
Abstract
Introduction
Keloids are assigned to pathological scars, which result in a dysregulated wound-healing process after cutaneous injury. 1 They extend beyond the original margins of the scar, and unlike hypertrophic scars, they do not regress spontaneously.2,3 Keloids appear as nodular, firm formations with teleangiectasia and a thin skin envelope. Predilection sites are regions with high skin tension, such as the chest, back, shoulder, or auricular region in the head and neck area.3-5 Although there is no tendency toward malignant transformation, keloids can affect QoL considerably.3,6 The treatment of keloids may be challenging, as recurrence rates are high, and the treatment may imply cosmetic and functional consequences for the patient. Multiple treatment modalities are established, including surgical approaches and conservative treatment methods. Conservative methods include the intralesional injection of steroids, 5-fluorouracil (5-FU), radiation, verapamil, cryotherapy, pressure therapy, or pulsed dye laser (PDL) therapy.7,8 Nowadays, there is no defined standard of care for keloid formations, and the therapeutic approach is often based on the experience of the consultant. 8 The intralesional injection of steroids, especially TAC, is widely established as one of the first-line treatment methods. 9 Especially in comparison to other conservative treatment methods, TAC shows a good response rate of 50%–100% with low adverse side effects.1,8,9 Wong et al. analyzed the efficacy of TAC for keloids and found a significant reduction in keloid size and advantages in comparison to silicone gel sheets, verapamil, and cryotherapy for different keloid aspects, such as vascularity, size, and thickness. 8 Yet, for a monotherapy or adjuvant therapy using TAC injections, a recurrence rate of 33% after one year and 50% after 5 years has been reported by Kill et al. 10 Pressure splint therapy is also a well-established adjuvant therapy for keloid formations that can help decrease recurrence rates. 11 Their efficacy is mainly dependent on the anatomical region. Despite high recurrence rates of 45%–100% in monotherapy, surgical excision of the keloid is essential, especially in patients with large keloids. 11 In the authors’ opinion, intramarginal resection is favorable in comparison to techniques with skin-harvest techniques, as patients suffering from keloids are prone to build out keloids at the donor sites as well. Furthermore, the expanded skin envelope of the keloid can easily be used for tension-free closure of the keloid region. 3 Some data show that the combination of different treatment modalities seems to improve the recurrence rate of auricular keloids.3,12 Coppola et al. 9 and Bao et al. 13 reported reductions in adverse effects and improvements in effectiveness with the combination of 5-FU and TAC in comparison to monotherapy. A systematic review by van Leeuwen et al. 14 investigated the results of radio therapy. They found a recurrence rate of 10%–22% in combination with surgical excision, favoring high-dose-rate (HDR) brachytherapy. This review included long-term follow-up results with a mean period of 49 ± 9.5 months, yet only 30% of the included studies reported recurrence rates. 14 In general, most studies report a follow-up of several months to one year. In an actual study by Berman et al., 15 superficial radiation following surgical excision showed a recurrence rate of 10.4% after one year. Therefore, there is a lack of long-term studies that have investigated recurrence rate after the end of treatment. Moreover, there are no long-term investigations of QoL in patients with auricular keloids. Especially, long-term results for multimodal treatment models are not reported in the literature.
A multimodal therapeutic concept that includes three stages has been established for many years in our department. The aim of this study was to investigate the long-term results of this multimodal treatment method and to evaluate the QoL of patients who had undergone this therapeutic regimen.
Patients and Methods
The study was conducted in the Department of Otorhinolaryngology, Head and Neck Surgery, Division of Facial Plastic and Reconstructive Surgery at our University Hospital. The study protocol was approved and reviewed by the local ethics board of the Medical Faculty (2018-645N-MA). Furthermore, the trial was registered in the German Clinical Trials Register (Register-ID: DRKS00016348).
All patients included in this study suffered from auricular keloid formations. A multimodal treatment approach was used as the therapy regimen. In the first step, the keloid formation was resected with an intramarginal resection using the expanded skin envelope to close the wound without tension. Second, an intralesional injection of TAC 40 mg/mL was given every 4–6 weeks over a period of 6 months, starting intraoperatively at the end of surgery. After 6 months, a customized magnetic pressure splint was fitted to each patient. The patients were advised to apply the splint at least 5 nights per week over a period of 6 months.
