
Abstract
The aim is to analyze the clinical outcomes of patients with extramedullary plasmacytoma (EMP) and review the characteristics of this disease. We retrospectively reviewed the clinical data of a cohort of 22 patients diagnosed with EMP between 1983 and 2017. Baseline characteristics and progression data were collected to calculate the incidence of progression to multiple myeloma (MM) and to analyze survival rates and outcomes. Previous major cohort studies were reviewed and compared with this study. Extramedullary plasmacytomas were located in the head and neck in 17 (77%) of the 22 patients. The median time between onset and diagnosis was 7 months, and the median age at diagnosis was 52.5 years (range 15-72 years). Extramedullary plasmacytoma occurred more frequently in men with an approximate ratio of 2.1:1. The majority of patients underwent surgery (13/22, 59.1%) and half received radiation (11/22, 50%). A small proportion of patients received chemotherapy (2/22, 9.1%). There was a median follow-up time of 98.5 months. The 5-year overall survival, progression-free survival, and MM-free survival rates were 84.2%, 67.3% and 75.9%, respectively. Complete resection without major functional damage is a promising option that can favorably improve prognosis in patients with resectable disease. Patients with regional lymph node metastasis or positive immunoelectrophoresis results require more aggressive treatment and may have poorer prognosis.
Introduction
Solitary plasmacytoma (SP) is a rare plasma cell tumor that does not involve bone marrow. 1,2 The disease represents less than 5% of all plasma cell dyscrasias. Extramedullary plasmacytoma (EMP) makes up a third of all SPs 3 and is rarer. Extramedullary plasmacytoma localizes to soft tissues and can develop in any part of the body but occurs most frequently in the head and neck regions. Approximately 80% to 90% of EMPs arise in the upper respiratory and digestive tracts. 2,4,5 Patients usually present with localized submucosal masses and accompanying symptoms related to compression and obstruction of local structures between the fifth and seventh decades of life. For this study, we retrospectively analyzed the clinical findings of diagnosed EMP patients seen at Peking Union Medical College Hospital (PUMCH) between January 1983 and December 2017 and conducted a review of the disease literature.
Patients and Methods
Twenty-two patients at PUMCH were treated for EMP between January 1983 and December 2017. Primary site masses were biopsied or underwent fine-needle aspiration. Extramedullary plasmacytoma was diagnosed histologically based on hematoxylin–eosin and Giemsa-stained slides. Diagnosis was confirmed by immunohistochemical (IHC) demonstration of monoclonal cytoplasmic immunoglobulins. Monoclonal disease was confirmed by IHC of pathologic samples and/or immunoelectrophoresis (IEP) of serum or urine. The histologic samples were independently assessed by 2 pathologists blinded to patient clinical status. Patients underwent bone scans or, after 2008, positron emission tomography–computed tomography to exclude multiple myeloma (MM). All patients underwent bone marrow aspiration, routine blood counts, blood chemistry, and urinalyses.
Diagnostic criteria 6 for EMP was as follows: (1) biopsied tissue samples showing plasma cell histology; (2) presence of monoclonal disease, as shown by IHC of pathology samples and/or IEP of blood or urine; (3) bone marrow plasma cell infiltration not exceeding 10% of all nucleated cells; (4) absence of osteolytic bone lesions; and (5) absence of anemia, hypercalcemia, or renal insufficiency. Imaging was repeated on all patients after treatment. Patients with IEP-positive results repeated IEP of serum and urine after treatment.
Patients were followed until April 2020, with a median follow-up duration of 98.5 months (range, 21-244 months). Survival rates were determined using the Kaplan Meier method. All statistical analyses were performed using SPSS software (SPSS for Windows version 26.0; SPSS).
Literature Search
The PubMed database was searched using the terms “plasmacytoma” and “extramedullary plasmacytoma” for papers published in English through April 2020. More than 1000 published articles were identified. All studies with more than 20 patients with EMP were reviewed. 2,4,5,7 -28 Of these, studies lacking adequate clinical data were excluded.
