
Abstract
Objectives
To evaluate the different characteristics of oropharyngeal pH changes in patients with different laryngeal diseases.
Methods
A retrospective analysis was performed. The clinical data of 262 patients were summarized. The patients were divided into 4 groups. Group 1 included 123 patients with suspected laryngopharyngeal reflux disease (LPRD). Group 2 included 45 patients with vocal cord polyps. Group 3 included 40 patients with vocal cord leukoplakia. Group 4 included 54 patients with laryngeal carcinoma. Their reflux symptom indexes (RSIs), reflux finding scores (RFSs), and Dx-pH monitoring results were compared.
Results
In total, 235 patients had abnormal RSI/RFS, 90 patients had abnormal Ryan scores. The rate of abnormal RSI/RFS of Group 1 was significantly higher than that of Group 4 (P = .001). Significant differences of the rates of abnormal Ryan scores existed between Groups 2 and 4 (P = .021) and Groups 3 and 4 (P = .027). There were obvious differences in upright Ryan scores between Groups 1 and 2 (P = .013), Groups 1 and 3 (P = .002), Groups 2 and 4 (P = .046), and Groups 3 and 4 (P = .009). There were significant differences in time percentage of oropharyngeal pH of upright 5.5∼6.5 and supine 5.0∼6.5 between Groups 1 and 3 as well as Groups 1 and 4 (upright: Groups 1 and 3: P = .017; Groups 1 and 4: P = .019. Supine: Groups 1 and 3: P = .018; Groups 1 and 4: P = .023).
Conclusions
There were different oropharyngeal pH characteristics in patients with different laryngeal diseases, which indicated laryngopharyngeal reflux may play different roles in different diseases through various patterns. Patients with vocal cord polyps, vocal cord leukoplakia, and laryngeal carcinoma had more and different patterns of oropharyngeal pH change than patients with LPRD. Patients with vocal cord polyps and vocal cord leukoplakia had more severe acid oropharyngeal pH change episodes than patients with laryngeal carcinoma.
Introduction
Laryngopharyngeal reflux disease (LPRD) has recently become a research focus because it is common and harmful. LPRD consists of a series of signs and symptoms caused by laryngopharyngeal reflux (LPR), in which gastric contents flow backward beyond the upper esophageal sphincters. Symptoms of LPRD include pharyngalgia, globus pharyngeus, hoarseness, cough, dyspnea, and so on. 1 It was reported that LPRD occurred in 50% of patients with voice problems and in 10% of patients treated in otolaryngology outpatient departments. 2 Additionally, LPR may be a pathogenic factor of benign and malignant vocal cord lesions.3,4 However, the detailed relationship between LPR and different laryngeal diseases remains unclear. Our previous study found that the rates of LPR in patients with vocal cord polyps, leukoplakia, and carcinoma were different, indicating that the features and roles of LPR in patients with different hypertrophic laryngeal diseases should be different. 5 However, details of the differences are unknown.
In this article, we further summarized and compared the characteristics of oropharyngeal pH of patients with different laryngeal diseases to explore the possible disparities in more detail.
Patients and Methods
Patients
In this study, we summarized the data of 262 patients treated in the Otolaryngology Department of the China-Japan Friendship Hospital from February 2016 to August 2021 who had various types of laryngeal lesions. The patients were divided into 4 groups according to their diagnoses. Group 1 had 123 patients with suspected LPRD (they had abnormal results of reflux symptom index, or reflux finding score, or Dx-pH monitoring). Group 2 included 45 patients with vocal cord polyps. Group 3 had 40 patients with vocal cord leukoplakia. Group 4 included 54 patients with vocal cord carcinoma. All the diagnoses of the patients in Groups 2, 3, and 4 were confirmed by pathology after surgery (note: The pathological diagnosis of patients in vocal cord leukoplakia contains keratinization, hyperplasia, and mild or moderate or severe dysplasia of squamous cell in epithelium of vocal cord, with or without inflammation). The exclusion criteria included laryngeal infection, allergy, trauma, administration of proton pump inhibitors (PPIs) in the past 3 months, previous history of laryngeal surgery, radiation of the head and neck, diseases of the spine, and acupuncture treatment of the neck and head. All the patients had reflux symptom index (RSI) and reflux finding score (RFS) data and Dx-pH monitoring results.
