
Abstract
Introduction
The thyroglossal duct cyst (TGDC) stands as the most common congenital cervical malformation, representing approximately 70% of midline neck masses in children. Its onset typically occurs in childhood within 10 years of age, although the age of onset is <5 years and no significant differences based on gender have been observed. 1 The thyroglossal duct lesions originate from the incomplete degeneration of the channel formed by the decline in thyroid tissues during embryonic development, and the accumulation of secretions from residual ductal epithelium leads to cyst formation. A fistula is formed when a cyst has a secondary infection or ruptures on the surface of the skin. Ultrasonic examination, computed tomography (CT), and magnetic resonance imaging (MRI) differentiate TGDC from other neck masses, such as dermoid cysts, lymph nodes, and ectopic thyroid. 2 Notably, the “fistula” formed by infection and rupture manifests as a draining sinus tract. The embryological entity is the same as TGDC but is often described separately due to varied clinical manifestations. 3
To date, surgical resection remains the most effective treatment option for TGDC. Except for lingual TGDC (the cyst is located at the root of the tongue, approximately 0.6%-3%) 4 that can be treated through suspension laryngoscopy, the modified Sistrunk (mSis) procedure remains the primary option for children with neck TGDC. 5 The evolution of the TGDC removal procedure has spanned over a century. In 1893, Schlange proposed, for the first time, to remove the middle hyoid bone alongside cyst or fistula excision. 6 Subsequently, in 1920, Sistrunk introduced the classic Sistrunk procedure, 7 involving the excision of the middle hyoid bone and the foramen cecum. In 1928, Sistrunk modified this classic procedure, without emphasizing the removal of the foramen cecum of the tongue, but separating it to the mucosal layer of the mouth floor, retaining the sublingual root and maintaining a sterile environment for clean incisions in the neck 8 ; thus, birthing the mSis procedure.
In the current study, we retrospectively summarize the clinical features of TGDC in children, aiming to evaluate the curative efficacy of mSis procedure and investigate related factors associated with recurrence.
Materials and Methods
Design and Participants
This retrospective study reviewed all patients who underwent mSis procedure at Beijing Children’s Hospital, Beijing, China, and Baoding Children’s Hospital, Baoding, China, from March 2012 to December 2021. A total of 391 cases met the inclusion criteria, including 361 from Beijing Children’s Hospital and 30 from Baoding Children’s Hospital. The cohort comprised 244 males and 147 females, with ages ranging from 0.76 to 15.02 years (mean, 5.35 ± 2.81 years). Informed consent for surgery was obtained from both patients and parents. Inclusion criteria encompassed children aged 0 to 18 diagnosed with TGDC who underwent mSis procedure under general anesthesia. Exclusion criteria were as follows: (1) lingual TGDC preoperatively diagnosed by fibrolaryngoscopy or MRI; (2) children with preoperative clinical diagnosis of TGDC who did not undergo mSis procedure because the correlation between the cyst and the hyoid bone was not found during the procedure.
This study received approval from the Medical Ethics Committee of Beijing Children’s Hospital, Capital Medical University [No. (2022)-E-228-R].
Diagnosis Process
Data of medical history were collected, and all children underwent general and special examinations of the pharynx and neck (including thyroid and lymph nodes). Preoperative ultrasound examinations were conducted. Multidirectional scans were performed in the cross-sectional, longitudinal, and oblique directions of the mass with an ultrasound probe; the location (relative to the hyoid bone), size, shape (circular, elliptical, and irregular), the internal echo status of the mass (no echo, low echo, high echo, or uneven echo), the relationship with surrounding tissues, wall thickness, and boundary were recorded. Simultaneously, a thyroid ultrasound was performed to confirm the normal position and morphology of the thyroid gland. In addition, fibrolaryngoscopy was conducted to exclude lingual TGDC in this study. Twenty cases underwent MRI scanning to further clarify the property of neck mass and its relationship with surroundings for differential diagnosis. Eight cases underwent CT scanning to clarify the morphology and postoperative status of the hyoid bone.
