
Abstract
Papillary thyroid carcinoma in a thyroglossal duct cyst is very rare. We present the case of a teenage boy with a large thyroglossal duct cyst containing papillary thyroid carcinoma. There was no evidence of carcinoma within the thyroid gland, making this an important case of primary thyroglossal duct cyst carcinoma.
Thyroglossal duct cysts (TGDCs) are among the most common congenital masses of the neck and are the result of failure of closure of the thyroglossal duct by the ninth week of gestation. 1 They can appear anywhere along the path of the thyroglossal duct from the foramen cecum to the thyroid gland in the inferior neck. They are present in approximately 7% of the population, with 50% of TGDC containing ectopic functional thyroid tissue. 2 Carcinoma arising from the thyroglossal duct cyst (TGDCa), however, is rare, with the incidence being less than 1%. 1,2 Here, we present a case of a 15-year-old male with a primary papillary thyroid carcinoma of a TGDC.
A 15-year-old male presented to our clinic with a chief complaint of a midline neck mass first noticed following an upper respiratory infection 3 months prior. A neck ultrasound performed demonstrated an 8.2 cm × 8.1 cm × 5.4 cm neck mass with both solid and cystic components. The mass was also noted to have calcifications and was avascular with smooth lobulated margins. A computed tomography with contrast was completed demonstrating a cystic, septated thick and thin walled mass with some calcifications immediately anterior to the hyoid bone (Figure 1). There was no lymphadenopathy. Past medical history was noncontributory. Physical examination showed a 3.5 cm × 2 cm firm submental midline mass extending laterally into the left neck. Due to the presentation and location of the mass, the patient underwent a Sistrunk procedure. Intraoperatively, a large cystic mass was observed to be displacing the left submandibular gland inferior-laterally. The capsule of the mass was adherent to surrounding tissue and required meticulous dissection (Figure 2A). This dissection was difficult as the large, calcified, component of the mass was overlying the hyoid.

Computed tomography neck with contrast showing a large multiloculatd cystic and solid mass just anterior to the hyoid bone consistent with a thyroglossal duct cyst. Note the central calcifications and the increased wall thickness of the cystic components.

A, Thyroglossal duct cyst surgical specimen. The calcified component is central in the lesion with the central hyoid bone inferiorly at the midpoint of the specimen. The capsule was adherent to local structures requiring meticulous dissection. B, Total thyroidectomy surgical specimen. No evidence of papillary thyroid carcinoma is found on final pathology.
Final surgical histopathology of the TGDC demonstrated papillary thyroid carcinoma, classic type, arising in a background of papillary hyperplasia (Figure 3). Metastasis or direct extension from a thyroid primary could not be excluded. For this reason, as well as to facilitate radioactive iodine treatment, the patient underwent a completion thyroidectomy a month later without any complications (Figure 2B). No clinically overt pathologic central compartment lymphadenopathy was observed during the procedure. Final pathology of the thyroid gland was negative for thyroid carcinoma. He was referred to pediatric endocrinology for evaluation for postoperative radioactive iodine.