Consent was obtained from each patient. This study was approved by the Ethics Committee of the China-Japan Friendship Hospital.
Reflux Symptom Index and Reflux Finding Score
According to Professor Belafsky, the symptoms and signs of LPRD can be assessed using the RSI and RFS.6,7 All the patients were asked to score their symptoms after they completely understood the meaning and method of the RSI scoring system. Two senior ENT physicians, who were blinded to all patients’ information, independently examined each patient with a transnasal Rhino-laryngo Videoscope (OLYMPUS ENF TYPE VH) with strobo (Atmos® Strobo 21 LED) and assigned an RFS to each patient (Strobo was used simultaneously to exclude scar, atrophy, and subtle paresis of vocal cord.). The average of the two RFS values was used as the RFS value of the patient. If a patient had an RSI > 13 and/or an RFS > 7, then that patient was considered to have an abnormal RSI/RFS; otherwise, the score was considered to be normal.
Dx-pH Monitoring
All the patients were subjected to 24-hour oropharynx pH monitoring with a Restech Dx-pH monitor. 8 The Dx-pH monitor was manufactured by Respiratory Technology Corporation (U.S.A.). When the monitor detected that the pH of the oropharynx was lower than 5.5 (upright) or 5.0 (supine), it recorded it as 1 episode of significant oropharyngeal pH change (severe acid oropharyngeal pH change episode). Changes of pH caused by eating or drinking were eliminated from the record. An upright Ryan score ≥ 9.41 (and/or a supine score ≥ 6.8) was considered to be an abnormal result, suggesting that the patient may have severe acid LPR. Then, the baseline of the Dx-pH monitor was changed to 6.5, and when the pH of the oropharynx decreased below 6.5, it was recorded and calculated (changes in pH caused by eating or drinking were eliminated from the record). If the frequency of pH below 6.5 was more than 3, the patient was also considered to have possible LPR. The episodes when the pH was between 6.5 and 5.5 (upright)/5.0 (supine) were considered weak acid oropharyngeal pH change episodes.
Statistics
SPSS software version 18.0 for Windows (IBM, Armonk, NY) was used to analyze the data. Chi-square tests, analysis of variance, and nonparametric tests were used for data analysis.
Results
Among the 262 patients, the youngest was 15 years old, and the oldest was 85 years old. The mean age was 51.36 (51.36 ± 15.34) years. The average ages of the patients in the 4 groups were 45.45 (45.45 ± 14.93), 45.62 (45.62 ± 12.51), 57.95 (57.95 ± 12.27), and 64.83 (64.83 ± 8.77) years. Significant differences were found among the 4 groups (P = .000). There were significant differences between Groups 1 and 3 (P = .000), Groups 1 and 4 (P = .000), Groups 2 and 3 (P = .000), Groups 2 and 4 (P = .000), and Groups 3 and 4 (P = .013). No significant difference was found between Groups 1 and 2 (P = .939).
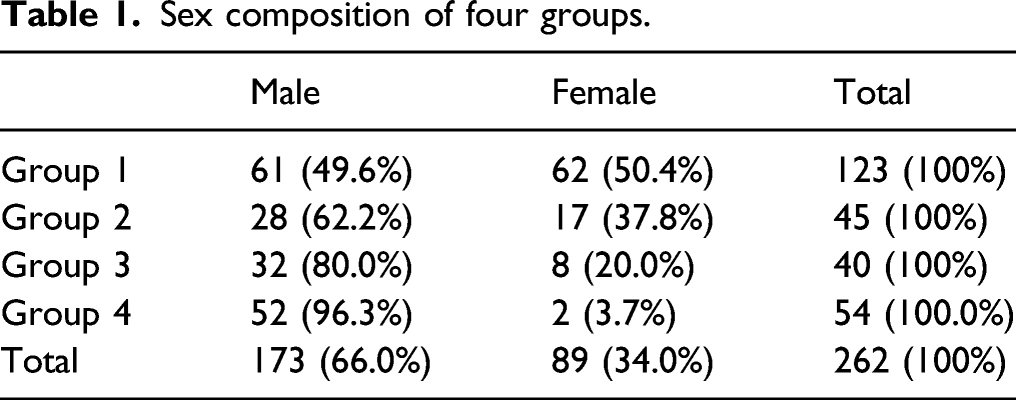
Sex composition of four groups.
