
Abstract
Traumatic temporal bone fractures with parapharyngeal emphysema represent a rare clinical entity with potential serious complications. This retrospective case series has taken 3 cases of traumatic temporal bone fractures with parapharyngeal emphysema and has examined their clinical presentation, management, and outcomes. Recognizing warning signs and managing them accordingly is vital to prevent the occurrence of problems such as airway compromise and deep-neck space infections. A multidisciplinary team consisting of otolaryngologists and oral and maxillofacial surgeons should be considered as a vital element in the process of improving the outcome of patients.
Introduction
The temporal bones are paired structures located on the lateral aspects of the skull and contribute to the skull base. 1 Temporal bone fractures, often resulting from high-energy head trauma, automobile accidents, and pressure injuries.2,3 It can lead to a range of clinical complications, including hearing loss, cranial nerve injury, especially facial nerve, traumatic brain, middle and internal ear injury, and cerebrospinal fluid leakage.2,4,5 Traumatic temporal bone fractures are believed to occur in 14%-22% of all calvarial fractures, with a prevalence of 3% of all trauma patients in 1 series. 6
Traumatic temporal bone fracture with parapharyngeal emphysema represents a unique clinical entity characterized by temporal bone fractures accompanied by the presence of air in the parapharyngeal space.7,8 The parapharyngeal space is one of the deep spaces of the upper neck. This space is located lateral to the pharynx and medial to the ramus of the mandible, the pterygoid muscles, and the parotid gland. 9 The presence of parapharyngeal emphysema raises concerns about further complications, including airway compromise, difficulty swallowing, and the risk of deep-neck infections due to its proximity to the upper aerodigestive tract and its communication with deep-neck spaces. 10 Given the rarity of parapharyngeal emphysema secondary to traumatic temporal fractures, there is limited literature available on its optimal treatment.
In this case series, we will provide an insight into the clinical course and treatment outcomes of this condition. Through the review of these cases and literature, our goal was to improve the understanding and awareness of health care providers in the evaluation and management of temporal fractures with parapharyngeal emphysema.
Case 1
A 10 year-old Sudanese boy, not known to have any medical condition, was brought to the emergency department (ED) by his father 5 hours after falling while playing football. No witness was available to inquire about the details of the event; however, the family was informed that their son had lost consciousness for around 2 minutes after a fall on his head. He also had an episode of vomiting afterward and was unable to recall the event. The patient had no other neurological symptoms, including headaches, weakness, numbness, or change in vision. He complained of pain in the right ear, associated with mild bleeding on the same side. However, there was no change in hearing level or tinnitus. On arrival in the ED, the patient was alert, conscious, and oriented with stable vital signs and unremarkable examination except for bleeding from the right external auditory canal. A contrast-free CT head was performed, which showed no evidence of intracranial bleeding or injury, but was positive for right otic-sparing temporal bone fracture traversing the temporomandibular joint (TMJ) and the tympanic part of the temporal bone with small amount of effusion in mastoid air cells and right deep-neck space emphysema reaching parapharyngeal space (Figure 1).
