
Abstract
Purpose:
This study aimed to contribute to the literature by sharing experience of head-neck extramedullary plasmacytoma (EMP), which are rarely seen.
Methods:
A total of 11 patients treated for head and neck region EMP between 2000 and 2023 were screened retrospectively.
Results:
The 11 patients comprised 9 men and 2 women with a mean age of 55.1 ± 16.2 (range, 16-74) years. The most affected regions were seen to be the sinonasal tract, larynx, and tonsils. In the histopathological examination, plasma cells had a mature or anaplastic appearance, and one of the kappa and lambda light chains was positive and the other was completely negative. The serum electrophoresis and bone marrow flow cytometry results were negative. Of the patients with confirmed EMP diagnosis, 8 were treated with radiotherapy (RT) alone, 1 patient with maxillectomy, and 1 patient endoscopic sinus surgery followed by RT. RT was applied at a dose of 44 to 50 Gy for 22 to 25 sessions. In 1 patient, RT and chemotherapy were applied together.
Conclusion:
In cases presenting with a submucosal, destructive tumor in the head and neck region, especially in the sinonasal region, EMP should be kept in mind. When histopathological results are confirmed, a differential diagnosis from multiple myeloma (MM) is required. Flow cytometry is of guidance in the differentiation of EMP from extranodal lymphoma. However, it should be noted that the effect of RT may be less in EMPs originating from the paranasal sinus compared with other anatomic regions, and surgery may be required before or after RT. A radiation dose of 45 Gy is sufficient for local control. Patients require long-term follow-up, as there is a possibility of EMP transforming to MM.
Introduction
Extramedullary plasmacytoma (EMP) is a monoclonal hematopoietic neoplasm of B-cell origin that develops outside of the bone marrow. The incidence of EMP is 0.02/100,000 person-years. 1 EMP accounts for 3% of all plasma cell neoplasms, and 85% of EMP occurs in the head and neck region. 2 EMP is more common in males than in females. This neoplasm often manifests itself as a solid submucosal grey-colored mass in the upper respiratory tract and is often seen in the nasopharynx, nasal cavity, and sinuses.3,4 Although there are variations according to the region involved, symptoms are mostly nasal obstruction in the sinonasal region and hoarseness in the laryngeal region. Although they are locally-aggressive tumors, 10% to 20% metastasize to the neck. 4 Biopsy is required for diagnosis after tumor evaluation with cross-sectional imaging. When histopathological results are confirmed, a differential diagnosis including multiple myeloma (MM) is required because a tumor in the head and neck region can be a late symptom of MM. 3 The risk of converting EMP to MM varies between 8% and 31%.2,5 Primary EMP has a better prognosis than plasmacytoma developing secondary to MM, so the differential diagnosis is important. 6 The differentiation of EMP from MM is based on the following criteria: (i) the presence of 1 or more extramedullar plasma cells tumor, (ii) normal plasma cell ratio and normal plasma cell morphology within the bone marrow or <10% normal plasma cells in the bone marrow, (iii) no radiological osteolytic lesion, (iv) no hypercalcemia or kidney failure, and (v) the absence of or low serum concentration of M-protein. The same criteria are valid for tumor recurrence.7,8
In these types of radiosensitive masses, the treatment options include radiotherapy (RT)/chemoradiotherapy or surgery (for resectable tumors). In 65% of patients, full recovery is achieved after treatment and the disease does not progress to MM. 9
The aim of this study was to contribute to the literature by sharing our experience of head-neck EMP.
Materials and Methods
The study was approved by the Clinical Research Ethics Committee (decision no. 2023/720). In a retrospective screening of patient records for the years 2000 to 2023, 11 patients were identified who had been treated for head and neck region EMP, and were enrolled in the study. Following the histological diagnosis of EMP, the diagnosis was confirmed by the demonstration of monoclonal immunoglobulins in immunohistochemical analysis. Then, patients diagnosed with plasmacytoma underwent tests for full blood count, serum calcium level, kidney function, serum protein electrophoresis, flow cytometry from bone marrow biopsy, and bone scanning/positron emission tomography (PET) -computed tomography (CT) imaging. The 11 patients were evaluated in respect of age, gender, symptoms and findings on presentation, pathological results, form of treatment, and prognosis after treatment.