The percentages of patients who had symptoms of gastroesophageal reflux disease, such as regurgitation and heartburn, were significantly different among the 4 groups (60.2%, 73.3%, 57.5%, and 40.7%, respectively, P = .011). There were significant differences between Groups 2 and 4 (P = .001), but no differences between the other groups (Groups 1 and 2: P = .148; Groups 1 and 3: P = .853; Groups 1 and 4: P = .022; Groups 2 and 3: P = .170; Groups 3 and 4: P = .144).
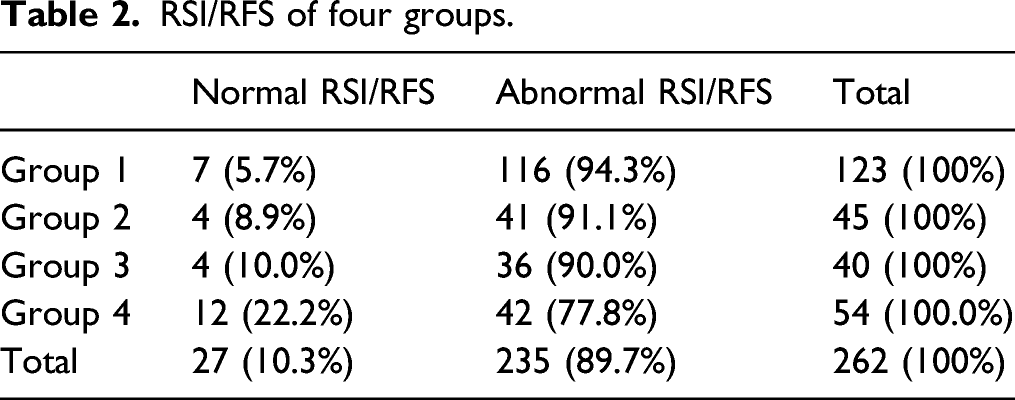
RSI/RFS of four groups.
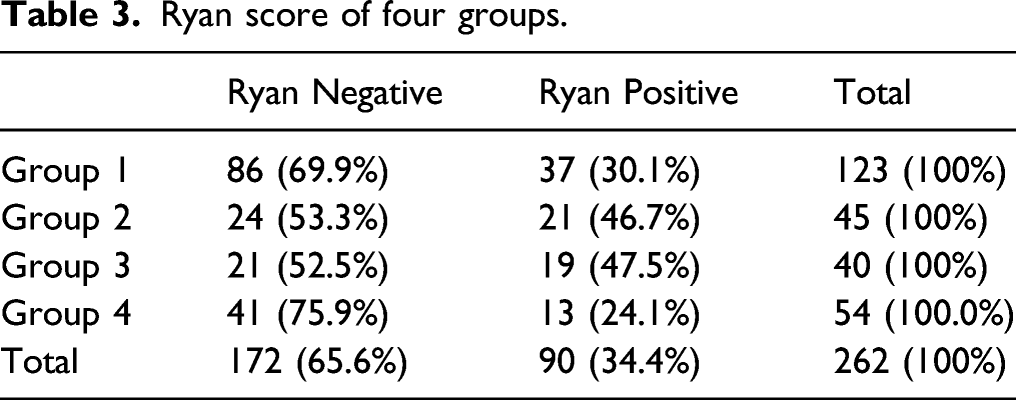
Ryan score of four groups.
