
Abstract
Introduction:
Auricular keloids may be associated with social stigma and impair patients’ quality of life (QoL) significantly. Little is known about the effect of different therapeutic concepts on the patient’s QoL. This study aims to investigate the QoL in patients with auricular keloids undergoing a specific multimodal therapeutic regimen.
Materials and Methods:
Patients suffering from auricular keloids were treated by a multimodal treatment comprising surgical excision, intralesional triamcinolone acetonide, and subsequent application of customized magnetic pressure splints. A prospective assessment of QoL was conducted using the validated Keloid Intervention Benefit Inventory-21 questionnaire at three time points.
Results:
In total, 22 auricular keloids were included in our study. All patients completed a comprehensive 1-year follow-up assessment, with an average follow-up duration of 29 months post-surgery. Quantitative analysis of QoL metrics demonstrated significant improvement of QoL at the three times of measurement (P < .0001). Significant results were also found for the subcategories general health, physical health, social interaction, and self-esteem.
Conclusion:
This study underscores the necessity of assessment of QoL in keloid treatment. Our findings highlight the advantages of multimodal treatment in enhancing patients’ QoL throughout the treatment period and managing auricular keloids with low recurrence.
Trial Registration:
The study was registered at the German Clinical Trials Register (Register ID: DRKS00016348, https://drks.de/search/en/trial/DRKS00016348).
Introduction
Keloids are characterized by abnormal proliferation and deposition of collagen with an overgrowth of scar tissue. They often result from a dysregulated wound-healing process after a cutaneous tissue injury. Unlike hypertrophic scars, keloid scars grow continuously beyond the margins of the initial wound with no tendency toward spontaneous regression.1,2 The underlying mechanisms are still not completely understood. As keloids cannot be found in animals, classical experimental research models cannot be used in keloid research. 3 Nevertheless, according to the current state of knowledge, the influencing factors include high skin pigmentation, mechanical stress, and specific anatomical areas with high skin tension and low skin mobility. Thus, keloid formations are primarily located on the chest, upper back, and shoulders, and in the head and neck region around the ear lobule or the back surface of the pinna.2,4,5 Other risk factors are a prolonged inflammatory reaction, tension on the wound, and psychological stress.6-10
Keloids in the head and neck region are particularly prone to stigmatization due to their exposed localization. Therefore, successful therapies with long-term disease control are important for improving the quality of life (QoL) of patients with keloids. 11 QoL has become an important outcome parameter for both the need for therapy and the assessment of therapeutic interventions for chronic diseases.12,13 This is plausible, as in non-life-threatening diseases, such as keloids, not only physical condition but also mental and psychological status and interventions’ impact on daily activities and social life affect patients’ perceptions of long-term outcomes. Several studies have demonstrated the negative impacts of chronic skin diseases, such as atopic dermatitis, psoriasis, and scleroderma, on patients’ QoL.13-16 QoL impairment in such conditions can even be compared to that caused by life-threatening diseases, such as chronic heart failure.