In the first step, keloid surgeries carried out in our department between 2009 and 2018 were identified. Patients with a follow-up period of less than 6 months were excluded from further analysis. All identified patients were contacted by phone, mail, or letter and were invited to a clinical assessment of the former keloid region. Written consent was provided, by which the patients agreed to the use and analysis of their data. The former keloid regions were evaluated clinically, and the participants were asked to fill out a questionnaire. QoL was assessed using the Keloid Intervention Benefit Inventory 21 (KIBI-21). This questionnaire is divided into four categories (General Health, Physical Health, Social Impact, and Self-Esteem) and evaluates the four dimensions using a scale ranging from −100 to 100, with positive values indicating an improvement in QoL. This keloid-specific questionnaire was designed to assess QoL before and after a therapeutic intervention. If there was no possibility of contacting the patients, the postoperative follow-up period, the recurrence rate, and the adherence to therapy were evaluated by studying the patients’ files. If the patients’ files did not contain these information, these cases were also excluded from the study. The participants were categorized into two groups related to the recurrency of the keloid formation after application of the multimodal treatment model. All patients without recurrence of the keloid lesion were included in group 1, and patients with keloid formation recurrence were included in group 2.
Statistical analysis was performed with SAS (SAS Institute, USA, Cary, North Carolina, version 9.2) and JMP file (SAS Institute, USA, Cary, North Carolina JMP 15). The Wilcoxon rank-sum test was used to compare the study groups. P-values less than 0.05 were considered significant.
Results
In total, 68 keloids were identified, that underwent the multimodal treatment in our department between 2009 and 2018. Eighteen keloids showed a follow-up period of less than 6 months, and 50 keloids with a mean follow-up period of 59 months and a median of 59 months (range 6–137 months) were enrolled for further analysis. Details are shown in Figure 1. Distribution of patients to the different groups. Mean follow-up given in months (median, range).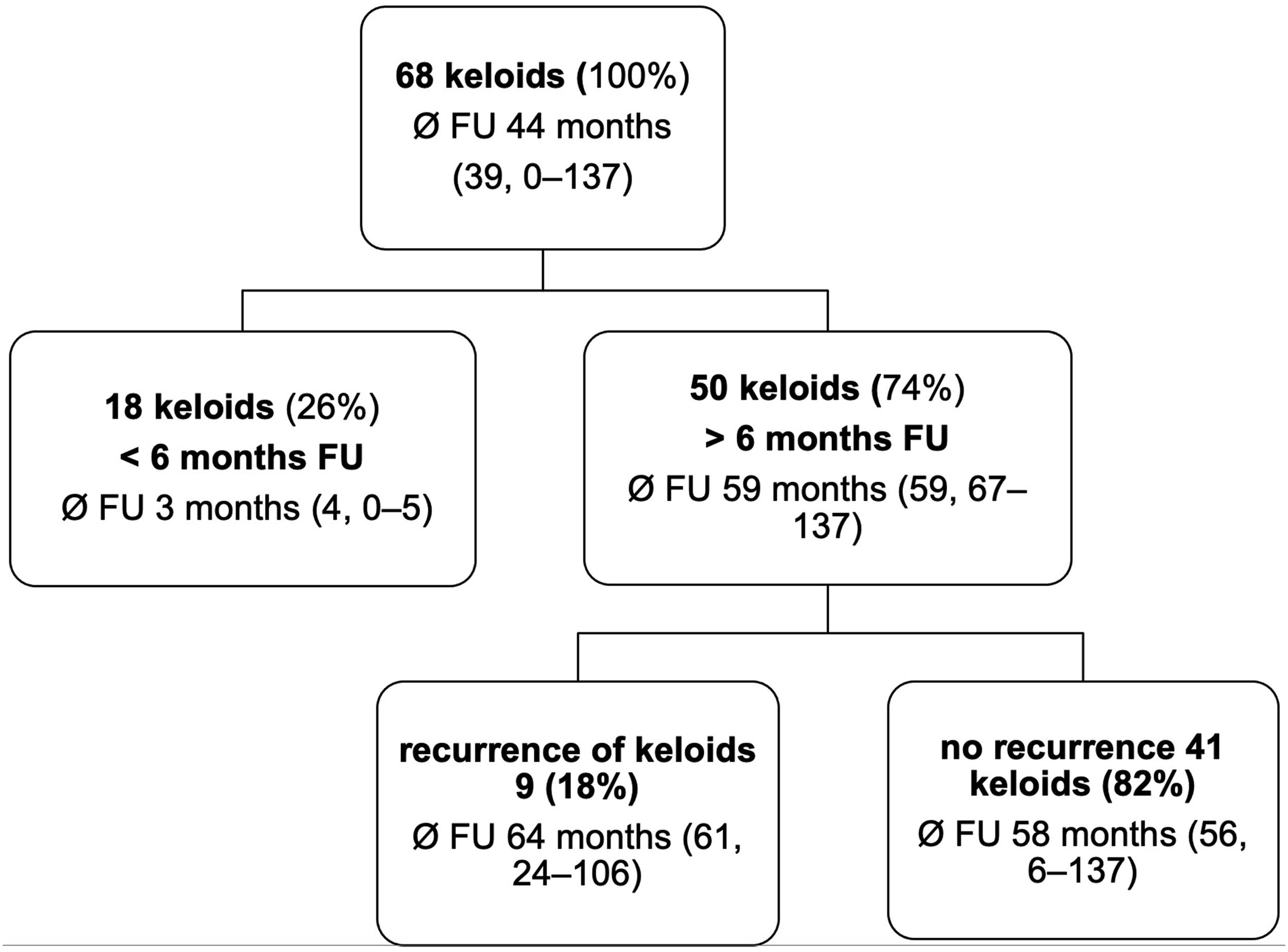
Distribution of Characteristics of the Included and Excluded Cases.

chi-square.
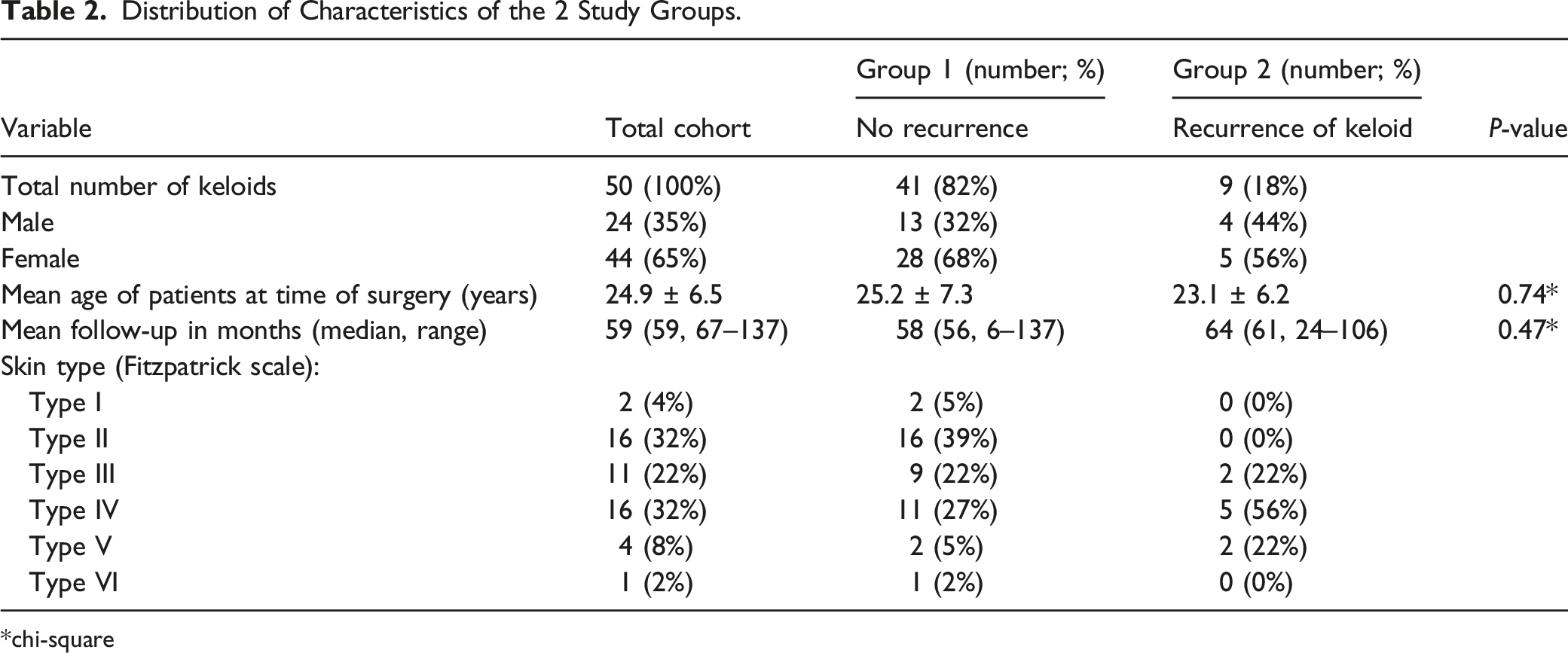
Distribution of Characteristics of the 2 Study Groups.