There was a significant difference in upright Ryan scores among the 4 groups (Group 1: 21.87 ± 55.98; Group 2: 67.46 ± 141.91; Group 3: 98.49 ± 274.01; Group 4: 42.18 ± 140.74; P = .003). Significant differences were found between Groups 1 and 2 (P = .013), Groups 1 and 3 (P = .002), Groups 2 and 4 (P = .046), and Groups 3 and 4 (P = .009), but no obvious differences were found between Groups 1 and 4 (P = .951) or Groups 2 and 3 (P = .586). Additionally, there was no significant difference in supine Ryan score among the 4 groups (Group 1: 3.39 ± 4.10; Group 2: 2.95 ± 2.25; Group 3: 6.56 ± 15.23; Group 4: 3.18 ± 6.99; P = .837).
When the baseline of the Dx-pH monitor was changed to 6.5, there were 243 patients (243/262, 92.75%) who had more than 3 episodes of oropharyngeal pH below 6.5. The time percentage when the oropharyngeal pH was below 6.5 (represented by T1) was the proportion of time in which the oropharyngeal pH was below 6.5 relative to the total monitoring duration (episodes when the pH decreased below 6.5 due to drinking and eating were eliminated). T1 was considered the total time percentage probably caused by LPR. The time percentage when the oropharyngeal pH was below 5.5 (upright) or 5.0 (supine) was represented by T2, which may be caused by severe acid LPR. The difference between T1 and T2 (represented by T3) was the time percentage when the oropharyngeal pH was between 6.5 and 5.5 (upright) or 5.0 (supine), which may be caused by weak acid LPR. For time percentage of oropharyngeal pH of both upright 5.5∼6.5 (upright T3) and supine 5.0∼6.5 (supine T3), there were obvious differences among the 4 groups (Upright T3: Group 1: 18.08 ± 22.46; Group 2: 23.20 ± 26.46; Group 3: 31.48 ± 24.14; Group 4: 32.95 ± 32.45; P = .001. Supine T3: Group 1: 38.77 ± 32.03; Group 2: 47.04 ± 35.73; Group 3: 53.13 ± 31.55; Group 4: 51.19 ± 34.17; P = .033). Furthermore, significant differences in both upright and supine T3 were observed between Groups 1 and 3, Groups 1 and 4 (Upright T3: Groups 1 and 3: P = .017; Groups 1 and 4: P = .019. Supine T3: Groups 1 and 3: P = .018; Groups 1 and 4: P = .023). No difference was found between the other groups (Upright T3: Groups 1 and 2: P = .824; Groups 2 and 3: P = .582; Groups 2 and 4: P = .485; Groups 3 and 4: P = 1.000. Supine T3: Groups 1 and 2: P = .152; Groups 2 and 3: P = .398; Groups 2 and 4: P = .536; Groups 3 and 4: P = .780.).
Discussion
LPR is a common phenomenon observed in patients with various laryngeal diseases and may be one of their pathogenic factors.3,4 Acid and pepsin from gastric juice can damage laryngeal epithelium, respectively. 9 But with acid, pepsin has more damaging effect than pepsin alone. 9 Moreover, different pH levels can affect the activity of pepsin, which in turn affect the severity of damage of pepsin. 9 So different laryngeal and pharyngeal pH may be an important factor in pathogenesis of laryngeal diseases.
LPRD can change the pH of larynx and pharynx. Different laryngeal diseases may have different LPR and different oropharyngeal pH. Our previous study found that patients with vocal cord polyps or vocal cord leukoplakia were more likely to have abnormal RSI/RFS and Ryan scores than patients with vocal cord carcinoma. 5 In this article, we further summarized the different characteristics of oropharyngeal pH in patients with different laryngeal diseases to infer possible different role of LPR in them.