Keloids can also significantly impair patients’ QoL. 17 QoL measurements in patients with hypertrophic scars or keloids have been performed by repurposing or adapting existing questionnaires. A systematic review by Lyons et al concluded that the variety in keloid outcome measures leads to disparities in the analysis of the numerous treatment methods. 18 A tool has also been specifically designed to assess the impact of keloids in the head and neck region on QoL: the Keloid Intervention Benefit Inventory-21 (KIBI-21). 19
No international consensus exists about the best monotherapy or combination therapy for keloids. The most well-known and commonly used first-line monotherapy for small keloids is triamcinolone acetonide (TAC) in doses of 10 to 40 mg/ml. 20 However, TAC monotherapy has recurrence rates of 33% and 50% after 1 and 5 years, respectively.21,22 Nevertheless, a meta-analysis found that TAC was superior to verapamil, silicone gel sheeting, and cryotherapy in terms of keloid size reduction. 20 For cryotherapy, a volume reduction of 67% after 1.5 years and a response rate of 50% to 76% are described in the literature.23,24 Furthermore, a prospective study reported that a combination therapy of TAC and CO2 laser had a recurrence rate of 11.7% 6 months after treatment. 25 To prevent recurrence in larger keloids, a combination of therapies is recommended by most experts, as surgical excision alone has a recurrence rate of 40% to 100%.26,27 For auricular keloids, Bran suggested a triple therapy consisting of intramarginal excision, intralesional TAC injections (40 mg/dl) every 4 to 6 weeks for 6 months, and a pressure splint for at least 5 nights a week for 6 months. 28 However, most studies have not assessed recurrence rates after more than 1 year postoperatively. The best long-term results regarding disease control evaluated through recurrence rates have been reported after 5 years for surgical resection and radiotherapy (10%-22%), surgical resection followed by TAC injections (8%-50%), and the described multimodal treatment by Bran et al (18%).22,28,29,30 The 3 described treatments have in common that volume reduction and esthetic reconstruction are achieved by surgical resection and long-term recurrence shall be prevented by consecutive anti-inflammatory treatments. Moreover, little is known about the long-term impact of treatments on QoL. Furthermore, for the single components of multimodal treatments, there are no data based on which it can be determined which component of the therapeutic regimen has the greatest impact on QoL.
The aim of this study was to investigate the QoL trajectories of patients with auricular keloids undergoing the multimodal treatment method described by Bran. Furthermore, the study aimed to assess the impacts of the 3 components of this therapy on patients’ QoL as measured by the KIBI-21. 28
Materials and Methods
This prospective single-center study was conducted at the Department of Otorhinolaryngology—Head and Neck Surgery, Division of Facial Plastic and Reconstructive Surgery, between June 2019 and September 2021. The study protocol was approved by the Ethics Board of the Medical Faculty (2018-645N-MA). The trial was registered in the German Clinical Trials Register (Register ID: DRKS00016348). All participants provided written informed consent. Only patients who were able to provide fully informed consent were included in the study.
All participants had auricular keloid formations and underwent a multimodal treatment regimen. The therapy consisted of intramarginal resection with primary wound closure, intralesional injections of TAC (40 mg/ml) every 4 to 6 weeks over a period of 6 months (a total of 6 injections), and a customized magnetic pressure splint applied 6 months after the injections. The patients were asked to wear the splint at least 5 nights a week over a period of 6 months. Surgical excision and intralesional injections were performed in our outpatient office. The customized pressure splint was adjusted using a cooperating epithetist.
The patients were asked to complete the KIBI-21 3 times to assess QoL under therapy. This validated tool for assessing QoL in patients with auricular keloids consists of 4 subscales: general health (GH), physical health (PH), social impact (SI), and self-esteem (SE). The questions are designed in such a way that they can be answered adequately before and after medical interventions. The items are rated on a five-point Likert scale. The total score ranges from −100 to 100. Higher scores indicate better QoL.19,30 QoL was assessed before surgery (N1), after surgery and the 6-month intralesional corticosteroid therapy (N2), and after the subsequent splint therapy—that is, 12 months postoperatively (N3). Follow-up examinations were performed every 4 to 6 weeks after surgery and throughout the intralesional injection therapy. Afterward, examinations were performed every 6 months or according to each patient’s needs. The skin type was characterized according to the Fitzpatrick Skin Scale.
Statistical analysis was performed using SAS version 9.2 (SAS Institute, Cary, NC, USA) and JMP version 15 (JMP Statistical Discovery LLC, Cary, NC, USA). P < .05 were considered statistically significant.