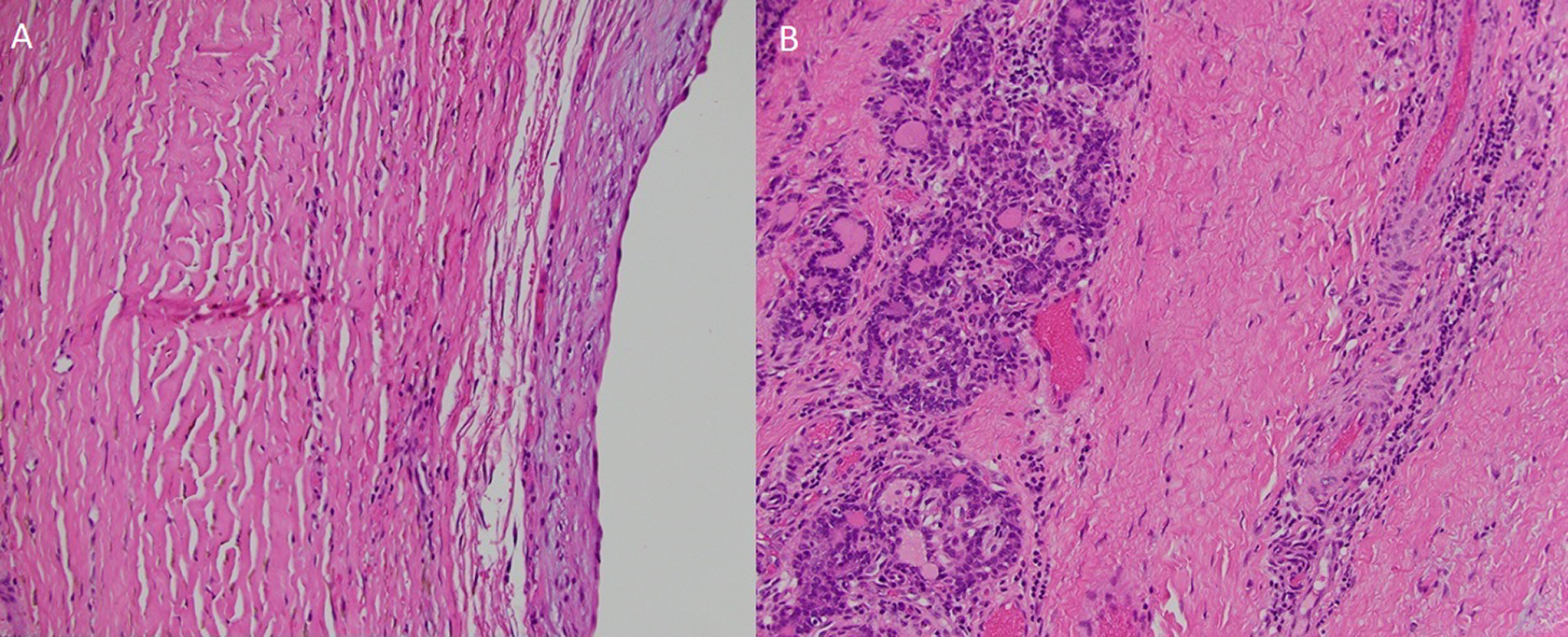
A, Microscopic examination demonstrates a thick fibrous wall lined by an attenuated cuboidal cyst lining. Portions of the wall contained thyroid tissues consistent with a thyroglossal duct cyst. B, Microscopic examination demonstrates a fibrous cyst wall containing thyroid tissues and chronic inflammation consistent with a thyroglossal duct cyst.
Discussion
Thyroglossal duct cysts represent the most common midline neck mass in children, with a 7% prevalence in the general population. 1,2 They are an embryologic remnant due to a failure to close the thyroglossal duct and can arise anywhere along the thyroid’s embryologic route of migration from the tongue base at the foramen cecum to the thyroid in the inferior neck. The thyroglossal duct forms together with the anterior portion of the hyoid bone during its descent, hence the relationship between the TGDC and the hyoid. Consequently, TGDCs typically present as an asymptomatic mobile midline neck mass near the hyoid bone. Up to 60% of TGDCs present at the level of the hyoid, with other locations being suprahyoidal (24%) and infrahyoidal (13%). 2 Patients, however, may also present with swallowing difficulties or relapsing throat infections. 1
Ultrasound is the initial imaging choice as it is inexpensive and readily available for children. 3 Due to the cystic nature of the lesion, however, the sensitivity of fine needle aspiration (FNA) biopsy is low and has been reserved only for investigation of findings suspicious for malignancy such as the presence of calcifications or solid components on ultrasound. 4,5
The treatment for TGDC is surgical removal to primarily prevent recurrent infections. The procedure of choice of nearly all TGDCs is the Sistrunk procedure, which includes the central third of the hyoid bone. 6
Fewer than 1% of TGDCs contain carcinoma, with papillary thyroid carcinoma the most common malignancy observed followed by squamous cell carcinoma. 1,2 In cases of papillary thyroid carcinoma of the TGDC, a concomitant papillary thyroid carcinoma is found in approximately 20% to 60% of patients. 5,7,8 While most TGDCs are diagnosed by the third decade of life, most patients diagnosed with TGDCa are adults with an average age of 39.5. 6 Cases of TGDCa in the pediatric population are exceedingly rare, with fewer than 30 cases reported in the literature to date. 9 This is reflective of the rarity of thyroid cancer in the pediatric population in general, which occurs with an annual incidence of 0.54 cases per 100 000 population. 10
Unfortunately, due to the rarity of this type of carcinoma, there is no consensus in the literature regarding treatment. 6,11 Most authors recommend performing a Sistrunk procedure at the very least, with further treatment usually involving evaluation of the lateral necks as well as the thyroid. 11 Based on these findings, further procedures such as a total thyroidectomy, lateral neck dissection, and postoperative radioactive iodine ablation may be indicated depending on the extent of disease per conventional management guidelines for thyroid cancer by the American Thyroid Association. 11,12 Prognosis is usually excellent, with a 99.4% survival rate reported in the literature. 6
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.