chi-square
In nine patients (18%), a recurrence of the auricular keloid was observed. There was no statistical difference in terms of intralesional steroid injections or adherence to pressure splint therapy. There was a tendency toward darker skin types observed in group 2, yet without significant differences (P = 0.07). In the analysis of all cases with a recurrent keloid formation, there was one patient with only one steroid injection, and the pressure splint was not worn by the patient. In four cases, the keloid expanded into the retroauricular or infralobular region. All recurrent keloids were treated with a series of intralesional TAC injections. No further surgical approach was needed, as all keloids could be controlled with the intralesional injections.
Quality of Life—The Keloid Intervention Benefit Inventory 21 (KIBI-21)
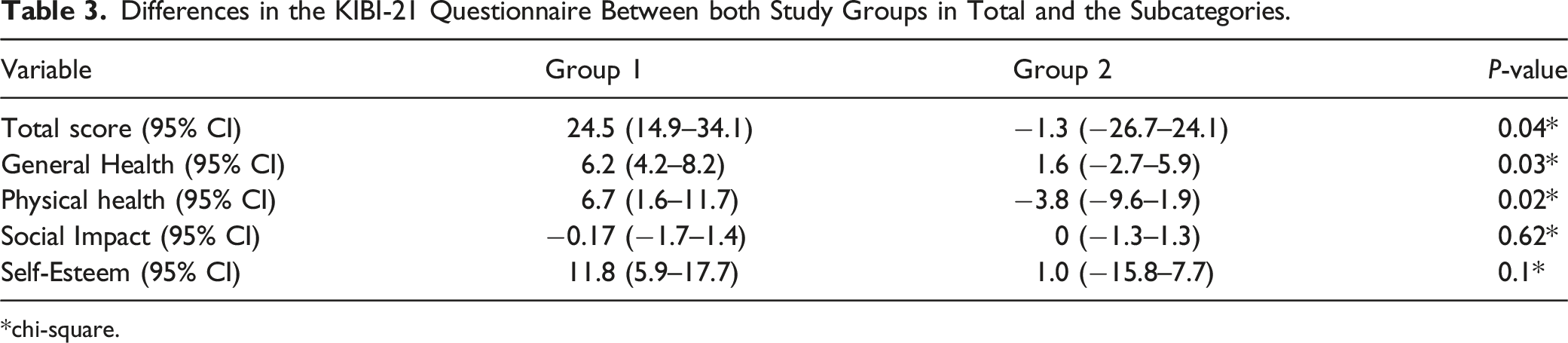
Differences in the KIBI-21 Questionnaire Between both Study Groups in Total and the Subcategories.
chi-square.