Operative Procedure
Under general anesthesia and endotracheal intubation, all included children underwent a standard mSis procedure 8 performed by the team’s deputy senior or senior chief physician. The key steps of the operation were as follows7,8: a transverse incision was made across the neck at approximately the level of the hyoid bone, and the skin and platysma muscle were reflected; then the dissection was performed down to and around the cyst, freeing it from the surrounding tissues up to the hyoid bone; then the infrahyoid muscles attached to the hyoid were separated, and the central portion of the hyoid was removed. In children, we adopted the “non-fusion of the hyoid” therapy 10 and detected the lateral synovial joints of the cartilaginous junction between the hyoid body and the greater horn with monopolar electrocauterization. The body of the hyoid, along with the cyst tract, was then freed from the surrounding muscular structures; dissection continued deeply to include the tract and a core of the tongue musculature to the level of lingual mucosa and ligation, rather than removing the lingual mucosa; the tongue defect was tightly closed, and the remnant strap muscles were approximated. The bandage was wrapped with compression rather than drainage unless in an infection phase.
Follow-Up
Resected specimens of all patients were routinely submitted for pathological examination. All children completed the first reexamination 7 to 10 days post-procedure and were followed up by outpatient visits at 1, 3, and 6 months, and 1 year subsequently. Follow-up assessments included physical examination and ultrasound within the first postoperative year, followed by annual telephone follow-up. During follow-up, which concluded on March 1, 2023, spanning 15 to 156 months (mean duration: 69.62 ± 28.33 months), possible complications, such as pain, scar, infection, mass recurrence, dysphagia, pharyngeal fistula, tongue deviation, and neck movement limitation were investigated and analyzed. In cases of cervical infection or mass recurred during follow-up, ultrasound was performed at the earliest.
