
Abstract
Introduction:
The presented case is unique as the patient presented with biopsy-proven papillary thyroid carcinoma (PTC) of the thyroid gland with an incidentally found concurrent thyroglossal duct cyst (TGDC) on computed tomography (CT). The patient was managed with a one-stage procedure.
Case Report:
A 26-year-old previously healthy female presented with a progressively enlarging neck lump over 6 months. Thyroid ultrasound revealed a 2.6 cm mass of the inferior right thyroid lobe, classified as TIRADS 5. Subsequent fine-needle aspiration of the mass confirmed PTC (Bethesda VI). A neck CT scan revealed a calcified, heterogeneous 2.6 cm mass in the right thyroid lobe along with a cystic lesion at the base of the tongue with likely extension into the floor of the mouth, consistent with a TGDC. The patient underwent simultaneous thyroidectomy and TGDC excision in a single operative session after discussion due to concerns for possible malignancy within the thyroglossal duct as well as possible enlargement of the TGDC leading to dyspnea or even dysphagia. At follow-up, the patient was doing well.
Discussion:
TGDCs are typically benign which is consistent with the findings in this case. The presence of biopsy-proven glandular thyroid cancer and an incidentally found TGDC present a unique challenge in surgical decision-making. In this case, there were no signs on imaging of malignancy of the TGDC so it was likely a primary glandular PTC. In this case, a one-stage procedure, combining total thyroidectomy and Sistrunk procedure, was selected based on the confirmed diagnosis of PTC with slight potential for synchronous cancer in the TGDC as well as prophylaxis against future aerodigestive tract symptomatology caused by the TGDC.
Background
Thyroglossal duct cysts (TGDCs) result from abnormal migration of thyroid cells during embryological development. They can occur anywhere along the thyroid’s migratory pathway from the base of the tongue to the inferior neck. TGDCs are relatively common, occurring in approximately 7% of the population, but only approximately 1% of TGDCs develop into thyroid carcinoma. 1 The most common malignancy of TGDC is papillary thyroid carcinoma (PTC), which accounts for up to 92.1% of TGDC-associated malignancies. 2
Standard management of TGDCs consists of the Sistrunk procedure (SP), which significantly reduces recurrence risk compared to simple cyst excision. 3 In thyroglossal duct carcinoma cases, the literature suggests that SP remains the primary treatment approach. However, an additional total thyroidectomy may be considered when dealing with highly aggressive disease and high-risk individuals.2,4 Some clinicians favor a more conservative approach toward synchronous thyroglossal duct carcinoma, consisting of SP with annual thyroid/cervical observation via ultrasound unless presenting with concerning features or otherwise deemed high risk.2,4 However, the incidence of benign TGDC found in the setting of biopsy-proven glandular thyroid cancer remains largely unknown.
The presented case is unique as the patient presented with biopsy-proven PTC of the thyroid gland with an incidentally found concurrent TGDC on computed tomography (CT). The patient was managed with a one-stage rather than a two-stage procedure.
Case
A 26-year-old female presented to her primary care doctor with a progressively enlarging neck lump over 6 months. She had no past medical history, no family history of thyroid cancer, and no prior surgeries. Thyroid function tests (TSH, T3, and T4) were within normal limits.
Thyroid ultrasound revealed a 2.6 cm mass of the inferior right thyroid lobe, classified as TIRADS 5. Subsequent fine-needle aspiration of the mass confirmed PTC (Bethesda VI). She was then referred to ENT for further evaluation and management.
During her initial ENT visit, the patient denied symptoms of hoarseness, orthopnea, and dysphagia and reported no history of neck radiation. Prompted by fullness in the neck, a neck CT scan was ordered to assist with surgical planning. It revealed a calcified, heterogeneous 2.6 cm mass in the right thyroid lobe along with a cystic lesion at the base of the tongue with likely extension into the floor of the mouth, consistent with a probable TGDC (Figures 1 and 2).