Results
Clinical Manifestations
The PUMCH database search identified 22 patients diagnosed with and treated for EMP between 1983 and 2017. These 22 patients included 15 (68%) men and 7 (32%) women with median age of 52.5 (range, 15-72 years) years. Extramedullary plasmacytomas were present in the head and neck regions of 17 (77%) patients. Five patients had one of the EMPs in kidney, anterior chest wall, superior mediastinum, colon, and testis (Table 1). The sinonasal cavity is the most commonly involved site in the head and neck area (7 cases, 32%). The mean time between the appearance of symptoms and diagnosis was 7 months (range 1-24 months).
Demographic and Clinical Characteristics of the 22 Patients With EMP.
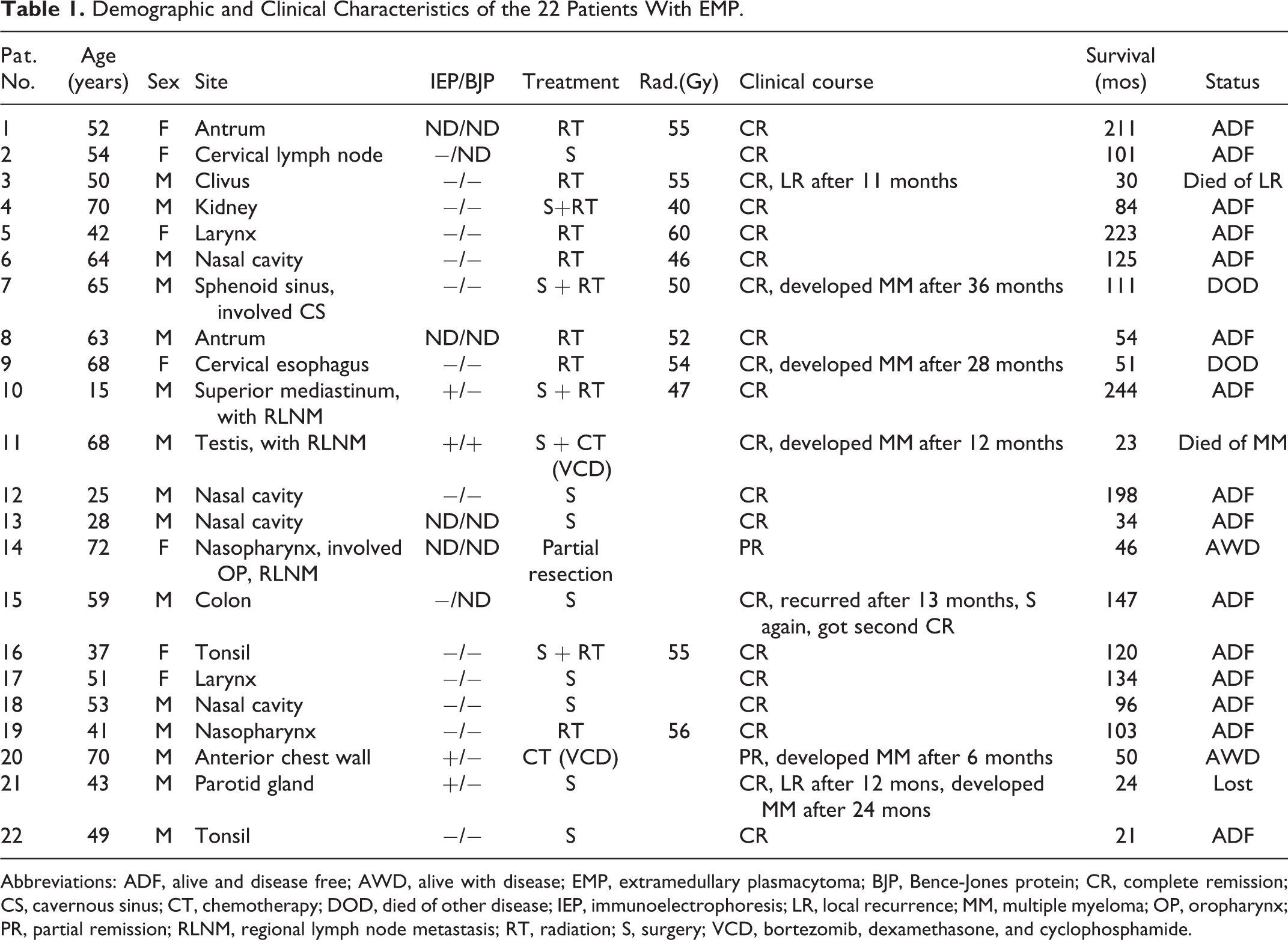
Abbreviations: ADF, alive and disease free; AWD, alive with disease; EMP, extramedullary plasmacytoma; BJP, Bence-Jones protein; CR, complete remission; CS, cavernous sinus; CT, chemotherapy; DOD, died of other disease; IEP, immunoelectrophoresis; LR, local recurrence; MM, multiple myeloma; OP, oropharynx; PR, partial remission; RLNM, regional lymph node metastasis; RT, radiation; S, surgery; VCD, bortezomib, dexamethasone, and cyclophosphamide.