Results
The study included a total of 11 patients comprising 9 males and 2 females with a mean age of 55.1 ± 16.2 years (range, 16-74 years).
The regions of the head and neck affected by EMP differed among the patients (Table 1).
Regions of Involvement and Treatment Methods.
Abbreviations: CT, chemotherapy; RT, radiotherapy; S, surgery.
The most commonly-presenting symptom was nasal obstruction, followed by dysphagia, stridor, hemoptysis, and hearing loss.
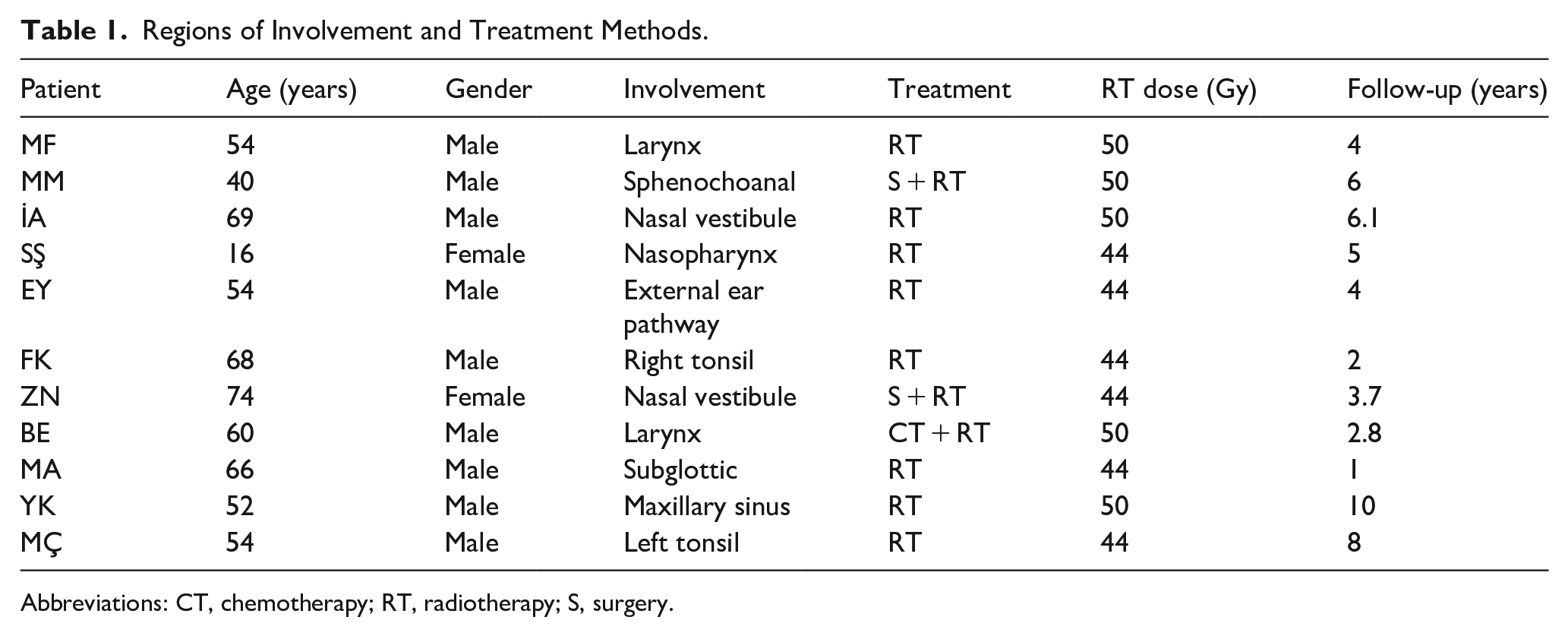
On examination, a submucosal mass with a smooth surface in all the patients was observed (Figure 1).