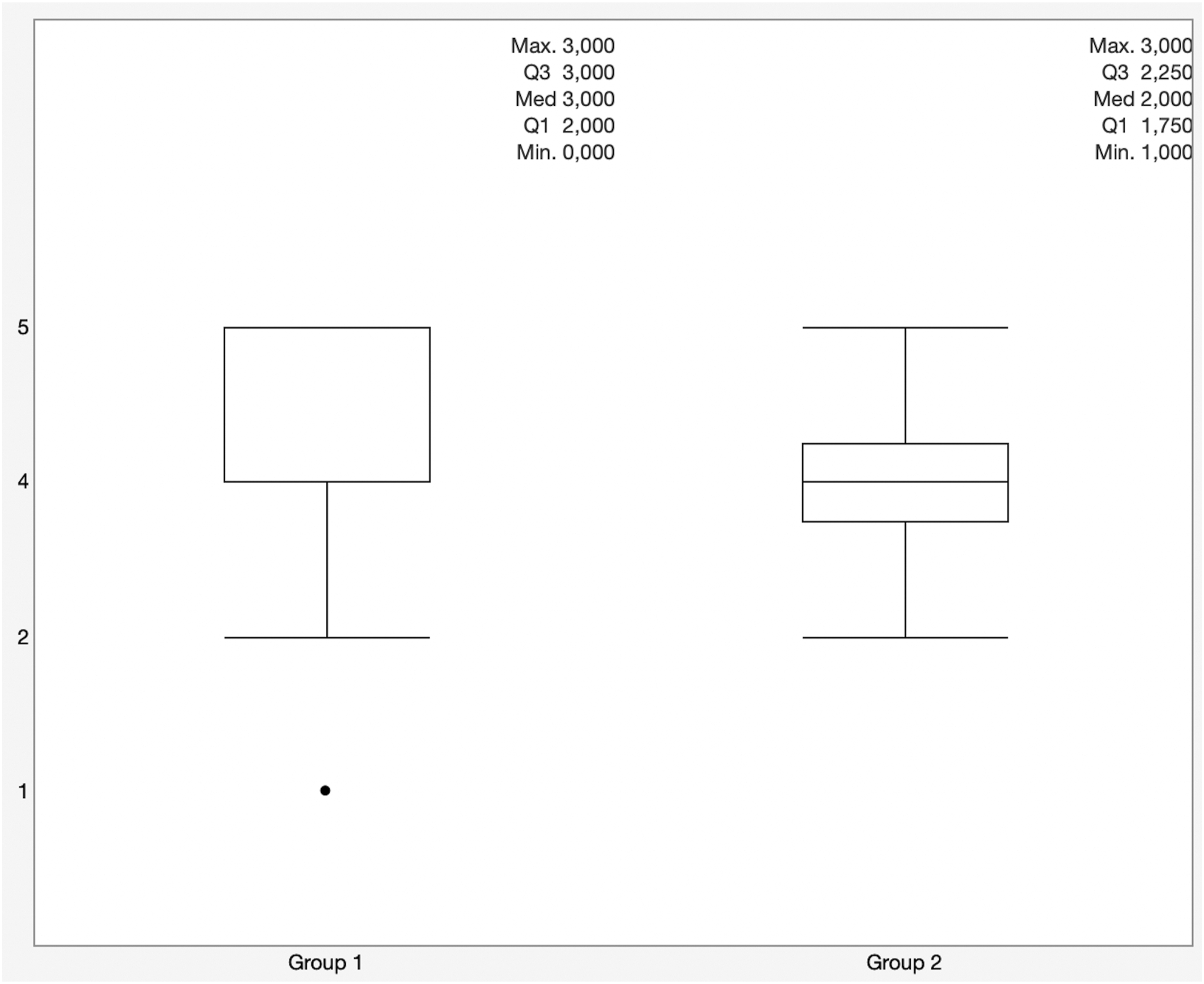
Satisfaction with multimodal treatment algorithm in comparison between both study groups.
Discussion
Keloid formations in the head and neck area may have a negative impact on QoL. Because of their exposed localization, they can lead to stigmatization, and depending on individual lifestyle, they can also impair patients’ leisure activities. As keloids tend to recur, the can impact patients’ QoL in a chronic disease-like fashion. 16 Therefore, the importance of QoL improvement has been raising consistently in these patients over the last decades.17,18 In other chronic diseases, QoL has become the primary therapeutic outcome goal. To improve QoL, especially functional and esthetic aspects must be considered individually. The diversity of available treatment methods, the lack of standardization for auricular keloids, and the individual expectations of each patient are the reasons why the treatment of keloids is still challenging.