All patients had monofocal lesions, although 2 patients showed involvement of more than 1 adjacent structure. Symptoms relating to the tumor sites included local masses, nasal congestion, hyposmia, dyspnea, diplopia, dysphagia, dysphonia, and swelling. Two patients had lymph node metastasis at diagnosis, but none had distal metastasis.
Of the 18 patients assayed by serum IEP, 4 were positive, 2 each for IgD and IgG. The light chains were all type λ. Of the 16 patients who underwent urine tests for Bence-Jones protein, 1 was type λ positive. This patient’s serum light chain was also positive. Bone marrow aspiration showed less than 5% clonal plasma cells in all cases.
Treatment
Of the 22 patients, 8 (36%) underwent surgery alone, 7 (32%) received radiotherapy alone, and 4 (18%) underwent both surgery and postoperative radiation. One (patient 7) patient who had a sphenoid sinus tumor with invasion of the cavernous sinus underwent partial resection and postoperative radiation. Average radiation doses were 51 Gy (40-60 Gy). Patients who underwent radiation alone received higher doses (55 Gy; range 46-60 Gy) than those who received postoperative radiation (48 Gy; range 40-55 Gy). One (patient 14) patient with a nasopharyngeal tumor involving the Eustachian tube and oropharynx underwent partial resection but refused postoperative radiotherapy. One (patient 11) patient with a left testis tumor and regional lymph node metastasis underwent surgery and 4 courses of postoperative chemotherapy with bortezomib, dexamethasone, and cyclophosphamide (VCD). One (patient 20) patient with a large (diameter 14 cm) anterior chest wall tumor received 9 courses of chemotherapy with VCD.
Clinical Course and Survival
Patient follow-up is shown in Table 1. Fourteen patients remained disease-free for 21 to 244 months (median 102 months). One (patient 15) patient with a colon EMP experienced a relapse in the rectum. This patient underwent a second operation, achieved a second complete remission (CR), and remained disease-free for more than 10 years after the second surgery. At the time of this analysis, 15 (68%) of the 22 patients were living and disease-free; 2 were living with local disease, and 1 was living with MM. Four patients had died, 1 each of local recurrence, pneumonia, MM, and heart disease. One patient with a parotid tumor experienced local recurrence 1 year after surgery and achieved a complete response following radiation. This patient developed MM 1 year after radiation therapy and was subsequently lost to follow-up. Patient 7 had a sphenoid sinus tumor with cavernous sinus involvement at the time of diagnosis and underwent partial tumor resection and postoperative radiation (50 Gy dose). He developed MM 36 months after initial treatment and subsequently underwent 9 courses of bortezomib and dexamethasone (BD). The patient died of pneumonia 111 months after diagnosis. The 4 IEP-positive patients were patients 10, 11, 20, and 21. Their IEP were all negative after treatment. Patients 10, 11, and 21 achieved CR following treatment, while patient 11 developed MM 12 months after treatment. The latter patient received 3 courses of BD protocol chemotherapy after progression but subsequently died 24 months after initial treatment. Patient 21 underwent a total tumor resection and entered into CR after surgery. He recurred 12 months later, received 51 Gy of radiation, and achieved a second CR. However, he developed MM 12 months after radiation, refused chemotherapy at PUMCH, and was lost to follow-up. Patient 20 had a 14-cm chest wall tumor entered into partial remission after chemotherapy. After 6 courses of VCD, the tumor was reduced 5 cm and the patient’s IEP was negative. However, the patient experienced neuropathy 3 months after the last course of chemotherapy and was M protein positive by immunofixation electrophoresis. He was treated with 2 courses of MP protocol after progression. None of the patients who received radiation had severe side effects from the treatment.