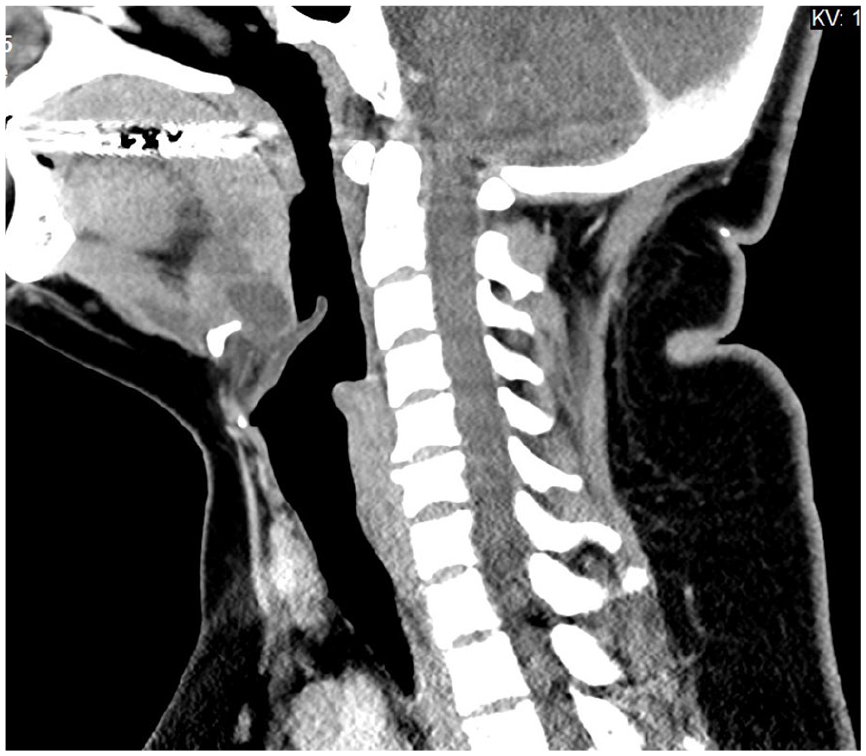
Sagittal CT image showing both TGDCs. CT, computed tomography; TGDC, thyroglossal duct cyst.

Coronal CT image showing thyroid mass that was found to be papillary thyroid cancer on fine-needle aspiration. CT, computed tomography.
The patient underwent simultaneous thyroidectomy and SP in a single surgery after discussion due to concerns for possible malignancy within the thyroglossal duct as well as possible enlargement of the TGDC leading to upper aerodigestive tract symptoms including dyspnea or dysphagia.
The pathology report confirmed stage 1 pT2 N0a, Mx papillary thyroid cancer, measuring 3.7 cm in the right thyroid lobe with 0/6 lymph nodes positive for metastasis. Both excised cysts from the base of the tongue were confirmed to be benign TGDCs. During 6 months of post-op follow-up, the patient was doing well with no recurrence of upper aerodigestive complaints.
Discussion
TGDCs are typically benign which is consistent with the findings in this case. The presence of biopsy-proven glandular thyroid cancer and an incidentally found TGDC present a unique challenge in surgical decision-making. PTC is currently hypothesized to arise de novo from a TGDC rather than from metastasis from the thyroid. 2 In this case, there were no signs on imaging of malignancy of the TGDC so it was likely a primary glandular PTC. It was also unlikely that the primary glandular cancer had spread beyond the thyroid as there was no lymphadenopathy present clinically or on imaging.
It is infrequent that patients with known thyroid cancer have concurrent findings of TGDC. As there was a low risk of malignancy in this patient’s TGDC, it would be reasonable to remove the TGDC at a later date to focus on the cancer operation. However, the base of the tongue orientation of the cyst (see Figure 1) meant that there was concern the patient could develop aerodigestive symptoms if the cyst were not resected at some point, and an extremely rare but unknown risk for synchronous PTC in the gland and the TGDC. As the patient would already be having surgery for her thyroid cancer, a single-stage surgery was discussed with the patient.
Upon learning of her incidentally found cyst, she expressed significant anxiety and a strong preference for simultaneous removal of the thyroid and TGDC. In such cases, addressing patient concerns and providing timely intervention can reduce stress and improve the patient’s overall well-being. By opting for a single-stage surgery, her concerns were addressed, and the delay and stress associated with a two-stage approach were avoided.
An alternative approach could have involved thyroidectomy with TGDC biopsy and close monitoring. Known as watchful waiting, this approach has been employed in select cases where the risk of malignancy in the TGDC was deemed low. One case study described this strategy—a TGDC was monitored closely until signs of malignancy were observed; at which point, an SP was performed. 5
Another advantage of a one-stage surgery was the reduced risk of anesthesia-related complications associated with undergoing 2 separate surgeries, including airway management issues, cardiac events, and deep vein thrombosis, increasing with the number of surgical procedures. The incidence of significant anesthesia complications has been reported to be approximately 1% to 2% in healthy individuals, with risks increasing in those with comorbidities. 6
Conclusion
We present a unique case of management of a patient with concurrent glandular thyroid cancer and an incidental benign TGDC. Careful consideration of the risks and benefits of various surgical approaches is required. In this case, a one-stage procedure, combining total thyroidectomy and SP, was selected based on the confirmed diagnosis of PTC with slight potential for synchronous cancer in the TGDC as well as prophylaxis against future aerodigestive tract symptomatology caused by the TGDC. While alternative approaches, such as biopsy with close monitoring of the TGDC, may be considered in cases with low-risk thyroid cancer and TGDC malignancy, our case highlights the complexity of decision-making and the importance of patient-centered care. The SCARE guideline was used to write this case report. 7 There was no funding for this study.