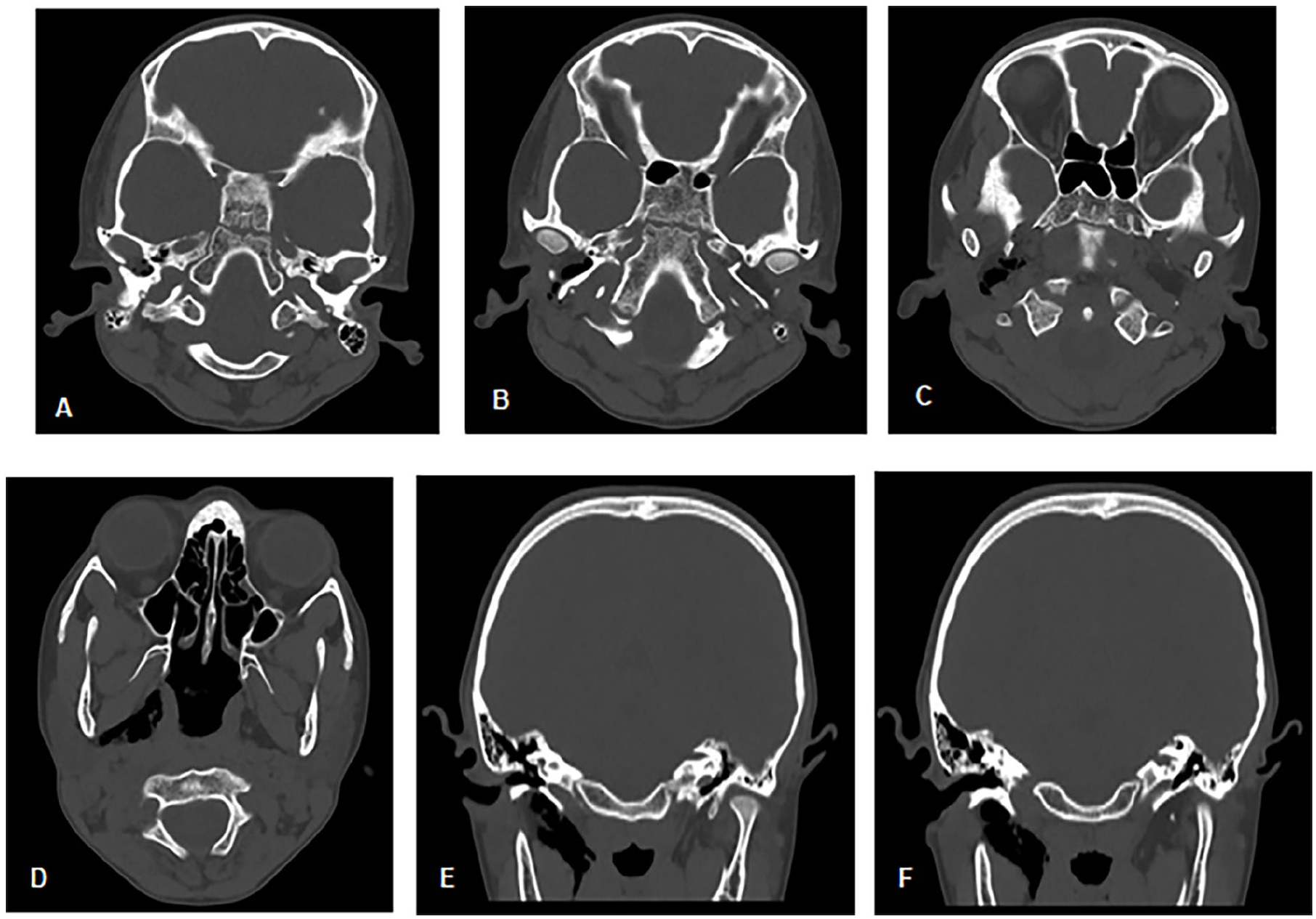
CT head images showing right otic-sparing temporal bone fracture traversing the temporomandibular joint and tympanic part of the temporal bone with parapharyngeal space emphysema. (A-D) Axial cuts from superior to inferior tracing the tract of emphysema from the fracture line to the parapharyngeal space. (E, F) Coronal cuts showing deep-neck space emphysema.
The patient was seen by the neurosurgery team for traumatic brain injury, which was treated conservatively. He was also referred to otolaryngology for temporal bone fracture. The history was negative for airway symptoms, dysphagia, odynophagia, or pain over the TMJ. A detailed examination did not show signs of respiratory distress or swelling of the face or neck. Flexible nasolaryngoscopy (FNLS) showed a patent airway without bulging in the pharyngeal walls. Evaluation of the ears showed an unremarkable left ear examination. Examination of the right ear showed lacerated external auditory canal skin anterior-inferiorly on the lateral aspect of the canal and a small central anterior-superior tympanic membrane perforation. The evaluation using a tuning fork was unremarkable.