Statistical Methods
Statistical data were compared between the 2 groups using SPSS for Windows v12.0 (SPSS, Inc), and a P value <.05 was considered statistically significant. In multivariate analysis, Poisson regression was utilized instead of multivariate logistic regression due to a large difference in the number of cases between the recurrence and the nonrecurrence groups (382/9).
Results
Clinical Features
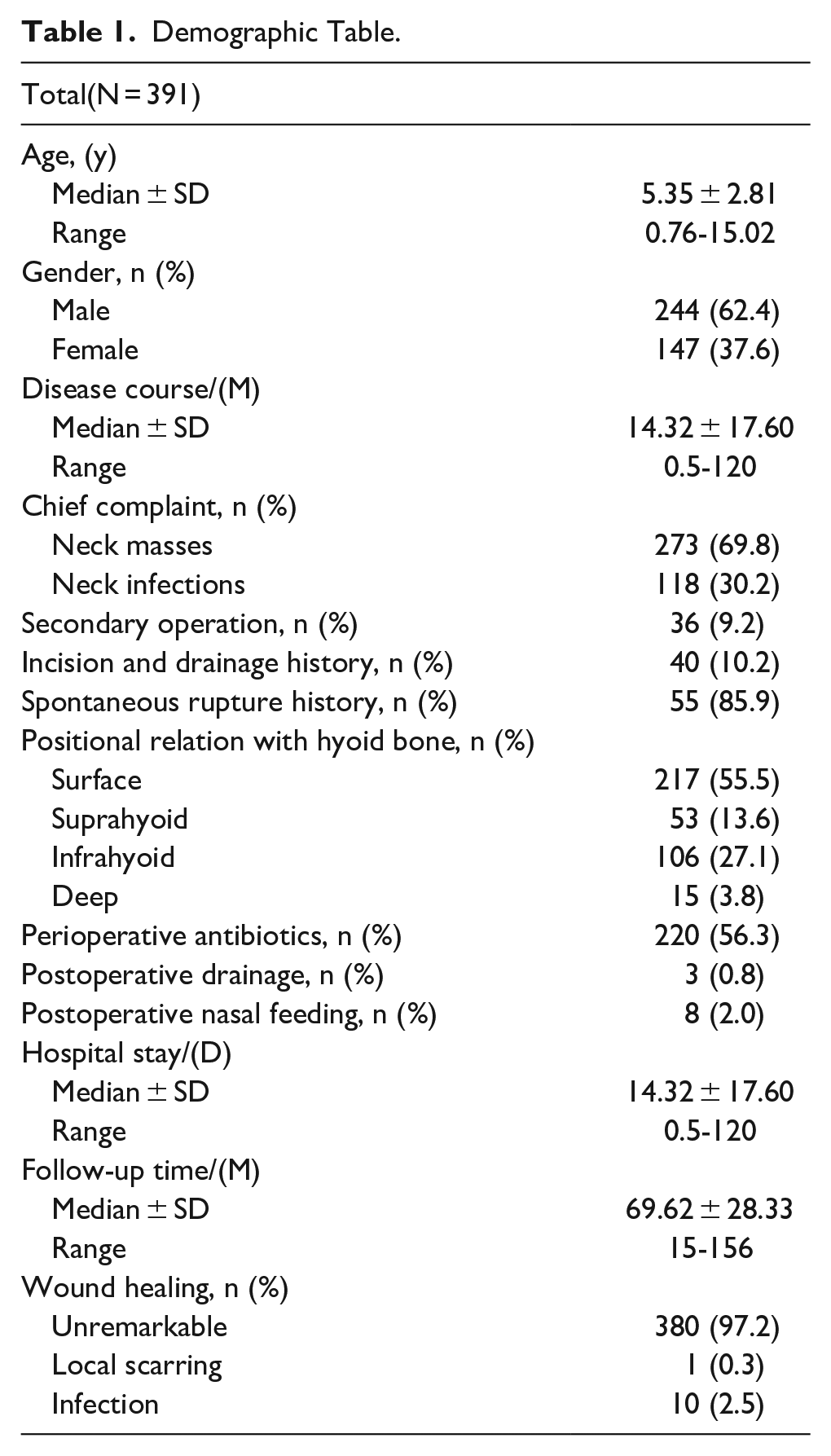
The clinical information of 391 children with TGDC is summarized in Table 1. The onset age of 72.1% of the cases fell within the range of 2 to 7 years old (Figure 1). Among the cases, 118 (30.2%) had a history of recurrent neck infection and 36 (9.2%) had undergone previous neck cyst and fistula resection surgeries, initially diagnosed as neck cyst (22 cases), TGDC (12 cases), and branchial fistula (2 cases), with only 6 cases having underwent partial hyoid bone resection in a previous operation. The disease course was 0.5 to 120 (average, 14.32 ± 17.60) months. Most cysts were situated on the surface of the hyoid (217, 55.5%) and infrahyoid (106, 27.1%), followed by the suprahyoid (53, 13.6%) and deep of the hyoid bone (15, 3.8%). Key ultrasound characteristics included (Figure 2): distinct boundary (90.10%), middle position of the neck (85.20%), and single cyst (82.6%). Approximately half of the cases had a cystic echo, with one-third having a maximum diameter >2 cm and sinus tract and fistula, respectively. Perioperative antibiotics were used in over half of the patients, while very few patients had postoperative drainage (3, 0.8%) and postoperative nasal feeding (8, 2.0%).
Demographic Table.
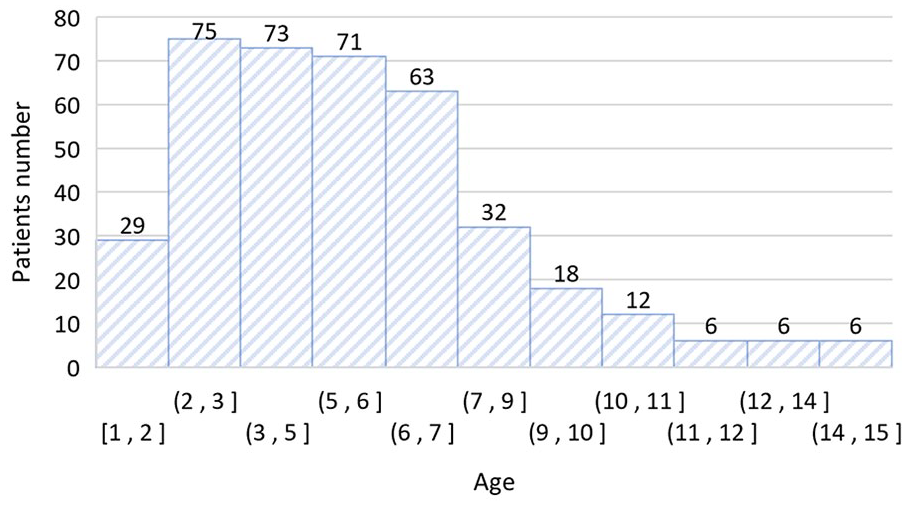
Age distribution.