In the sequence of suspected LPRD, vocal cord polyps, vocal cord leukoplakia, and vocal cord carcinoma, the average age of the 4 groups increased gradually from benign disease to malignant lesion. There were significant differences of average age among the 4 groups, with one exception: no significant difference was found between patients with LPRD and vocal cord polyps. These results are consistent with our previous study and studies from other groups.5,10,11 Patients with benign phonotraumatic lesions were predominantly younger, and patients with glottic neoplasms were older, 10 while patients with vocal cord leukoplakia were the oldest group among the patients with benign vocal cord lesions. 11 Age was confirmed to be an independent risk factor associated with malignancy. 12
The percentage of male patients increased gradually according to the order of the groups. A male preponderance was observed in the later 3 groups. In particular, there were more male patients in the vocal cord leukoplakia and carcinoma group than in the LPRD and vocal cord polyp groups. It seems that males are more susceptible to vocal cord leukoplakia and laryngeal carcinoma. This is consistent with reported literature. 10
The RSI and RFS are widely used in clinical practice to evaluate the symptoms and signs of LPRD patients because of their simplicity, convenience, validity, and reliability.6,7 If a patient’s RSI is greater than 13 and/or RFS is greater than 7, the patient can be diagnosed with suspected LPRD. In this study, 235 (89.7%) patients in total had abnormal RSI/RFS values, indicating that most patients with laryngeal lesions had suspected LPRD and that LPR may play an important role in the pathogenesis of these lesions. The results were consistent with those in the literature.3,4 From Groups 1 to 4, the rates of abnormal RSI/RFS decreased gradually. LPRD patients had more symptoms and signs than the patients with the other three kinds of hypertrophic laryngeal diseases, and patients with benign hypertrophic laryngeal diseases had higher RSIs or RFSs than those with borderline and malignant hypertrophic laryngeal disease, although the only significant difference was observed between LPRD and laryngeal carcinoma patients. This is similar to our previous study. 5 The underlying mechanism is not clear. This may be because patients with hypertrophic laryngeal disease tend to have voice problems earlier due to hypertrophic lesions and visit the hospital in a timely manner before more symptoms emerge. However, further research is needed to draw a conclusion.
Dx-pH monitor is the only instrument specifically designed to record oropharyngeal pH, and this monitor can detect pH of both aerosolized and liquid environment.13-15 As this device is minimally invasive, sensitive to pH changes, more tolerated by patients, and easily manipulated, it is widely used to evaluate LPR. 16 In our study, 90 (34.35%) patients had abnormal Ryan scores. In other words, these patients had severe acid oropharyngeal pH change episodes, which indicated that severe acid LPR may occur in these patients. This result was consistent with other studies. 3 The rates of abnormal Ryan score of both the vocal cord polyp group and vocal cord leukoplakia group were significantly higher than those of the laryngeal carcinoma group, similar to our previous study. 5 It seemed that patients with vocal cord polyps and vocal cord leukoplakia may have more severe acid reflux than patients with laryngeal carcinoma. Further analysis of the Ryan scores confirmed this. The upright Ryan scores of the vocal cord polyps group and vocal cord leukoplakia group were significantly higher than those of the suspected LPRD group and laryngeal carcinoma group. There were no obvious differences between the suspected LPRD group and the laryngeal carcinoma group, vocal cord polyps group and vocal cord leukoplakia group. In addition, there were no marked differences in the supine Ryan scores among the 4 groups.
For weak acid LPR (pH between upright 5.5/supine 5.0 and 6.5), the condition was different. The normal average pH of the pharynx is 7.03, as measured by a Dx-pH monitor 17 ; hence, a transient pharyngeal pH below 6.5 except food and drinking is not completely normal and can be considered to be mostly caused by LPR. Since Ryan scores are designed to measure LPR episodes when the pH is lower than 5.5 (upright)/5.0 (supine), we compared the time percentage when the pharyngeal pH was between 5.5 (upright)/5.0 (supine) and 6.5 in order to evaluate weak acid LPR. This time percentage value in both upright and supine positions of patients in the vocal cord leukoplakia group and laryngeal carcinoma group was much higher than that of the suspected LPRD group. No obvious differences were found among the other groups. That is to say patients with vocal cord leukoplakia and laryngeal carcinoma experienced more weak acid oropharyngeal pH change episodes than suspected LPRD patients, which indicated that patients with vocal cord leukoplakia and laryngeal carcinoma may had more weak acid LPR than LPRD patients.