(a) A 60-year-old male with a submucosal mass in the left aryepiglottic fold (thick arrow: mass, thin arrow: right arytenoid). (b) A 74-year-old female patient with a smooth-surfaced mass filling the right nasal vestibule and passage (thick arrow: mass, thin arrow: right nasal vestibule). (c) A 40-year-old male patient with a smooth-surfaced mass with right sphenochoanal localization (thick arrow: mass, thin arrow: right middle turbinate).
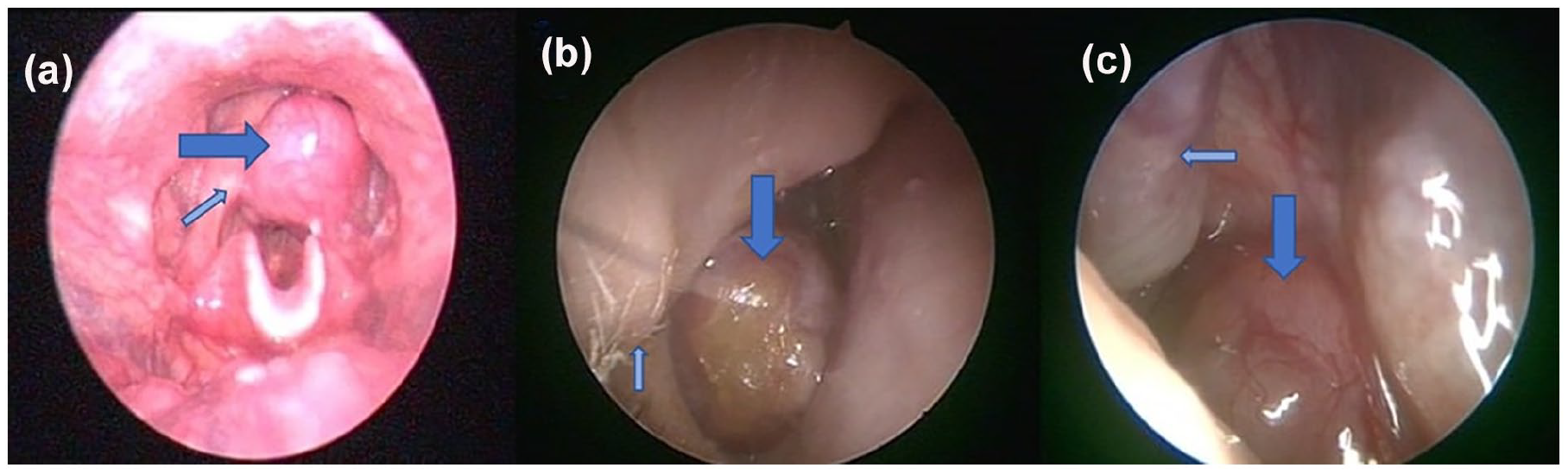
Radiological imaging was performed before the diagnostic biopsy. In some patients, CT or magnetic resonance imaging (MRI) was preferred, and both imaging methods were performed in some others. The most common imaging finding was a lobulated/irregular contoured mass with homogenous/diffuse contrast, causing bone destruction (Figure 2). Before treatment, the mass dimensions were 20 to 45 mm.
(a)MRI T2 fat-suppressed image showing hyperintense appearance in the left aryepiglottic fold in a 60-year-old male patient. (b) A 66-year-old male patient with soft tissue in the subglottic area on CT. (c) A 74-year-old female patient with soft tissue in the right nasal vestibule with hypointense appearance on T1 MRI. (d, e) A 69-year-old male patient with soft tissue in the right nasal passage showing intense contrast enhancement on T1 and on T2 fat-suppressed images on MRI. (f) A 52-year-old male patient with left maxillary sinus involvement on PET/CT. CT, computed tomography; MRI, magnetic resonance imaging; PET, positron emission tomography.
