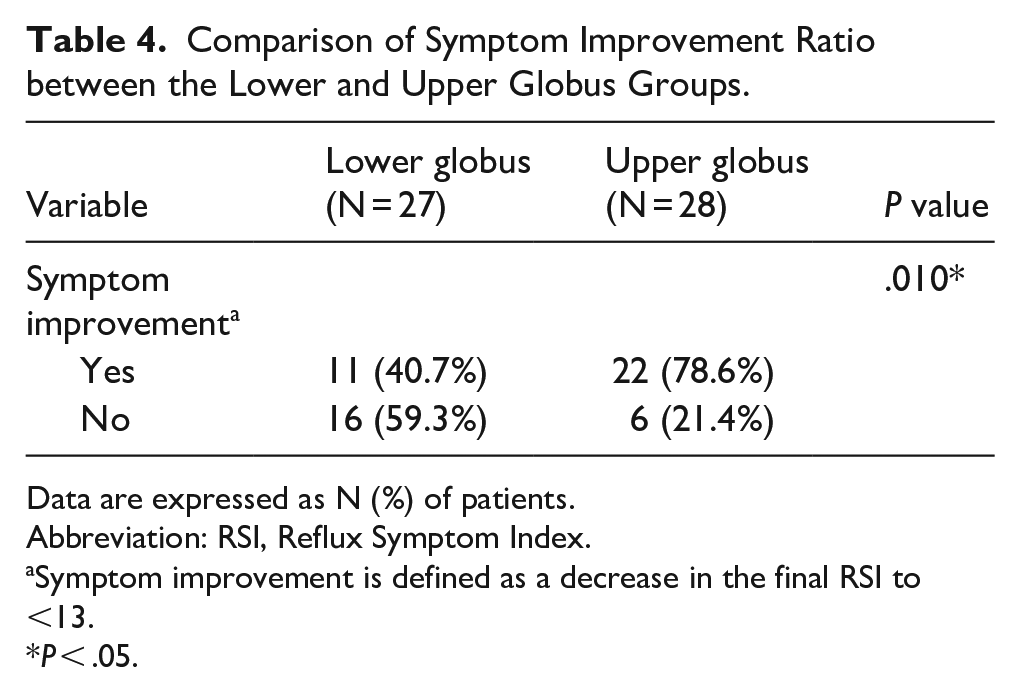
Data are expressed as N (%) of patients.
Abbreviation: RSI, Reflux Symptom Index.
Symptom improvement is defined as a decrease in the final RSI to <13.
P < .05.
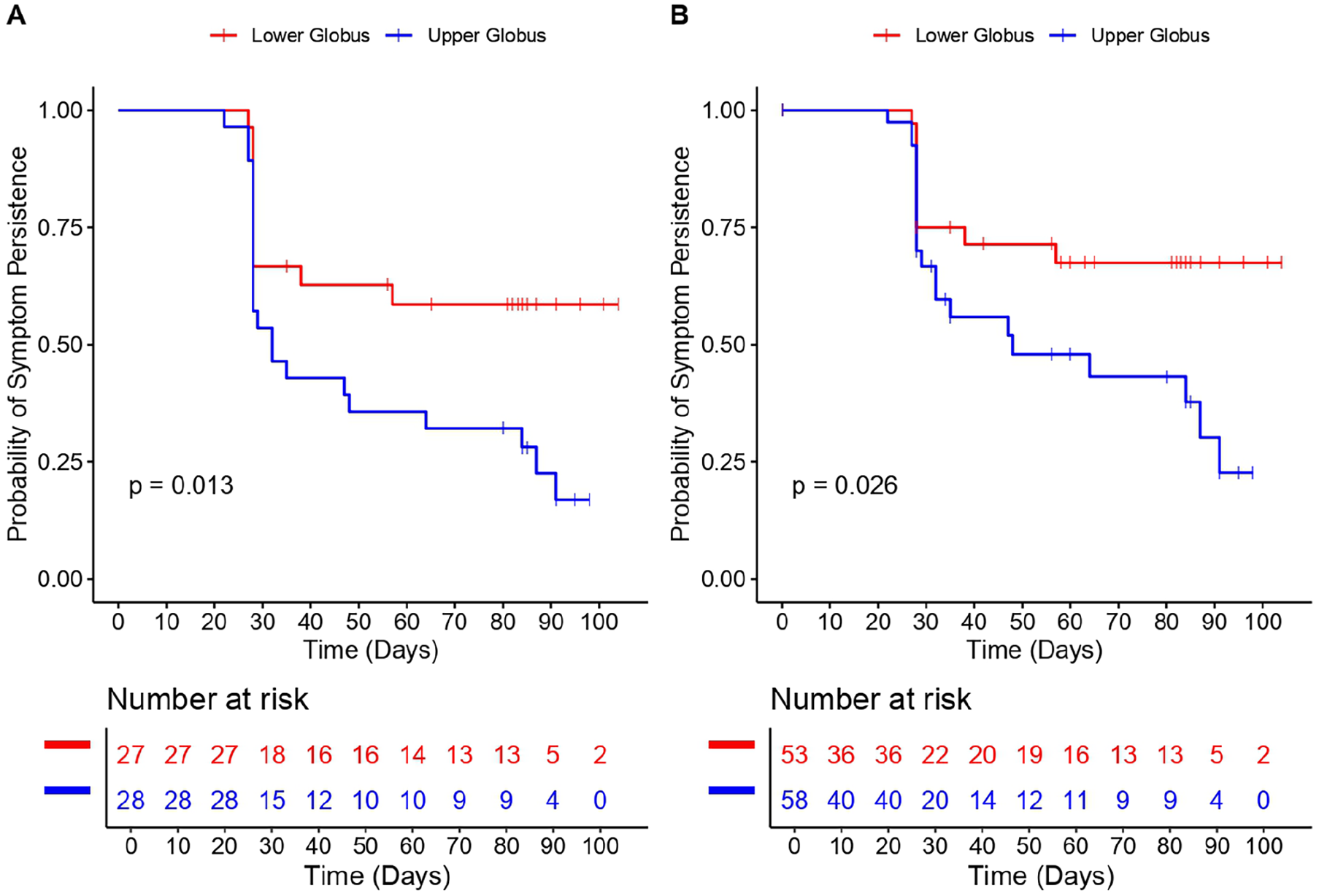
Symptom persistence rates. (A) Symptom persistence rates among 55 patients after excluding patients lost to follow-up. (B) Symptom persistence rates among 111 patients including patients lost to follow-up.
The forest plot in Figure 4 highlights the factors associated with symptom improvement. Patients with upper globus were significantly more likely to respond to PPI treatment (OR: 13.69, 95% CI: 2.11-88.74, P < .01). Other factors positively associated with symptom improvement included coffee consumption (OR: 10.13, 95% CI: 1.36-75.33, P < .05) and older age (OR: 1.1, 95% CI: 1.02-1.19, P < .05). High baseline RSI was negatively associated with symptom improvement (OR: 0.75, 95% CI: 0.62-0.91, P < .01), while sex (male) was not significantly associated with symptom improvement.
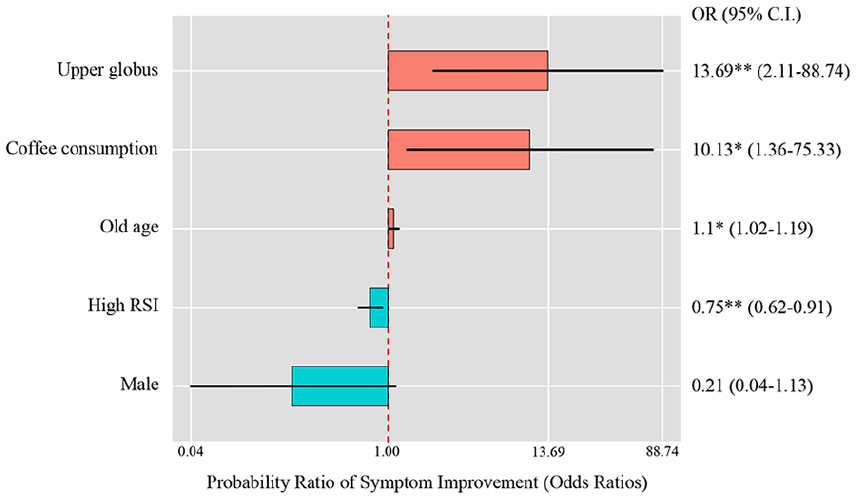
Forest plot showing the probability ratio of treatment success for various factors associated with symptom improvement in patients with globus. OR, odds ratio; 95% CI, 95% confidence intervals.
Discussion
In this study, we aimed to investigate the effect of anatomical location of the globus sensation on symptom severity and treatment efficacy. The present study revealed differences in symptom improvement and persistence between patients with upper and lower globus sensation. Specifically, the upper globus group exhibited a significantly-higher rate of symptom improvement, with 78.6% of patients showing improvement compared with 40.7% in the lower globus group (Table 4). The probability of symptom persistence after PPI treatment was significantly higher in the lower globus group than that in the higher globus group (Figure 3). Additionally, the baseline severity of symptoms was more pronounced in the lower globus group (RSI: 22.5 ± 6.4) than in the upper globus group (RSI: 20.4 ± 5.4), whereas posterior commissure hypertrophy was significantly-more prevalent in the upper globus group (Table 3).