Results
A total of 15 patients with an average age of 26 years (range: 16-70 years) were included in this study. Three patients (20%) were male and 12 (80%) were female. All patients completed the 1-year follow-up. Complete intralesional resection of the keloid formation was achieved in all cases. The mean follow-up period after surgery was 29 months (range: 13-49 months). After the last patient completed the structured follow-up period and before closing the data collection, all patients were interviewed about clinical conditions and recurrence of keloids. Eight patients had bilateral auricular keloids. Thus, a total of 22 keloids were treated. Fifteen keloids were distributed in the lobule area, and 7 were distributed along the helix. In 2 cases, the keloids resulted from trauma or tumor resection. In all other cases, they developed after ear piercing. Five patients (33%) had type II skin, 7 (47%) had type III skin, and 3 (20%) had type IV skin. Eight patients had undergone at least 1 previous treatment in the treated area. Four patients underwent surgical resection, 2 of them even 2 resections. One patient reported surgical resection followed by intralesional steroid injections. Three patients showed recurrence of their keloids after undergoing cryosurgery. The patients’ demographic characteristics are shown in Table 1. Pictures of the treatment process can be found in the supplement material section (Figures 3 and 4).
Distribution of Characteristics of the Patient Collective.

All patients completed the 6-month TAC therapy after local surgical removal. Only 2 patients (13%) did not wear a customized magnetic pressure splint as recommended. All patients underwent the scheduled follow-up examinations and completed the KIBI-21. No recurrence of the keloid was found throughout the follow-up period. Therefore, no sub-analysis was possible for those patients who did not wear a customized pressure splint.
The overall mean KIBI-21 scores after surgery and TAC therapy (N2: 35.28) and upon treatment completion (N3: 40.77) increased significantly compared to those before surgery (N1: −−25.56; both P < .0001). The mean GH scores were −4.23 ± 3.8 at N1, 36.28 ± 16.5 at N2, and 6.2 ± 3.1 at N3. The differences between N1 and N2 and between N1 and N3 were statistically significant (both P < .0001). Similarly, statistically significant differences were observed between N1 and N2 and between N1 and N3 in terms of PH (both P < .0001). The mean PH scores were −8.2 ± 7.7 at N1, 10.51 ± 8.7 at N2, and 14.3 ± 5.5 at N3. The mean SI scores were 0.38 ± 1.9 at N1, 2.14 ± 2.7 at N2, and 3.97 ± 5.0 at N3. The differences between N1 and N2 and between N1 and N3 were also statistically significant (P < .0001 and P = .01, respectively). Statistically significant differences were also observed between N1 and N2 and between N1 and N3 in terms of SE (both P < .0001), with mean scores of −13.59 ± 10.7 at N1, 19.28 ± 10.0 at N2, and 27.71 ± 11.0 at N3. Details are shown in Table 2.
Comparison of the Mean Values of the Results of the KIBI-21 and Comparison at Different Times of Assessment.
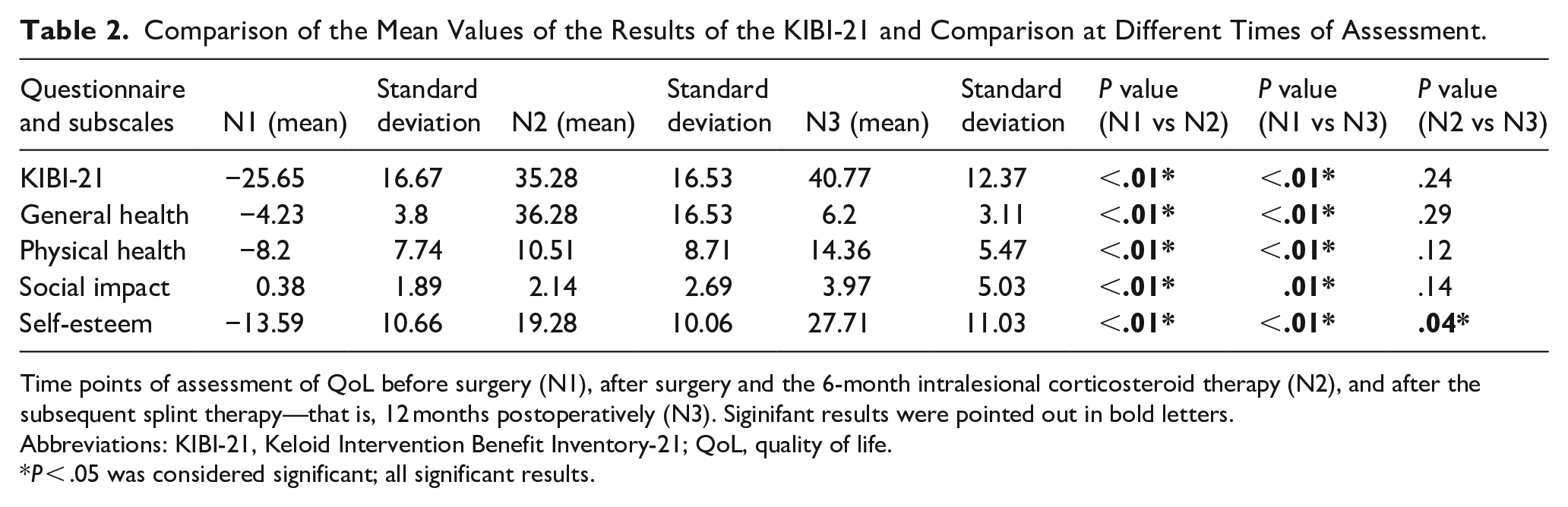
Time points of assessment of QoL before surgery (N1), after surgery and the 6-month intralesional corticosteroid therapy (N2), and after the subsequent splint therapy—that is, 12 months postoperatively (N3). Siginifant results were pointed out in bold letters.