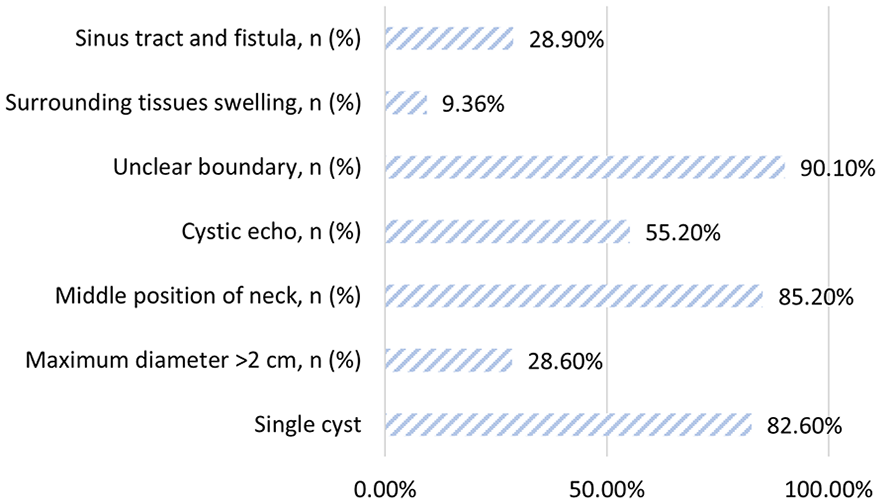
Ultrasound characteristics and proportion.
Safety and Efficacy
During the 15 to 156 month follow-up period, 10 children presented local wound infection, with no recurrence, and only one child expressed dissatisfaction with the incision scar. Notably, no other complications, such as bleeding, unplanned reoperation, unplanned intubation, pneumonia, nerve injury, dysphagia, pharyngeal fistula, tongue deviation, and limited neck movement, were reported. Regarding effectiveness, recurrence occurred in 9 children, resulting in an overall recurrence rate of 2.30%. Among those experiencing recurrence, 7 had cervical masses and 2 had redness, swelling, or pus in the neck wound. The recurrence time ranged from 0.5 to 34 (median = 5) months post-procedure, and the recurrence time of 8 children was less than 7 months.