Overall, the pH values of oropharynx in different laryngeal diseases were not quite the same, which implied that the function and mechanism of LPR in different diseases may vary. 1) Compared to patients with suspected LPRD, patients with vocal cord polyps had more upright severe acid oropharyngeal pH change episodes, patients with laryngeal carcinoma had more upright and supine weak acid oropharyngeal pH change episodes, and patients with vocal cord leukoplakia had more severe and weak acid oropharyngeal pH change episodes. In other words, suspected LPRD patients had fewer oropharyngeal pH change episodes than patients with these 3 hypertrophic laryngeal diseases. Therefore, it is probable that mild and less LPR causes LPRD, and severe and more LPR may result in hypertrophic laryngeal disease, depending on the pH and number of LPR episodes, duration of LPR, and other essential cofactors. 2) Compared to patients with laryngeal carcinoma, patients with vocal cord polyps and vocal cord leukoplakia had more upright severe acid oropharyngeal pH change episodes. This can explain the phenomena we observed in the previous article [5]. It seemed that severe acid oropharyngeal pH change episodes may be less likely to contribute to the development of laryngeal carcinoma. In contrast, weak acid reflux may play a more important role in the pathogenesis of laryngeal carcinoma. Pepsin can damage all extragastric tissues at pH values up to 6. 18 Studies have reported that pepsin at pH 7.0 can promote carcinogenesis of the laryngeal tissue,19,20 which indicates the role of the nonacid environment in the mechanism of carcinoma. This indirectly verifies our results. 3) Neither severe acid oropharyngeal pH change episodes nor weak acid oropharyngeal pH change episode showed significant differences between patients with vocal cord polyps and vocal cord leukoplakia. There should be some other factors to determine the progress of these lesions, such as age, as we found in this study, and other unknown elements.
There is a key point to illustrate. What is recorded by Dx-pH monitoring is oropharyngeal pH, not LPR itself directly. So oropharyngeal pH does not equal to LPR. The oropharyngeal pH is affected by bacteria, salivary secretion, LPR, food and drinking, and so on. 15 When the factor of food and drinking is eliminated, LPR may be the most reasonable reason for the temporary drop of oropharyngeal pH and associated with LPRD symptoms. 15 So oropharyngeal pH can reflect LPR indirectly to some degree at least.
Certainly, this study had some limitations, such as the limited sample size and the disadvantages of the RSI, RFS, and Dx-pH monitoring. Dx-pH monitoring cannot record non-acid reflux which may be important in pathogenesis. Hypopharyngeal-esophageal multichannel intraluminal impedance with dual pH testing may compensate this and can be a better supplement in future studies. Pepsin and bile salts, which are significant in the damage caused by reflux contents, were not included in this study. However, this is the first report of different oropharyngeal pH change patterns in patients with different laryngeal diseases.
In conclusion, the average age and percentage of male patients increased in the following order: suspected LPRD, vocal cord polyps, vocal cord leukoplakia, and laryngeal carcinoma. Most patients had abnormal RSI/RFS, and some patients had abnormal Ryan scores. Most patients had more episodes with oropharyngeal pH lower than 6.5, which indicated that LPR may play an important role in the pathogenesis of these laryngeal diseases. However, there were different oropharyngeal pH patterns in different laryngeal diseases. Compared to patients with suspected LPRD, patients with vocal cord polyps had more upright severe acid oropharyngeal pH change episodes, patients with laryngeal carcinoma had more upright and supine weak acid oropharyngeal pH change episodes, and patients with vocal cord leukoplakia had more severe and weak acid oropharyngeal pH change episodes. Patients with vocal cord polyps and vocal cord leukoplakia had more severe acid oropharyngeal pH change episodes than patients with laryngeal carcinoma. There were no significant differences between patients with vocal cord polyps and vocal cord leukoplakia, regardless of severe or weak acid oropharyngeal pH change episodes. Hence, further research is needed.
Footnotes
Acknowledgments
The authors thank the colleagues of Gastroenterology department of China-Japan Friendship Hospital for their help in the oropharynx pH monitoring.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.