Abbreviations: KIBI-21, Keloid Intervention Benefit Inventory-21; QoL, quality of life.
P < .05 was considered significant; all significant results.
SE also improved significantly at N3 compared to N2 (P < .036). Conversely, PH and SI did not show statistically significant improvements at N3 compared to N2, and the GH scores showed a decrease at N3 compared to N2. The results are shown in Figures 1 and 2.
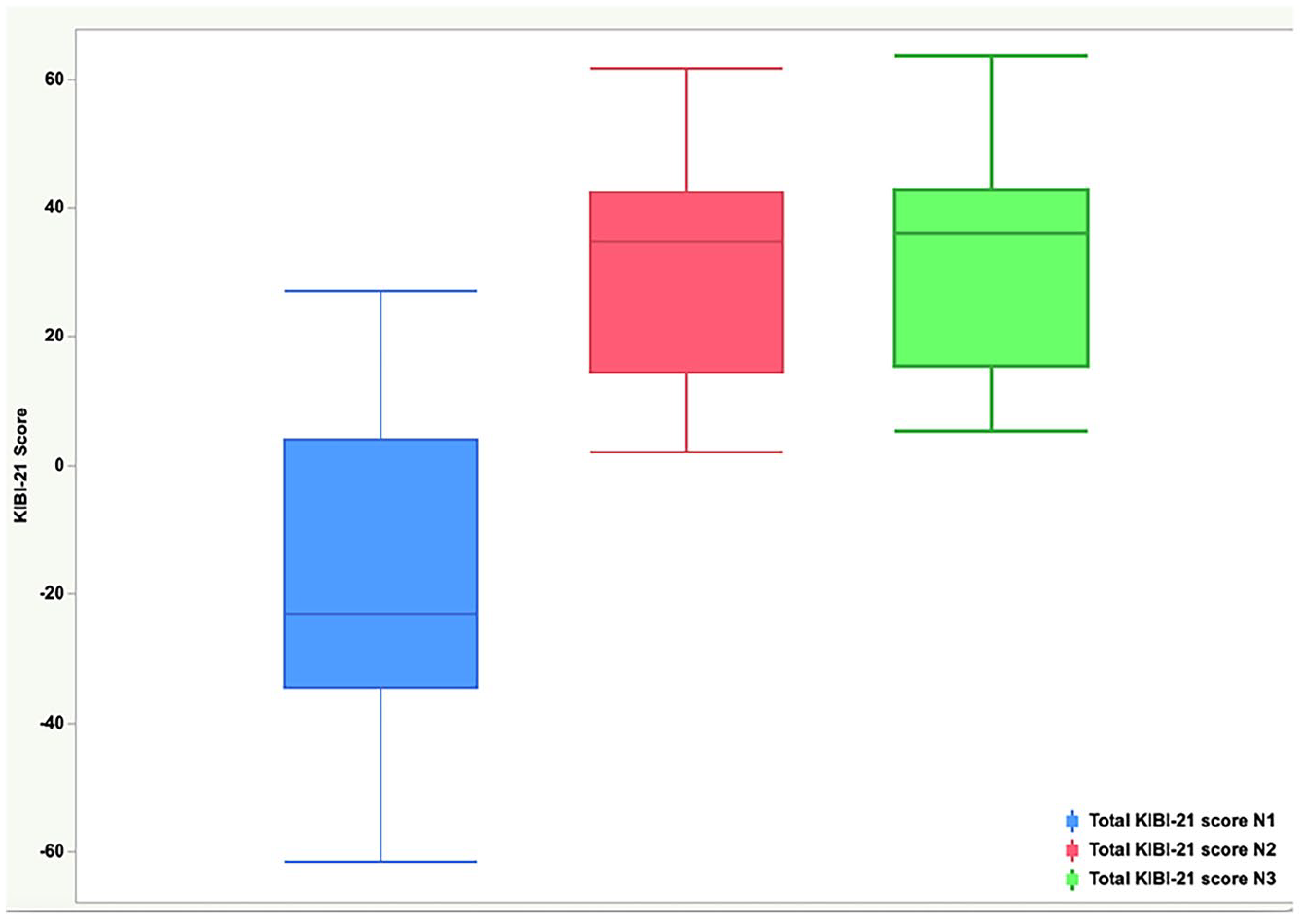
Results of the Keloid Intervention Benefit Inventory-21 at the 3 times of assessment depicted in boxplots. Preoperative data (N1) are shown in blue, results after 6 months (N2) are shown in red, and results after 12 months (N3) are shown in green.
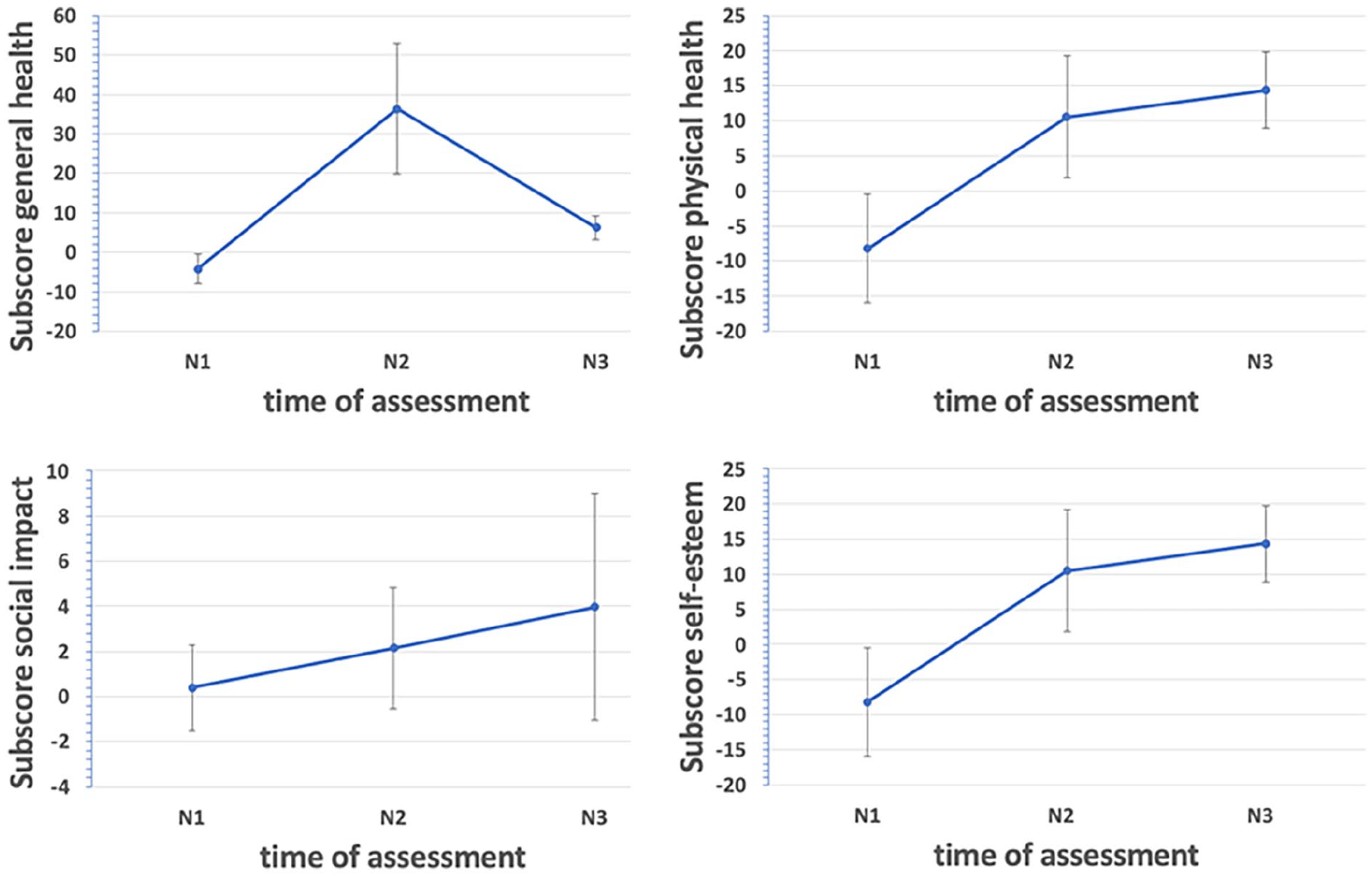
Results of the subscores general health, physical health, social impact, and self-esteem at the 3 times of assessment [preoperative data (N1), results after 6 months (N2), and results after 12 months (N3)].
Discussion
In the field of ENT, various questionnaires for measuring health-related QoL have been developed over the past few decades. Most are designed to assess the QoL of head and neck cancer patients, patients with chronic diseases (eg, chronic tonsillitis and rhinosinusitis), and patients undergoing esthetic surgery.31-37 In chronic diseases, QoL has become the primary therapeutic outcome measure and a marker for assessing therapeutic interventions. Various studies have reported substantial QoL impairment among these patients.17,38 This study assessed the impact of a multimodal therapy for auricular keloids on patients’ QoL. As recurrence is a common problem in keloid formations, it may affect QoL in a chronic disease-like fashion. Moreover, the wide variety of available therapies indicates a lack of standardization in the treatment of keloid formations. This study is the first to assess the impact of each of the 3 components of a well-established therapeutic regimen on patients’ QoL in a prospective design.
Recurrence-free treatment has been shown to effectively improve QoL. 2 A review of outcomes reported by patients with keloids found that multimodal treatments had more positive results. 39 These findings are in line with the long-term results described after administering the multimodal treatment in question for 5 years. 30 This suggests that this regimen, which encompasses local surgical excision, intralesional TAC injections, and the application of a tailored magnetic pressure splint, yields significant improvements in the QoL of auricular keloid patients, as well as low recurrence rates.
The KIBI-21 is a validated tool for assessing QoL throughout the treatment of auricular keloids. 19 To our knowledge, no previous studies have prospectively investigated the QoL of patients with keloids during therapy. In our study, the KIBI-21 scores showed significant improvements in QoL after surgery and intralesional steroid therapy and after pressure splint therapy compared to the preoperative values. Interestingly, QoL improved continuously between the second and third assessments. All subscales also showed significant improvements. Notably, the SE subscale showed significant improvements even between the second and third assessments. Although the GH scores decreased between the second and third assessments, they still showed a significant improvement compared to the preoperative values.