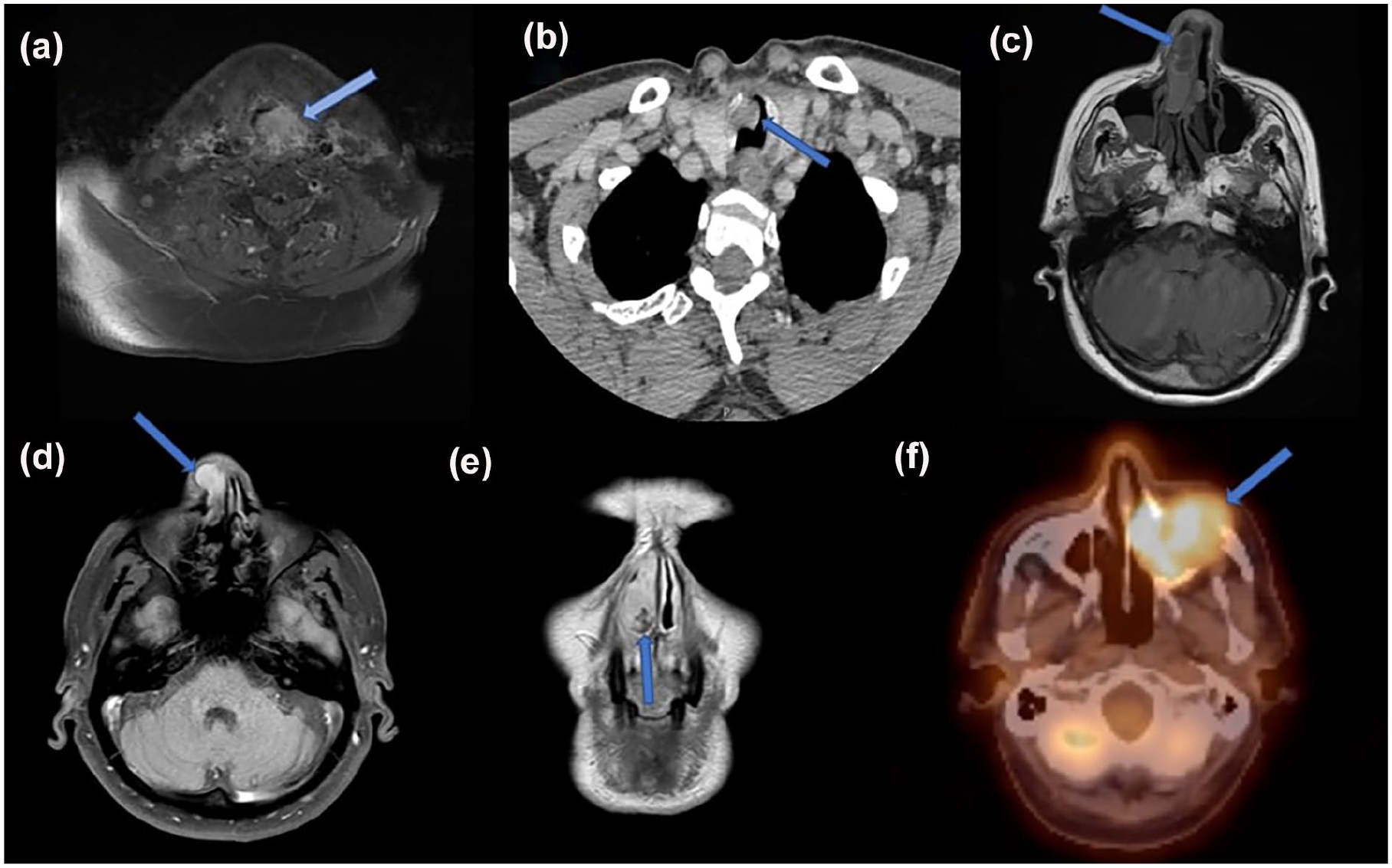
The sampling in all patients was performed with a punch biopsy. Histological analysis of hematoxylin-eosin (H&E)-stained sections of plasmacytoma showed infiltration of uniform round diffuse plasma cells with ordinary or, in some cases, with anaplastic morphology, which is a prominent nucleolus or a blastic nucleus and abundant eccentric cytoplasm. Plasma cells were positive for Vs38c, CD138, Mum-1, CD56, and CD117, and negative for CD20, CD19, and CD45. The plasma cells had a mature or anaplastic appearance, and one of the light chains of kappa and lambda was positive and the other was completely negative (Figure 3).