Risk Factors for Recurrence
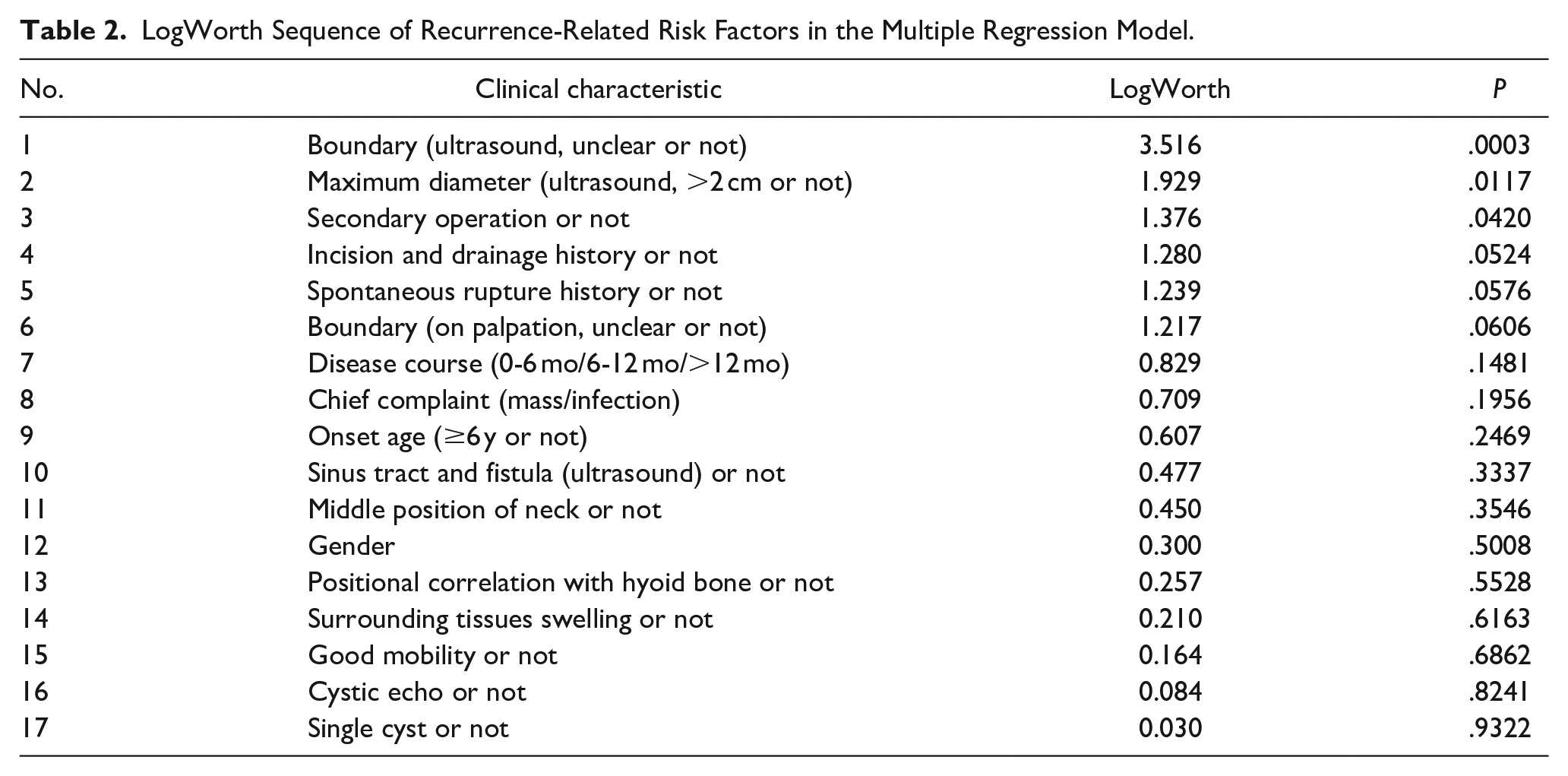
The LogWorth of 17 clinical features in the multiple regression model was calculated, with each feature arranged in ascending order based on the P value. Based on clinical value and statistical significance, 6 variables with LogWorth >1 and P value <.1 were included in the multivariate analysis (Table 2).
LogWorth Sequence of Recurrence-Related Risk Factors in the Multiple Regression Model.
Given the low recurrence incidence and substantial sample size difference between the recurrence and nonrecurrence groups (9/382), Poisson linear logarithm regression was employed to evaluate the related factors of recurrence. The frequency of recurrence, consistent with the Poisson distribution (Kolmogorov-Sminov Z value = 0.005 and P value = 1.000 in the Poisson distribution test), was used as the dependent variable, and the main effect included the top 6 independent variables in Table 2. The deviation value/degree of freedom in the goodness of fit of the model was 0.100, meeting the requirement of equal discreteness; while the Omnibus value of the global test was significant at 0.002. Statistically significant parameters are detailed in Table 3 (independent variables with P < .05). The results indicated that the P values of the 3 factors of clarity of the lesion boundary, surgical history, and maximum diameter of cyst in the model were <.05, indicating statistical significance and deeming them independent risk factors for recurrence. Consequently, the relative risk (RR) values for the aforementioned 3 risk factors, such as Exp (B), were 27.918, 10.054, and 6.606, respectively. This suggests that TGDC children with indistinct lesion boundaries under ultrasound, surgical history, and maximum diameter >2 cm were 26.918, 9.054, and 5.606 times more likely to experience recurrence compared to those without the aforementioned characteristics, respectively.