Several limitations of this study should be acknowledged. One limitation was the modest sample size. Another limitation was the single-center nature of this study. Future studies should involve larger and more diverse cohorts and should seek multicenter collaborations to enrich our understanding and management of keloids. 2 Another limitation is that, because the first TAC injection was administered during surgery, the observed QoL improvement at the second measurement could not be specifically attributed to either the surgery or the injection. Although our study does not allow to determine whether a different sequence of therapy components would have shown the same effect on the QoL, we assume that the main effect on the improvement in QoL was due to the improvement in clinical symptoms and the reduction in keloid mass, as in most cases, the resection comes along with the improvement in esthetic appearance in the exposed auricular region. As no other treatment modality was compared in our study, the efficacy of the described multimodal treatment cannot be assessed in our study. Also, the study is not able to define whether the multimodal treatment leads to a higher improvement of QoL compared to other keloid treatment methods. Yet, in a previous retrospective study, it was found that the recurrence of keloids leads to a detectable impairment of QoL even in the long term. 30
Nevertheless, our findings show that the successful management of keloids improves a patient’s QoL throughout the therapeutic process. Walliczek et al reported a higher recurrence rate among patients who did not use a pressure splint. As we did not find a recurrence of keloids in our study over a mean observation period of 29 months, our results may help improve patient adherence to pressure splint therapy, which is particularly important given that these splints are expensive and, in most cases, patients must cover the costs themselves. 2 Indeed, 2 patients in our study did not use a pressure splint due to the high cost involved. Although we found no statistically significant differences in terms of QoL either in the KIBI-21 or in its subscales comparing these 2 patients to the patients with a pressure splint, larger sample sizes for both groups would be needed to evaluate the effect of pressure splint therapy on QoL after 1 year.
In conclusion, the multimodal treatment regimen used in this study can effectively manage auricular keloids, achieving low recurrence rates and improving patients’ QoL. Our study highlights the need for longitudinal evaluations of the effects of keloid treatments on QoL, as relevant data on most published keloid monotherapies and multimodal treatments are lacking. Further studies with larger sample sizes should be conducted to estimate long-term recurrence rates.
Supplemental Material
sj-jpg-1-ear-10.1177_01455613251333673 – Supplemental material for Impact of a Multimodal Treatment of Auricular Keloids on the Patient’s Health-Related Quality of Life: A Prospective Study
Supplemental material, sj-jpg-1-ear-10.1177_01455613251333673 for Impact of a Multimodal Treatment of Auricular Keloids on the Patient’s Health-Related Quality of Life: A Prospective Study by Alexander Helmer, Marcio Cantillo, Lena Zaubitzer, Benedikt Kramer, Nicole Rottery, Haneen Sadick and Daniel Haeussler in Ear, Nose & Throat Journal
Supplemental Material
sj-jpg-2-ear-10.1177_01455613251333673 – Supplemental material for Impact of a Multimodal Treatment of Auricular Keloids on the Patient’s Health-Related Quality of Life: A Prospective Study
Supplemental material, sj-jpg-2-ear-10.1177_01455613251333673 for Impact of a Multimodal Treatment of Auricular Keloids on the Patient’s Health-Related Quality of Life: A Prospective Study by Alexander Helmer, Marcio Cantillo, Lena Zaubitzer, Benedikt Kramer, Nicole Rottery, Haneen Sadick and Daniel Haeussler in Ear, Nose & Throat Journal
Footnotes
Ethical Considerations
Study protocol was reviewed and approved by local Ethics Committee, approval number (2018-645N-MA).
Consent to Participate
Prior to inclusion, each participant (or their parent/legal guardian/next of kin) provided written consent to participate in the study.
Author Contributions
Haneen Sadick, Benedikt Kramer, and Daniel Haeussler were essentially involved in the implementation and conceptualization of the study. Lena Zaubitzer and Daniel Haeussler were responsible for the enrollment of patients and data collection. Alexander Helmer, Marcio Cantillo, and Daniel Haeussler were responsible for data analysis and scientific writing. Nicole Rotter and Haneen Sadick contributed significantly to the success of the study by providing the appropriate human and diagnostic resources and support in data interpretation. Lena Zaubitzer and Haneen Sadick were major contributors to writing the manuscript. All authors read and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this article and its supplementary material files. Further inquiries can be directed to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.