A 66-year-old male patient with subglottic solitary plasmacytoma. (a) All plasma cell infiltration in anaplastic morphology (×400 H&E; yellow arrow). (b) Widespread positivity seen in neoplastic cells with CD38 (×200, immunoperoxidase). (c) Kappa positive (×200, immunoperoxidase). (d) Lambda negative (×200, immunoperoxidase).
On PET/CT scans obtained after the histopathological diagnosis, metastasis was negative, and on the blood tests no anemia, hypercalcemia or kidney dysfunction was determined.
There was no evidence of an increase in serum immunoglobulin in the serum electrophoresis performed (Figure 4).
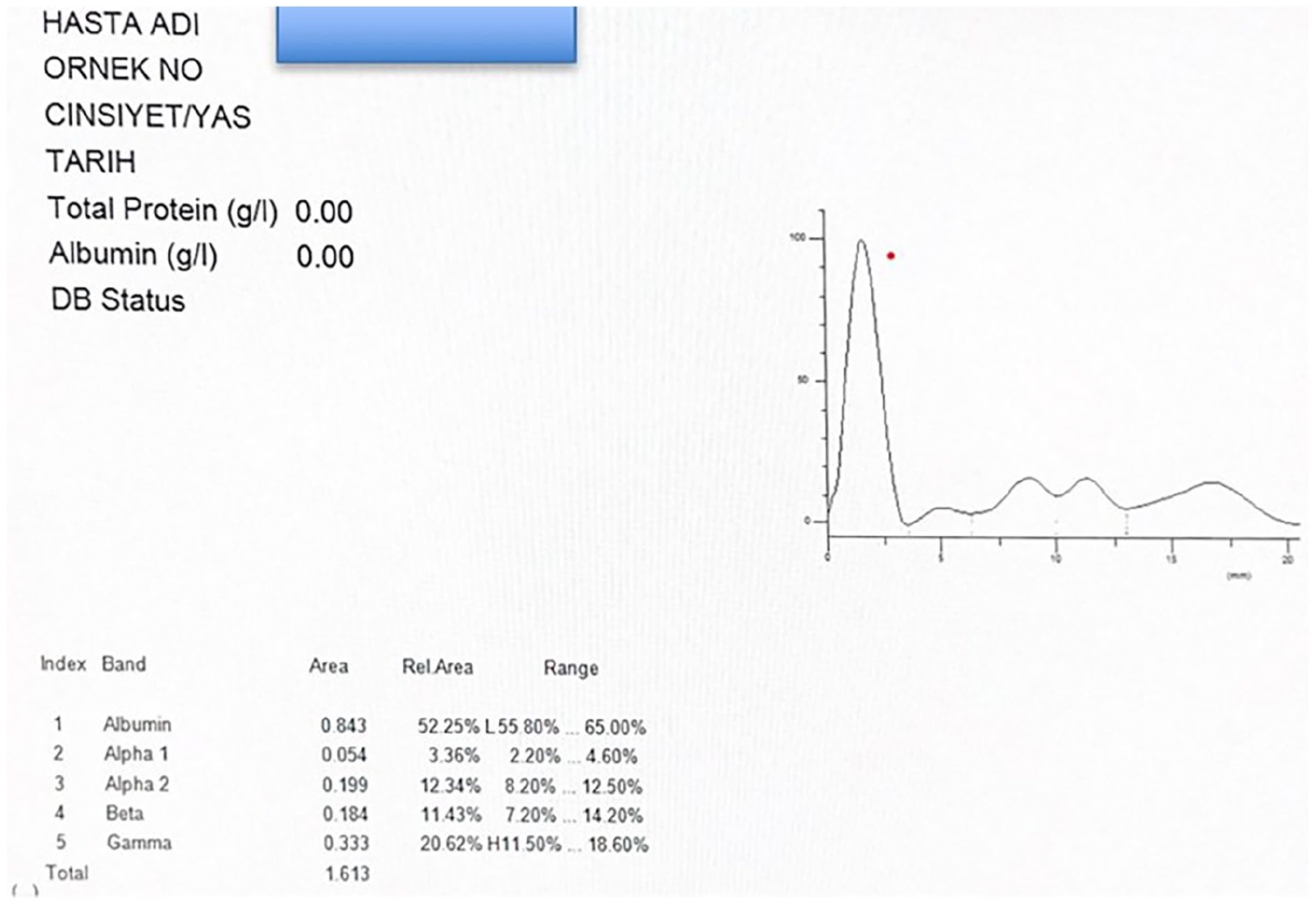
Absence of M spike shown on serum protein electrophoresis test in a 40-year-old male patient.
In flow cytometry performed on bone marrow aspirate, <5% plasma cells were present, there was no monoclonality, and in all 11 patients, the flow cytometry result was evaluated as normal (Figure 5).
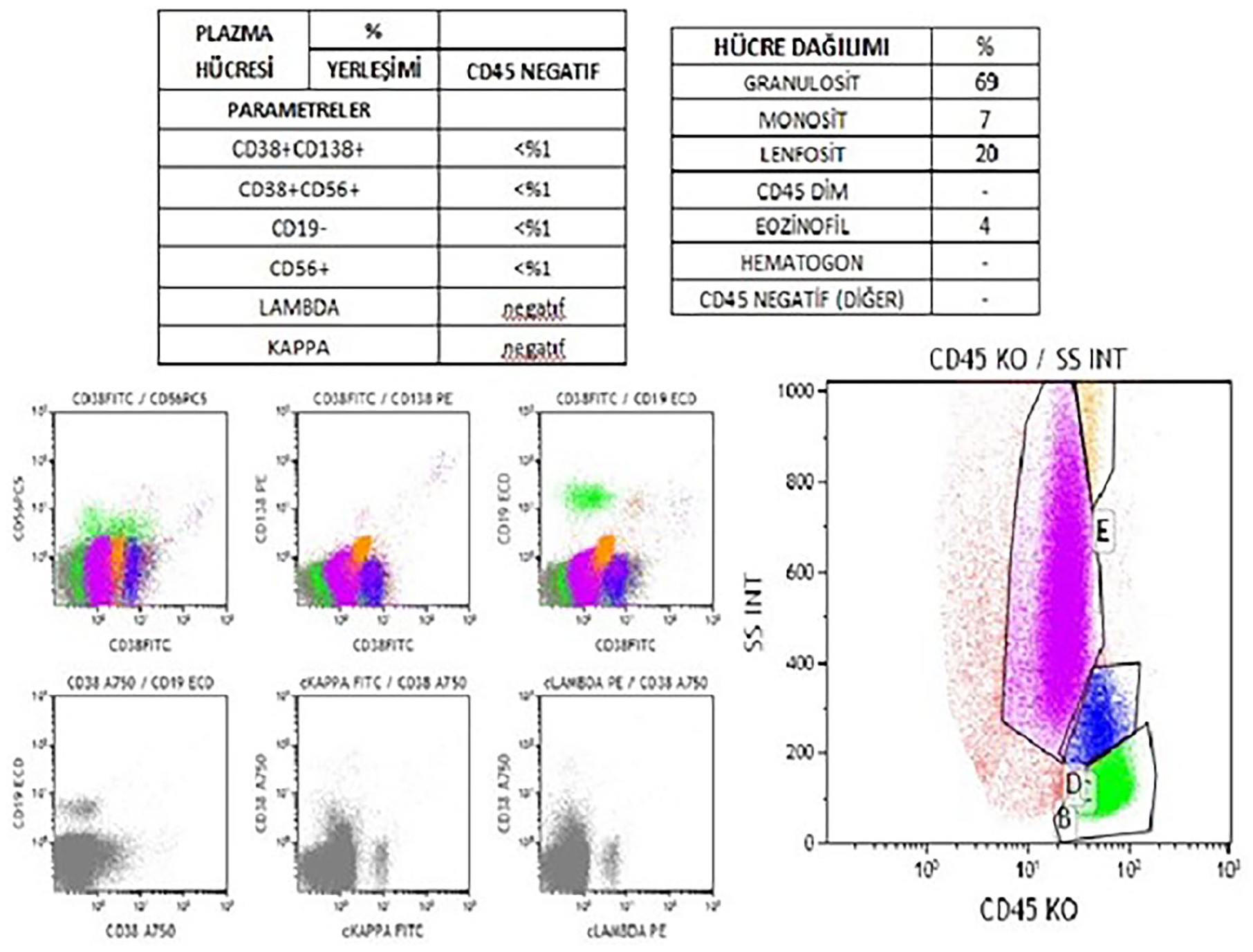
74-year-old female; flow cytometry result. In total, <0.1% of plasma cells without CD38 and CD138 expression were observed.
Eight of the 11 patients with confirmed diagnosis of EMP were treated with RT alone. RT was applied after maxillectomy in 1 patient with a 45 mm mass causing destruction in the nasal bones, after endoscopic sinus surgery in 1 patient, and CT and RT were applied together in 1 patient. RT was applied at a dose of 44 to 50 Gy for a total of 22 to 25 sessions. The mean follow-up period in the current series was 4.7 years (range, 1-10 years), and the survival rate was 63.6%. There was no recurrence or MM transformation in any patient. Four patients died during the follow-up period, but the causes of death could not be found in the records.
Discussion
Head and neck EMP is a rarely-seen malignant plasma cell tumor. EMP is more common in men 10 and is usually seen in the fourth to seventh decade of life. The findings of this study showed a predominance of male patients and the mean age at the time of diagnosis was 55.1 years, consistent with the literature. However, the youngest patient was 16 years old, showing that the disease can also develop at a young age.