The patient was admitted to the hospital to observe the airway symptoms and was covered with analgesia and systemic antibiotics to prevent deep-neck infections. The lacerated canal skin was re-draped into its anatomical position, and an otowick soaked with fluoroquinolone was inserted in the canal to preserve its patency. The oral and maxillofacial (OMF) team was consulted for TMJ involvement, and conservative management was recommended. The patient was doing well during his hospital stay and was discharged after 48 hours with instructions to return to ED in case of airway symptoms. He was covered with systemic antibiotics (amoxicillin and clavulanic acid) for 7 days and topical antibiotic ear drops (fluoroquinolone) for 10 days. The patient was given a follow-up appointment after 5 days for the removal of the otowick; however, he missed his appointment and was seen 10 days after discharge. The otowick was removed with a healed laceration and persistent perforation of the tympanic membrane. Audiological evaluation was performed and mild conductive hearing loss was found on the right side and normal hearing on the left. The family was advised to continue with water precautions with a 3 month follow-up appointment and to repeat CT to reassess parapharyngeal emphysema. However, the family refused to repeat the CT scan due to lack of symptoms, radiation risk, and financial reasons.
Case 2
A 24 year-old Pakistani man, medically free, came to the ED with a history of accidental fall of 3 m height. The main impact was on the right shoulder and the temporal surface of the head. The patient lost consciousness for 1 minute and had 2 episodes of vomiting after the incident. However, there were no other neurological problems. Upon arrival in the ED, the patient was alert, conscious, and oriented. Primary and secondary surveys were unremarkable except for clotted blood in the right ear. Head and cervical spine CT was performed and revealed no intracranial pathologies; however, a non-displaced fracture of the tympanic part of the right temporal bone involving the anterior wall of the right external auditory canal and extended into mastoid air cells with multiple air foci seen within the right parapharyngeal space was noted (Figure 2).
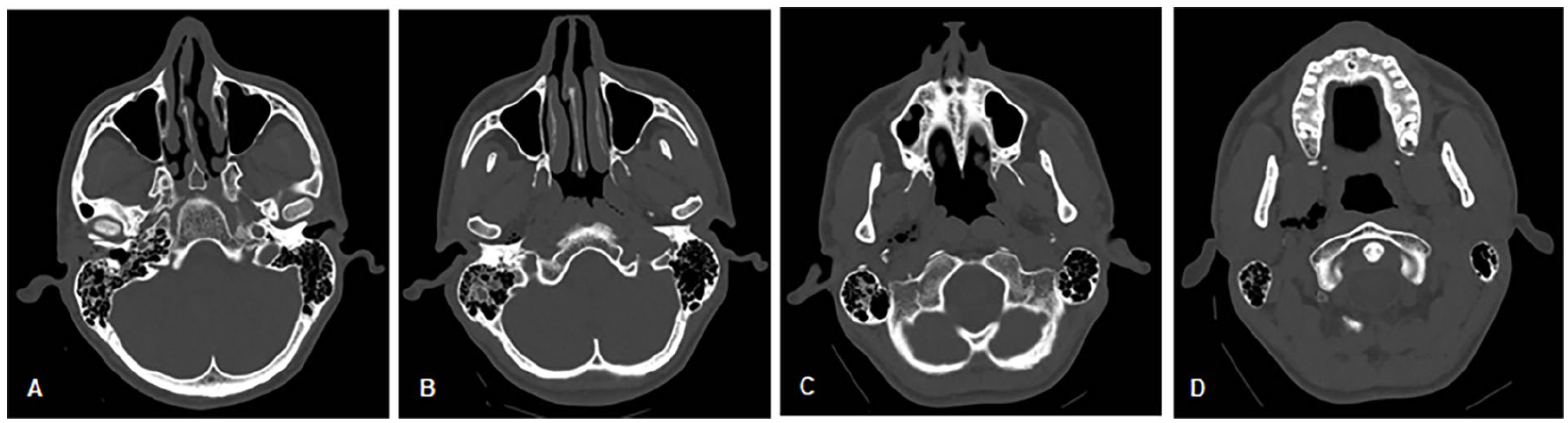
CT head axial cuts showing non-displaced fracture of the tympanic part of the right temporal bone involving the anterior wall of the right external auditory canal and extending into the mastoid air cells with multiple air foci extending into the right parapharyngeal space. From most superior to most inferior (A to D).