The local recurrence rate was 13.6% (3/22) and the progression rate to MM was 22.7% (5/22). For survival outcomes, the 5-year overall survival rate was 84.2%. The 5-year progression-free survival rate was 67.3%, and the 5-year MM-free survival rate was 75.9%.
Literature Review
Our literature search identified 25 relevant studies reporting on patients with EMP (Table 2). In these reports, the head and neck regions were the most frequently involved area: 17 studies reported on disease in all body regions, and of these, 73% of patients with head and neck EMP (EMPHN). In the head and neck area, the sinonasal cavity, nasopharynx, and oropharynx are the most commonly involved sites. 2,4,7,9 -17 Extramedullary plasmacytoma also showed male predominance (2.3:1 in the 23 papers), which aligns with previously reported findings. 1,29
Review of Published Studies Including at Least 20 Patients With Extramedullary Plasmacytoma.
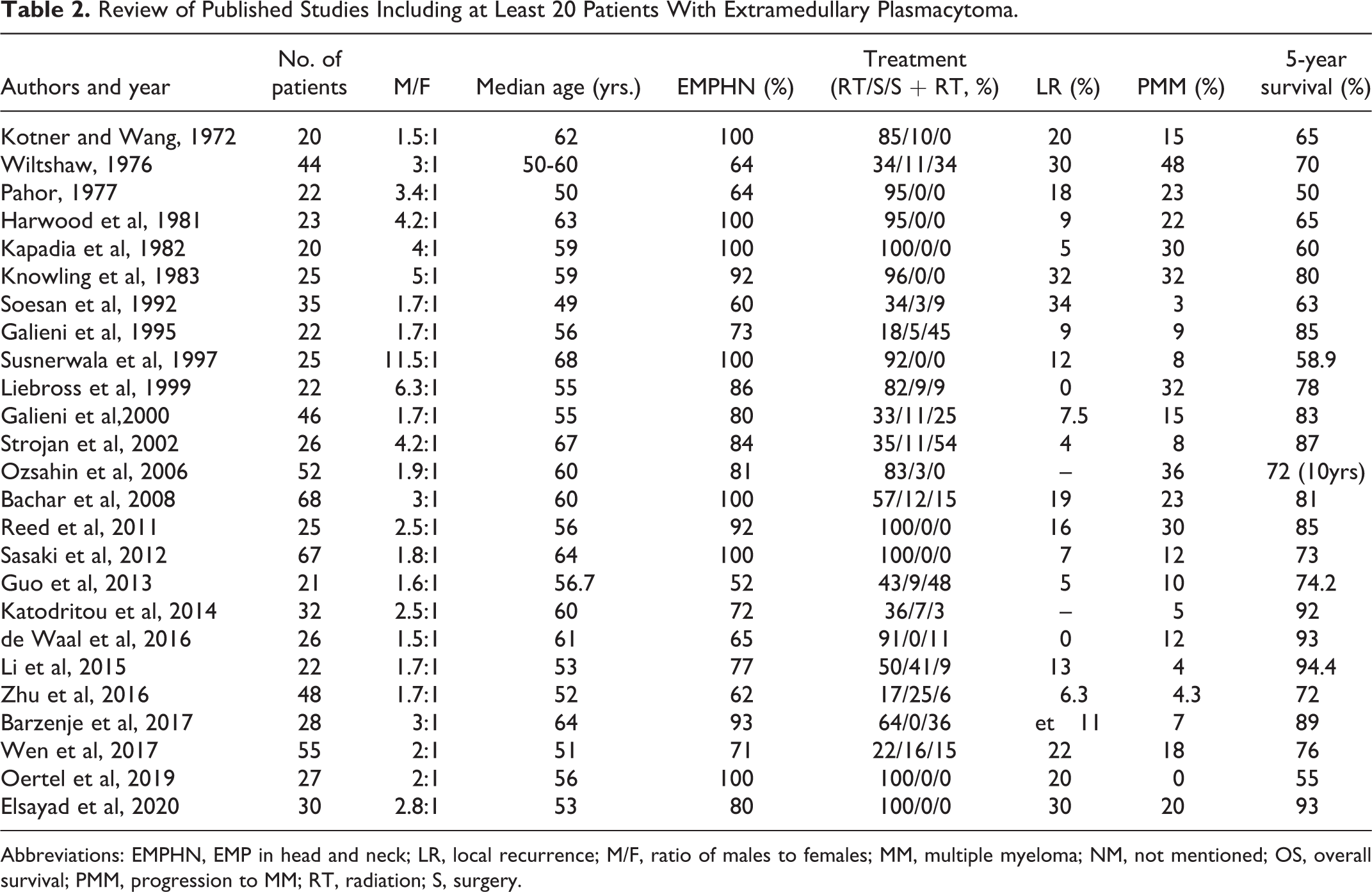
Abbreviations: EMPHN, EMP in head and neck; LR, local recurrence; M/F, ratio of males to females; MM, multiple myeloma; NM, not mentioned; OS, overall survival; PMM, progression to MM; RT, radiation; S, surgery.
Therapeutic strategies varied across these studies. Seven studies included only EMPHN patients, and in these, 76% of patients were treated with radiation alone, 4% with surgery alone, and 15% with surgery plus radiation. In the studies reporting on patients with EMP at all sites, 56% of patients underwent radiation alone, 17% underwent surgery alone and 19% received both. Surgery or surgery plus radiation was used more frequently for non-EMPHN than EMPHN patients.
Patient outcomes also varied in across studies. The 5-year local recurrence and progression to MM rates ranged from 0% to 34% and 0% to 32%, respectively. Five-year overall survival rates varied from 50% to 94.4%. Differences in overall survival between EMPHN and non-EMPHN patients were not reported.
Discussion