EMP mostly involves the sinonasal region,1,2 but can also involve the larynx, oral cavity, oropharynx, hypopharynx, thyroid gland, salivary glands, and lymph nodes. 11 In this case series, there was heterogenous region involvement.
High-resolution contrast CT and MRI provide information on differential diagnosis, involvement of surrounding structures, and disease spread. Typical features on MRI are hypointense T1, hyperintense T2, infiltrative, and significant contrast enhancement giving multiple flow-space signals without necrosis after contrast administration.12,13 Destruction of surrounding bone tissue is generally seen on CT. 14 The imaging findings of the cases in this series are compatible with those in the literature.12-14
EMPs are formed from plasma cells that express CD138, CD38, and cytoplasmic light chains of kappa or lambda type. 15 The most important finding showing that the plasma cells were neoplastic was that one of the kappa and lambda light chains was positive and the other completely negative. Negative staining for CD45, CD19, and CD20, and positive staining for CD56 and CD79 can support this diagnosis.15,16 However, in some patients, even if morphology and immunohistochemistry are compatible with plasma cell neoplasia, a differential diagnosis of extranodal B-cell lymphoma may be necessary. Flow cytometry performed from an aspirate sample can be used for differentiation in these patients. Previous studies have also reported that by determining patients with minimal occult bone marrow disease, flow cytometry can show the risk of disease progression. 17
RT is accepted as the primary treatment for EMP due to the radiation sensitivity of plasma cell tumors. Some authors have stated that local control is obtained with a dose of 30 to 35 Gy for 3 weeks, while others have recommended a longer duration and a higher dose of RT (>45 Gy), especially in sinonasal involvement.5,18-21 Another study reported that the administration of at least 45 Gy RT is