The patient was evaluated by the neurosurgery team, given instructions on head trauma, and started conservative treatment. He was also seen by orthopedic and otolaryngology teams for acromioclavicular subluxation and right temporal bone fracture, respectively. The detailed history was positive for bleeding in the right ear that had stopped spontaneously, decreased hearing on the right side, and otalgia. He had no other otologic or respiratory symptoms. Examination of the right ear showed a small auricular hematoma, lacerated meatal skin wall anterior-inferiorly, and intact tympanic membrane with hemotympanum. The Rinne test was bilaterally positive and the Weber test lateralized to the right. Oral examination did not show trismus and FNLS confirmed airway patency.
The lacerated skin was placed in its anatomical position, the auricular hematoma was aspirated, and a pressure dressing was applied. The patient was admitted to the hospital for 48 hours to observe airway symptoms and started on systemic and topical antibiotics in addition to analgesia. Tetanus toxoid vaccination was administered. The OMF team was consulted for TMJ involvement, which was treated conservatively in the form of soft diet and physiotherapy. The pressure dressing was removed after 24 hours. During his admission, the patient did not show signs of respiratory distress with stable vital signs. He was discharged home after 48 hours with an outpatient appointment in 3 weeks. However, the patient did not attend his follow-up appointment for social and financial reasons.
Case 3
A 47 year-old Pakistani male, previously medically and surgically free, came to the ED with a history of falling from a 3 m ladder over the right side of his body. The patient presented with chest and shoulder pain on the right side, bleeding from the right ear, and a small occipital wound. There was no history of amnesia or loss of consciousness. He had an episode of vomiting in the ED. The trauma team was involved, and the primary and secondary surveys were reassuring except for right shoulder deformity, small occipital cut wound, and bleeding from the right ear. The wound was sutured and pan-CT was performed. CT brain without contrast showed supratentorial subarachnoid hemorrhage (SAH) more on the left side with a small extra-axial left temporal area of hemorrhage. Right basisphenoid and