Globus sensation is characterized by a persistent or intermittent feeling of a lump or foreign body in the throat. 8 Globus sensation is commonly located between the sternal notch and thyroid cartilage. 5 Globus sensation is often associated with reflux-related diseases. Non-reflux causes may include high UES pressure and psychogenic factors such as depression or anxiety disorders.6,10,11 To minimize the influence of psychogenic factors, we excluded patients with a psychogenic history from our study. The UES is mainly composed of the cricopharyngeus muscle, which extends from the caudal border of the cricoid cartilage to the first tracheal ring. 12 High UES pressure in this region may result in persistent or intermittent sensations of obstruction or a lump in the lower throat. If patients with high UES pressure were included in the lower globus group, they would have shown resistance to PPI treatment. In contrast, the better response to PPI treatment observed in the upper globus group suggests that this group may have included a relatively-higher proportion of patients whose globus symptoms were reflux-induced (Table 4).
The RSI and RFS are tools used to assess subjective symptoms and objective findings related to reflux. Belafsky et al observed that treatment responses are typically faster as evaluated by the RSI, whereas improvements evaluated by the RFS may take longer. 13 Our study found no significant improvement in RFS within 3 months, which is consistent with Belafsky’s observations (Table 3). While some studies have found a correlation between the RSI and RFS, most have not.14,15 In our study, the RSI was slightly higher in the lower globus group, whereas the RFS was slightly elevated in the upper globus group. The upper globus group exhibited a generally-higher RFS with significantly-higher posterior commissure hypertrophy (Table 2). Since the RFS does not assess structures below the cricoid level, it is reasonable that the upper globus group showed relatively-higher RFS scores. Among the RFS components, posterior commissure hypertrophy demonstrated a statistically-significant difference between the groups. The treatment success rate in the upper globus group (78.6%) was similar to that reported in previous studies on LPR (76.6%). 16 Conversely, the lower globus group showed a relatively-lower improvement rate of 40.7%.
This study revealed that coffee consumption positively correlated with symptom improvement in patients with GP. The effect of coffee consumption on acid reflux disease and its related symptoms varies across studies. Older studies conducted in 1997 reported that caffeinated coffee significantly promoted reflux-related symptoms, whereas decaffeinated coffee did not promote these symptoms. 17 Similarly, a 1978 study noted that coffee is generally considered a potent stimulus for gastric acid secretion and is thus associated with heartburn. 18 Conversely, more recent research found no significant relationship between coffee consumption and reflux diseases. A large-scale cross-sectional study conducted in 2013 found no significant association between coffee consumption and the incidence of gastric ulcers, duodenal ulcers, reflux esophagitis, or nonerosive reflux disease in 8013 healthy Japanese adults. 19 However, in the present study, all patients who consumed coffee were advised to stop coffee consumption. Therefore, the positive treatment outcomes observed in coffee-consuming patients may be attributed to the cessation of coffee intake rather than coffee consumption itself.
In our results, smoking and alcohol consumption did not significantly affect the GP treatment outcomes. However, existing research indicates that these factors may increase the risk of developing GP. For instance, Chen et al identified smoking and drinking histories as risk factors for acid reflux disease. 20 Similarly, stress, smoking, and alcohol consumption are significant risk factors for GP without LPR, potentially due to increased UES pressure. 6 Although our patients were advised to stop smoking and drinking early in the treatment, compliance may have been lower than adherence to coffee cessation.
This study had several limitations. First, because this was a single-center study, the generalizability of our findings may be limited. Second, the relatively-small sample size may have limited the statistical power of the study. Third, the follow-up duration was relatively short, which may not have been sufficient to assess the long-term effects of PPI therapy. Fourth, given that GP is a multifactorial symptom, the exclusive use of PPI therapy may have introduced a bias in treatment success rates by not accounting for other potential contributing factors. However, we attempted to minimize this limitation by systematically excluding patients with identifiable structural abnormalities, psychogenic histories, or neurological conditions. Nonetheless, the diagnosis of psychological factors can be complex, and undiagnosed or subclinical psychogenic components may have influenced treatment outcomes. Finally, the study did not include a comprehensive assessment of adherence to lifestyle modifications, such as cessation of coffee intake, smoking, and alcohol consumption, during the follow-up period, which may have influenced the outcomes. Future studies should aim to control for these variables more rigorously.
Conclusion
This study compared the efficacy of PPI therapy in patients with upper and lower globus sensation. The results indicated that patients with lower globus had a significantly-higher rate of symptom persistence than those with upper globus. This suggests that treatment outcomes of GP may vary depending on the anatomical location of the globus sensation. In clinical practice, the anatomical location of globus sensation could serve as a supplementary indicator for predicting treatment response when considering empirical therapy for GP.
Footnotes
Ethical Considerations
The study has received ethics approval from the Institutional Review Board of Hallym University Sacred Heart Hospital.
Author Contributions
Conceptualization: J.W.K. Data curation: S.-H.L. Formal analysis: S.-H.L. Methodology: J.W.K.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.