necessary in head and neck EMP. 22 In the current study, RT was administered at doses of 44 to 50 Gy. Factors associated with poor prognosis during RT include young age, the presence of bone destruction, large primary tumor (>5 cm), the recurrence of tumors, and tumors located in the sphenoid sinus, maxillary sinus, orbit, and pharynx.18,23 In a study by Tsang et al, local control could not be achieved with RT in 3 of 5 patients with tumors originating from the paranasal sinuses. 18 Surgery is another treatment option for those with resectable disease. 10 A 10-year-old girl with EMP of the maxillary sinus was reported to have been treated with excision of the mass and postoperative RT for recurrence. 23 In the patient of the current series who underwent maxillectomy, the mass, 45 mm in size, had caused destruction in the nasal bones. Another patient who underwent sinus surgery had a sphneochoanal mass. These 2 patients with paranasal sinus involvement were treated with postoperative RT, and no recurrence occurred. If the mass cannot be completely excised or if regional lymph nodes are involved, treatment of RT is recommended together with surgery. 24 There are studies in literature showing that the recurrence-free survival rate is higher in combined treatment (surgery + RT) than for a single treatment modality.2,20 However, there is also a study reporting that patients have not benefitted from combined treatment. 25 The United Kingdom Myeloma Forum recommends adjuvant CT for EMPs that are >5 cm in size, recurrent, refractory, and high-grade, and for MM. 26
In the literature, it has been reported that 61.1% of patients diagnosed with EMP do not experience recurrence or systemic involvement, and local recurrence develops in 22%. 24 In other reports, local recurrences developed in 19% of patients. 2 When comparing patients treated with primary radiation dose <35 Gy with those treated with >35 Gy, the number of recurrences has not been found to be statistically significant. 2 The current series patients were treated with radiation dose 44 to 50 Gy, and no recurrence or MM transformation developed. Tournier-Rangeard et al reported improved local control when the radiation dose was ≥45 Gy. 5 The current study results support the knowledge that a radiation dose of 45 Gy is sufficient for local control.