temporal bone fracture involved the petrous apex with soft tissue emphysema reaching the parapharyngeal space. Opacified right sphenoid sinus was suggestive of hemosinus with suspicions of involvement of the right internal carotid artery (ICA) canal (Figure 3). CT chest, abdomen, and pelvis without contrast showed no injuries except for posterior displacement of L5 over S1 vertebra, and anterior displacement of L4 over L5 vertebra with non-displaced fracture of the posterior arch of L4 and right acromioclavicular dislocation.
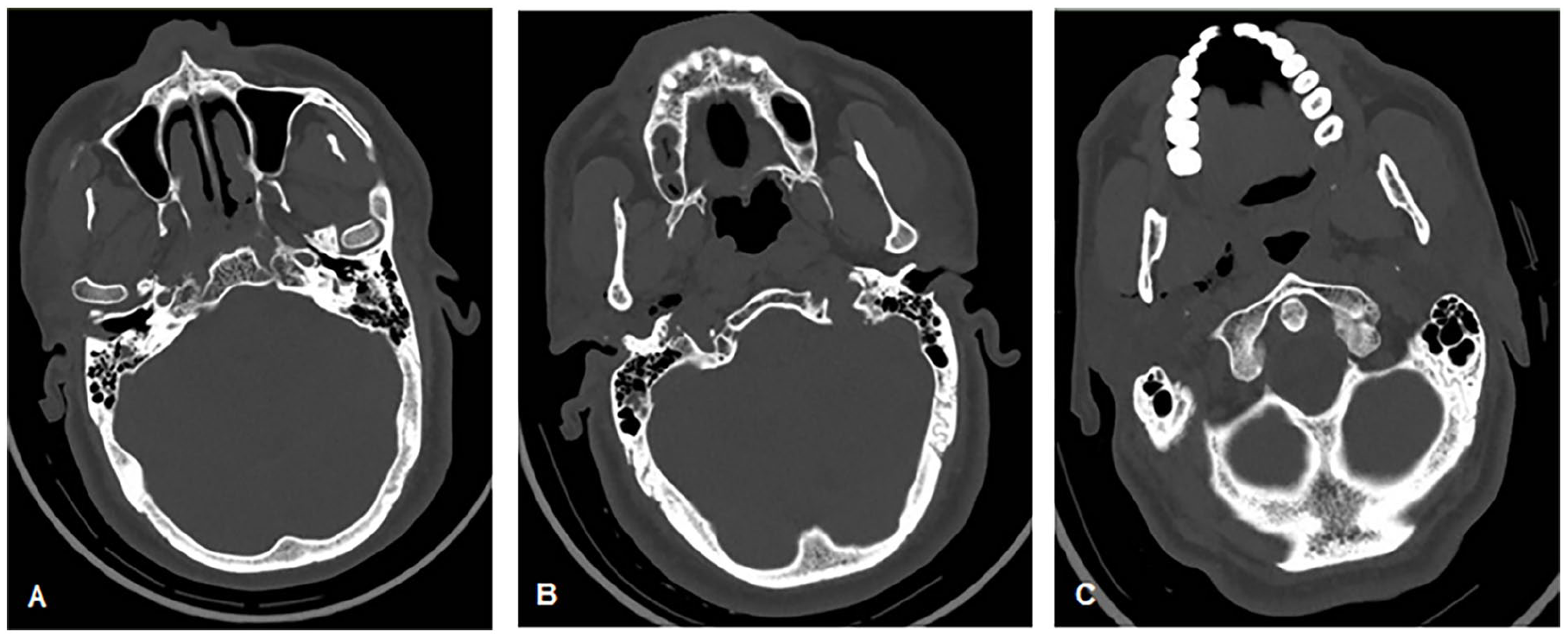
CT head axial cuts fracture of the tympanic part of the right temporal bone involving the anterior wall of the right external auditory with right parapharyngeal space emphysema. (A-C) From superior to inferior.
Urgent CT angiography (CTA) of the brain was performed and showed subtle outline irregularities in the distal portion of the petrous segment of the ICA bilaterally with no extravasation or signs of vascular injury. Parapharyngeal space emphysema progression was also observed in the CTA, which was performed 6 hours after the initial brain CT (Figure 4).
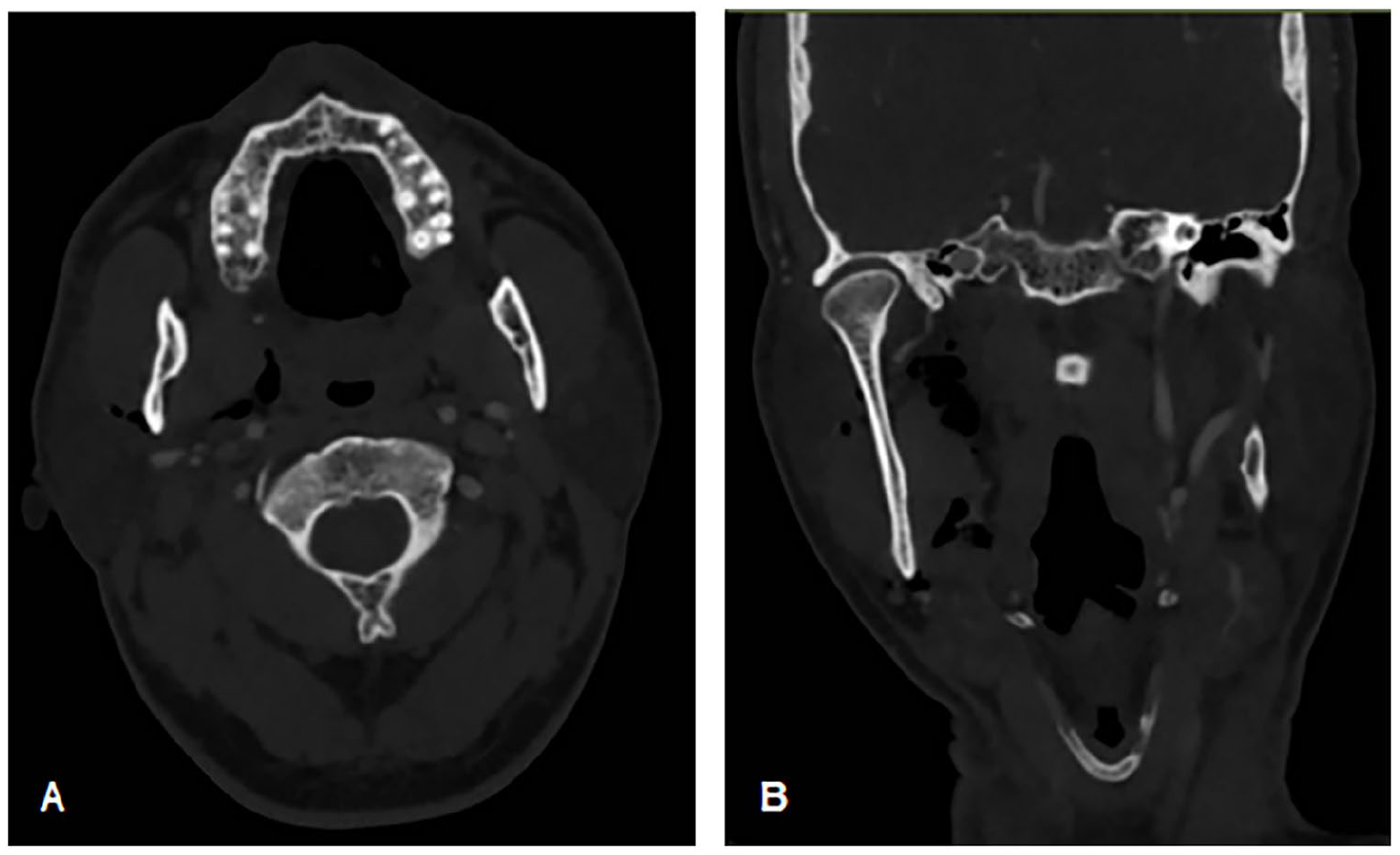
CT angiography of the brain showing the progression of right parapharyngeal emphysema. (A) Axial cut, (B) coronal cut.
The patient was admitted to the hospital for observation. He was followed by multiple teams: neurosurgery for SAH, orthopedics for spinal and acromioclavicular joint injury, and otolaryngology for right temporal bone fracture.
The patient was evaluated for right temporal bone fracture by the otolaryngology team. He had no active ear bleeding at the time of evaluation. The patient had no changes in hearing, tinnitus, otorrhea, or facial weakness. He had no difficulty breathing, shortness of breath, stridor, dysphagia, or odynophagia. Upon examination, the external auditory canal was patent and the tympanic membrane was clear, with bilaterally-positive Rinne test, centralized Weber test and bilateral grade 1 facial nerve mobility on the House-Brackmann grading system. FNLS showed patent airway.
The patient was admitted for 6 days for the management of the right acromioclavicular joint dislocation. During his hospital stay, the patient continued to have no airway complaints. He received systemic antibiotics (Ceftriaxone), analgesia, and tetanus vaccination. A patient was given a follow-up appointment with the otolaryngology clinic 6 weeks after discharge.