Multiple Regression Analysis (Poisson Regression) of Factors Related to Recurrence.
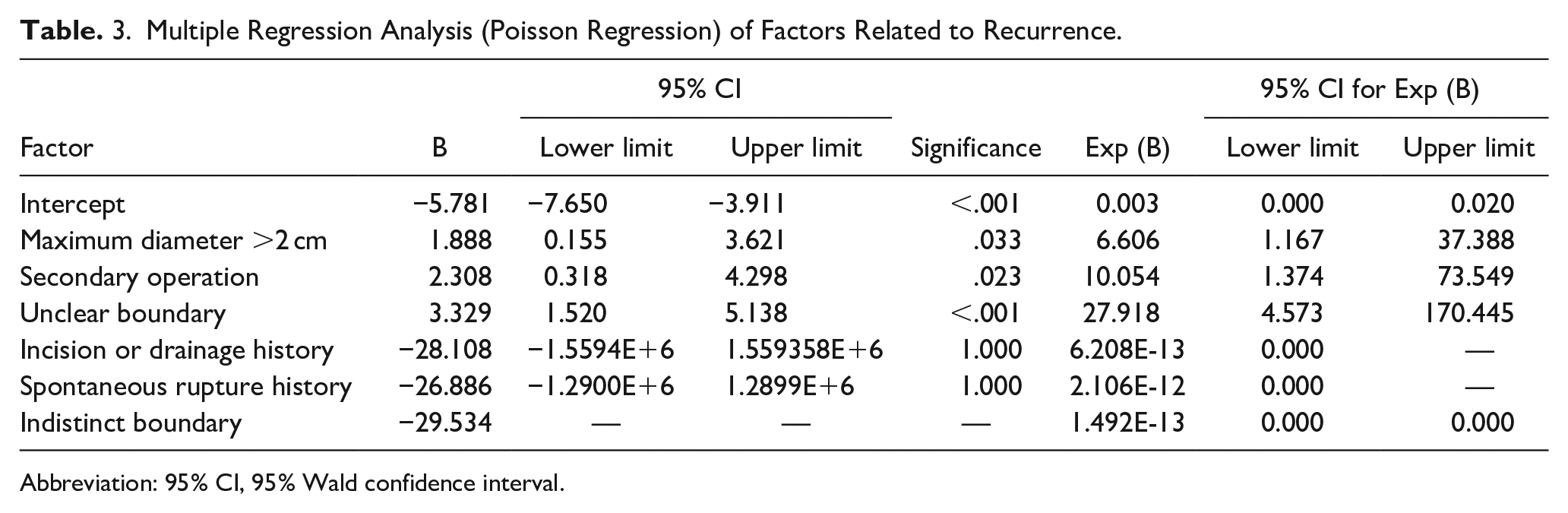
Abbreviation: 95% CI, 95% Wald confidence interval.