EMP has the best prognosis among plasma cell tumors, and the 5 year disease-free survival rate varies between 31% and 81%. 5 The occurrence rate of MM at 5 and 10 years was reported to be 23% and 28%, respectively. 2 In the same study, the average time to the development of MM from the date of diagnosis of EMP was 2.8 years, with a range of 4.5 months to 8.6 years. 2 Eriksen et al reported that the risk of transformation to MM increases in the first 2 to 3 years after diagnosis. 1 The mean follow-up period in the current series was 4.7 years (range, 1-10 years), and the survival rate was 63.6%. It has also been emphasized that head and neck EMPs have a better prognosis than EMPs in other regions. 10 Old age, which is considered a poor prognostic factor, is thought to be responsible for the wide survival range. 11
Conclusion
In cases presenting with a submucosal, destructive tumor in the head and neck region, especially in the sinonasal region, EMP should be considered. When histopathological results are confirmed, a differential diagnosis from MM is required. Flow cytometry is of guidance in the differentiation of EMP from extranodal lymphoma. However, it should be noted that the effect of RT may be less in EMPs originating from the paranasal sinus compared with other anatomic regions, and surgery may be required before or after RT. A radiation dose of 45 Gy is sufficient for local control. Patients require long-term follow-up, as there is a possibility of EMP transforming to MM.
Footnotes
Acknowledgements
The authors thank Prof Dr Mustafa Yavuz Köker who gave permission for the use of the flow cytometry data.
Author Note
Nezaket Tektaş who is the corresponding author has moved to a new institution from Erciyes University since completing the research, so the current address information was used as the contact address.