Discussion
The temporal bone, which is a complex paired structure within the skull base that houses several important structures such as the cranial nerves, major vascular structures, the middle ear ossicles, and the labyrinth. Temporal bone is made up of 4 separate osseous segments: tympanic, mastoid, petrous, and squamous. 1 Temporal bone fractures can result from a variety of high-energy traumatic incidents, including motor vehicle accidents, falls, and direct trauma to the head or face.2,3 These fractures may involve different parts of the temporal bone, including the squamous, petrous, mastoid, and tympanic parts. Depending on the mechanism of injury, temporal bone fractures can be classified into longitudinal, transverse, or mixed patterns, each with its own implications for clinical management and outcomes. 10
The parapharyngeal space is a crucial anatomical region located lateral to the pharynx and medial to the deep spaces of the neck. It is bounded by several structures, including the medial pterygoid muscle anteriorly, the prevertebral fascia posteriorly, the styloid process and the carotid sheath laterally, and the base of the skull superiorly, and it is divided into prestyloid and poststyloid (retrostyloid) compartments. This space communicates with other critical neck spaces, including the retropharyngeal, masticator, and carotid spaces.11,12
After a thorough review of the literature, as well as the cases presented in this series, we observed that parapharyngeal emphysema was associated with temporal bone fracture when the fracture line affects the tympanic part and the anterior meatal wall, allowing air entrapment from the external canal into the parapharyngeal space. Fracture in the skin of the anterior meatal wall may cause the spread of infection into the parapharyngeal space and then into the communicating spaces of the neck, which can lead to fatal complications if not recognized early and treated appropriately. In addition, there is a theoretical risk of airway compromise if the size of the emphysema increases sufficiently to obstruct the upper airway or if it extends to involve the peri-laryngeal and perihypopharyngeal spaces. 7 These patients may initially present with dysphagia that precedes airway symptoms.