The mean age at EMP diagnosis is in the fifth decade of life, about 10 years younger than the mean age at diagnosis for MM. Although the median age of our patients was 52.5 years, 45% were younger than 50. The youngest patient, who had EMP in the superior mediastinum, was 15 years old at diagnosis, indicating that the disease can develop early in life. The literature review analysis supported our study findings, with a median age at diagnosis between 50 and 60 years old and male predominance.
A review of 869 patients with EMP showed that 714 (82.2%) of patients had EMP in the submucosa of the upper aerodigestive tract, with the remaining 17.8% having disease at other sites. 1 In our study, 77% of patients developed EMP in head and neck area. Other locations included the kidney, testis, chest wall, colon, and superior mediastinum, showing that EMP can affect widespread regions of the body. Seven studies included EMPHN patients only. For the remaining studies that covered EMP in all bodily regions, 73% of EMPs were located in the head and neck area. 5,18,29
Extramedullary plasmacytoma may spread locally. 2 Two patients in our study had involvement of 2 or more anatomic structures and another 2 patients had disease invasion of contiguous bones. The literature review found that 8% to 40% of patients with EMP had lymph node metastasis at diagnosis. 17,30 In our analysis, 3 (12%) of the 22 patients had regional lymph node disease at diagnosis, consistent with these earlier reports.
The key diagnostic criteria in our cohort analyses were based on morphologic and immunohistochemistry findings of monoclonal plasmacytoma without involvement of bone marrow or bones, except for erosion of contiguous bones caused by direct tumor invasion. Immunoelectrophoresis of serum or urine may show evidence of monoclonal disease. All of the patients in the present study were strictly diagnosed based on pathology findings, imaging and bone marrow aspiration, and serum immune fixation tests to exclude solitary plasmacytoma of bone or MM.