The intralesional application of TAC is, aside from surgical resection, one of the most widely accepted therapies of choice.7,8,13,19 It can be applied either as a first-line therapy or an adjuvant therapy after surgical resection, and it has been shown to improve the recurrence rate. 9 The combination of different treatment modalities has been shown to improve recurrence rates and patient satisfaction.3,9,14 A couple of studies have investigated the combination of two different treatment modalities.8,9,13,14 The best results in terms of recurrence rates have been found following surgical resection and radiotherapy (10%–22%) and surgical resection followed by TAC injections (8%–50%).9,11,14 For multimodal treatment methods, Walliczek et al. 3 and Hao et al. 20 described recurrence rates of 8% and 12.8%, respectively. Both studies used surgical resection, TAC injections, and, subsequently, the application of pressure splints. The studies evaluated the recurrence rate after mean follow-up periods of 30 months and 12 months. For the first time, our study presents long-term follow-up data for a multimodal treatment regimen for auricular keloids. With a recurrence rate of 18% over a mean period of 5 years, this multimodal treatment regimen shows good results in comparison to monotherapies and other combination therapies. The assessment of QoL shows good results for patients without keloid recurrence. In our study, there was no difference in QoL concerning the subcategories SI and SE. This may be because time had passed between the end of treatment and the time of data collection, which may have influenced the participants’ perception of SI and SE. Furthermore, even if patients had suffered from a recurrence of their keloid, they had already undergone further treatment by TAC injections at the time of data collection. Therefore, these patients may not have experienced impairment of the SI and SE. Interestingly, we still found significant differences in the categories GH and PH. Even if the keloids recurred, they could be controlled by TAC injections and pressure splint application. This may be why participants with keloid recurrence still experience a negative impact on their QoL, as the aesthetic result may be impaired if a recurrence of the keloid occurred. Yet, satisfaction with the therapy was high in both groups. In four cases, the pressure splint could not be fitted sufficiently to the complete wound ground because of the localization. We hypothesize that the location of the keloid especially may impact the probability of recurrence, as the keloid recurred in the area that was not covered by the pressure splint.
Different limitations apply to our study. First, as all patients had already undergone therapy, a retrospective collection of data was necessary. In total, 26% of the keloids had to be excluded from further analysis, as they were lost to follow-up, less than 6 months had passed after therapy at the time of data collection, or the needed information was not accessible. Yet, both study groups show long-term follow-up periods with means of 64 months and 58 months. In group two, there was an even longer follow-up period, so recurrence of the keloid after the secondary treatment can be excluded. Second, in five cases, the keloid recurred between 2 and 6 months after treatment. In four cases, the exact recurrence-free period was determined from the patients’ memories. This means it is not possible to differentiate between recurrence and possible residual tumor mass after the end of treatment. In this case, recurrence may be prevented by an early continuation of TAC injections and pressure splint therapy. Third, the QoL was assessed at one moment of follow-up after every patient had undergone sufficient therapy and control of the keloid formation. Therefore, it is not possible to attribute the effect of each treatment modality to the QoL or its subcategories. Furthermore, the time that passed between the last intervention or recurrence of the keloid may influence the evaluation of QoL of each patient. Still, as the negative impact of keloids on the QoL has been well documented in the literature, the improvement of QoL in the long-term by the described multimodal treatment may be an important parameter for clinical therapists in the evaluation of treatment strategies. Our results show that this positive impact on the QoL may be detectable even over a long-term period. The fact that we did not find significant differences in the categories SI and SE may be explainable as all keloids could be controlled at the time of assessment. Even in a case of recurrence, these keloids were controlled by TAC injections and pressure splint therapy. Therefore, the categories SI and SE may no longer be affected at the time of assessment. In our opinion it seems plausible that GH and PH may still show impairment in patients suffering from recurrence as these categories contain questions about their daily discomforts such as itching, pain, problems wearing headgear or their personal evaluation of an optimistic view of the future. Yet, further prospective studies are needed to evaluate the effect of each treatment modality on the QoL and to prove a causal connection between the multimodal treatment and the impact on the subcategories of the QoL questionnaire.
Conclusions
As especially young and female patients are more likely to be affected by keloids, radiation therapy should not be considered a therapy of choice in the authors’ opinion, even if it shows good clinical results in terms of recurrence rates. Therefore, the presented treatment regimen can be considered a good option in patients suffering from auricular keloids, as the recurrence rate is comparable to the best outcome rates reported in the literature. This method improves QoL in patients with auricular keloids. Our data suggest that the localization of the keloid and the possibility of an adequate adjustment of pressure splint therapy influence the recurrence rate in a relevant fashion. Further prospective controlled studies are needed to investigate this relationship further.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was approved and reviewed by the local ethics board of the Ethical board II of the University of Heidelberg, Medical Faculty of Mannheim (2018-645N-MA).
Informed Consent
Written informed consent was obtained from all individuals enrolled in the study for their anonymized information to be published in this article.
Statement of Human Rights
All methods were carried out in accordance with the Declaration of Helsinki and were approved by the local ethics board of the Ethical board II of the University of Heidelberg, Medical Faculty of Mannheim (2018-645N-MA).