Temporal bone fracture complicated by parapharyngeal emphysema was first described by Plaza et al. 7 This case has been treated conservatively, where the patient was admitted for observation for 5 days, followed by a repeated CT showing complete resolution of the emphysema. The latest literature that described this unusual presentation of temporal bone was published in 2013 by de Matos et al. 6 Again, the patient was treated conservatively with complete recovery after 2 weeks.
When treating these patients, it is important to address other injuries that may be associated with the fracture, including external auditory canal lacerations that can result in canal stenosis. It is also essential to involve the OMF team to address the involvement of the TMJ and begin preventive measures to decrease the risk of joint complications. Moreover, a short course of systemic antibiotics may be justified as prophylaxis against deep-neck space infections. More importantly, it is crucial to educate patients about possible complications and to give them clear instructions regarding red flags that require a visit to ED.
It should be noted that the presence of parapharyngeal emphysema can aid in the diagnosis of temporal bone fracture, since it serves as a radiological sign that raises the suspicion of facial fractures. However, there are other causes that could result in parapharyngeal emphysema, including bilateral styloid process fracture, 13 orbitozygomatic fracture, 14 parapharyngeal tumors through airway erosion, 15 iatrogenic injury during surgical or procedural manipulation,16,17 and mediastinal emphysema. 18
This case series underscores the importance of prompt recognition and appropriate management of parapharyngeal emphysema that results from temporal bone fracture to prevent potential complications such as airway compromise and deep-neck space infections. Furthermore, the interdisciplinary approach involving otolaryngologists, trauma surgeons, and oral OMF surgeons is essential to coordinate care and optimize outcomes in these cases. Finally, it is important to always explore the potential causes of parapharyngeal emphysema once it has been identified radiologically.
Conclusion
Traumatic temporal bone fractures with parapharyngeal emphysema are rare, but can cause serious complications. Early diagnosis and appropriate imaging are very important to reduce risks and obtain the best results. This case series highlights the need for a systematic multidisciplinary approach between health care providers to deal with these cases. Additional studies are required to increase understanding and awareness of this rare entity among medical professionals and to propose a specific protocol for its management.
Footnotes
Ethical Considerations
Our institution does not require ethics approval for reporting individual cases.
Consent to Participate
Written informed consent for participation was obtained from the patients (cases 2 and 3) and the patient’s legally-authorized representative (case 1) with an emphasis on keeping all personal information anonymous
Consent for Publication
Written informed consent for publication was obtained from the patients.
Author contributions
Lana Saleh: Conceptualization and design, acquisition of data, drafting of the manuscript, critical review of the manuscript, supervision, and coordination. Ali H. Hasan: Conceptualization and design, acquisition of data, drafting of the manuscript, and critical review of the manuscript. Razan M. Saleh: Acquisition of data, drafting of the manuscript, and critical review of the manuscript. Ahmed Saleh: Acquisition of data, drafting of the manuscript, and critical review of the manuscript. Yasser G. Alarimah: Conceptualization and design, acquisition of data, and critical review of the manuscript. Fahad N. Altamimi: Conceptualization and design, critical review of the manuscript, supervision, and coordination.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are openly available in a public repository.