Although no randomized trials for EMP have been performed to date, radiation is widely reported to be an effective treatment. Surgery is also an option for patients with resectable disease. 1,31 In our cohort, the prognosis for patients who received surgery was quite favorable. Most of the patients were from rural areas in China, where radiation is more expensive and time-consuming than surgery. Surgery without functional impairment is an effective treatment option for such patients. If complete tumor resection is impossible or regional lymph nodes are involved, surgery combined with radiation is recommended. 1 However, clear margins are crucial for surgical resection. The likelihood of lymph node metastasis varies between patients, therefore regular lymph node dissection is not recommended for most but is recommended in patients with proven positive lymphadenopathy. Two (patient 10 and patient 11) of the 3 patients with regional lymph node metastasis had very different prognosis due to differences in their age and health status. The prognosis indicated that radiation is more efficacious than chemotherapy for EMP patients with lymph node metastasis.
Among the few cases reported in the literature, even fewer studies have compared the prognosis of head and neck EMPs with non-head and neck EMPs. Zhu et al 25 reported that the tumor site was not a prognostic factor for EMP patients. Alternatively, Gerry and Lentsch 31 compared data from the SEER database and found that head and neck EMPs had significantly better outcomes than EMPs from other sites. In our series, patients with head and neck EMPs had similar results with patients with non-head and neck EMPs.
While some literature showed that the local control and survival rate of radiation alone is better than surgery alone, 19,23,26 several studies found that surgery had a higher local control rate than both radiation and combined treatment. 1,31 Although some authors reported that a combined treatment of surgery and radiation had a more favorable prognosis than either radiation or surgery alone, 19,20 more studies found that patients did not benefit from a combination treatment. 6,23,25 Our study showed that surgery alone for patients with resectable disease while having no major function impairment had excellent results. Due to the heterogeneity of the cases and treatment options in the literature review, it is difficult to statistically compare the prognosis outcomes of surgery, radiation, or combined treatments. This needs to be further investigated using prospective randomized studies.
The average recommended radiation treatment dose for EMP is 50 Gy (range, 45-55 Gy). It has been shown that doses larger than 45 Gy are effective for treating EMP. In our study, the average radiation dose was 51 Gy, with the average radiation dose being higher in patients who underwent radiation alone (54 Gy) than in those who underwent radiation following surgery (48 Gy). As discussed, we were more conservative in administering the radiation protocol for patients from rural areas. Only 1 patient received a low dose of 40 Gy postoperatively. The remaining patients all received doses greater than 46 Gy. All patients tolerated the radiation well without serious adverse side effects.
Four patients in our study were positive in serum or urine IEP testing for monoclonal light chain protein. Three were treated with combined therapies. Only 1 achieved long-term progression-free survival. Two of the 4 died, while the remaining patient progressed to MM quickly after treatment. This indicates that patients with positive IEP tests may have poorer prognosis and need more aggressive treatment.
Generally, EMP responds well to therapy and has a positive clinical course with treatment. The 5-year local control rate and 5-year survival rate in most reports were between 60% to 90% and 70% to 90%, respectively. In our study, 2of the patients who died were treated with radiation alone, and the third was treated with surgery alone. Another patient (patient 7) progressed to MM and was treated with partial resection combined with postoperative radiation. He achieved CR after treatment but developed MM 3 years later. He died of pneumonia 111 months after initial diagnosis. Four patients underwent surgery plus radiation. Three of these patients, who underwent total resection with negative margins, were alive and tumor-free at the time of this analysis, whereas the fourth underwent partial tumor resection, progressed to MM 3 years later, received chemotherapy, and died of pneumonia 6 years after progression. Due to the small number of patients in this study, we could not compare outcomes between patients who underwent radiation alone, surgery alone, and surgery plus radiation. However, our findings indicate that surgery alone is an effective treatment for localized disease. The patients who underwent combined treatment either had tumors located in crucial areas (patients 4, 7, and 10) or did not have adequate surgical margin because the diagnosis was unclear at the time of surgery (patient 16). Postoperative radiation was effective in all 4 of these patients.
In conclusion, EMP is a rare plasma cell dyscrasia with a favorable clinical outcome. Complete resection is a viable option for patients with resectable tumors as radiation. Patients with regional lymph node metastasis or positive IEP results may have poorer prognosis and need more aggressive treatment.
Footnotes
Authors’ Note
Xiaoli Zhu and Li Wang contribute equally to this work.
Acknowledgments
The authors gratefully acknowledge Dr Xiaohua Shi and Zhiyong Liang of the pathological diagnosis for the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.