Discussion
About the Operation Procedure
In the traditional modified Sistrunk surgery, the central body or middle third of the hyoid bone was cut transversely with bone-cutting forceps on both sides of the hyoid body. However, the operation procedure adopted in the present study used needle electrocauterization to divide the cartilaginous junction between the hyoid body and the greater horn by combining the anatomical characteristics specific to childhood, as an overview of the hyoid bone discovered that until middle age, the connection between the body and the greater cornu is fibrous. 9 Consequently, for pediatric TGDC, needle electrocauterization can easily complete the division of the cartilaginous junction between the body and the greater horn without unnecessary bleeding. Similar findings have been reported by Ryu et al after studying 26 pediatric patients. 10
Regarding the tracking and anatomy of the foramen cecum, it is essential to emphasize the importance of maintaining the en bloc principle without attempting to identify a sinus tract in the region superior to the hyoid bone 11 and the cuff column of approximately 1 cm tissue volume was completely separated to the mucosal of lingual foramen cecum level, encompassing the mylohyoid muscles and the genioglossus. While Sistrunk suggested that the diameter of the cuff of the tissues around the lingual duct separated along the suprahyoid bone is about 3 mm, 8 Horisawa et al found extensive branches in suprahyoid and infrahyoid areas in the 3-dimensional reconstruction of the thyroglossal duct. 12 In 1950, Boyd proposed that the rupture of the thyroglossal duct in thickening and shortening of the proximal portion, and its epithelium resembles that of the tongue and frequently redevelops a lumen from which an extensive system of branches is grown. 13 Soucy and Penning, in their review of 44 pathological sections of TGDC, demonstrated that the thyroglossal duct delivers many dendritic branches to surrounding tissues. 14 Consequently, the resection range covered these hidden branch fistulas. Given that the separation occurs deep into the mucosal layer of the foramen cecum, dissection should be conducted using a cold knife to avoid the possible risk of pharyngeal fistula. This approach safeguards the healing process and facilitates visual observation to confirm the mucosal epithelium of the fistula in resected tissues. This procedure avoids entering the pharyngeal cavity, thus negating the purse string suture and adopting the figure-of-8 suture to consolidate the stumps. Since the fully bending backward position could lead to glossocoma and the tracheal intubation would be close to the epiglottis and the root of the tongue, the suture should not be extremely deep.
Recurrence and Risk Factors
The sample size of previous case-control studies on the application of mSis procedure in TGDC ranged from 24 to 251, with a recurrence rate varying between 1.6 and 16.1%.15,16 The present study has the largest sample size, involving retrospective data of mSis procedure in children, and the recurrence rate (2.30%, during 15-156 months of follow-up) was lower than the average reported by other studies. Statistical analysis revealed that the distinct lesion boundary, surgical history, and lesion diameter were independent risk factors for disease recurrence.
Leision boundary
In this study, the presence of an indistinct lesion boundary suggested that infection can lead to local cicatricial or inflammatory adhesions. Furthermore, the duration of surgery was 2 weeks after the infection was controlled. However, the aforementioned findings indicated that while the skin surface indicated controlled infection, the internal peripheral lesions could still be in the inflammatory recovery stage of the infection. During the infection stage of TGDC, the tissue is edematous and congested, and the fistula wall and small branches have poor elasticity and toughness, making them prone to rupture during separation. Although several studies have suggested an association between infection and recurrence,17-19 some reports do not support this association.20,21 The present findings demonstrated that the preoperative stage of occult infection could affect the complete resection of the small branches and fistulas during the procedure, leading to recurrence.
Secondary surgery
For patients with a surgical history of neck masses, local inflammatory or cicatricial adhesions, unclear anatomical level, blind operation present significant challenges for the complete resection of cysts and fistulas in secondary surgery, leading to residual and recurrent fistulas and the formation of small branches. Kim et al found that even experienced physicians using the classic Sistrunk procedure to resect TGDC had a mean recurrence rate was >4%, with resurgery failing in 33% of recurrent patients. 11 In the present study, the failure rate of resurgery in recurrent patients was 5.6% (2/36), highlighting the importance of detailed and thorough intraoperative procedures, particularly in children undergoing nonstandard surgeries, such as simple cyst resection and nondissection of the hyoid bone. Perkins et al demonstrated that if the hyoid bone was not dissected in the first surgery, resurgery after recurrence would increase the risk of a second recurrence. 22 Some studies reported successful experiences with central neck dissection in the treatment of recurrent TGDC, expanding the resection range of the Sistrunk procedure to include the anterior tracheal soft tissues to achieve en bloc resection; the width of the resected tissue volume of the strap muscles and hyoid bone was 3 to 4 cm, while that of the foramen cecum reached 2 to 3 cm. 23 Furthermore, although no recurrence or serious complication was observed after central neck dissection, risks, such as damage to the internal carotid artery, the vagus nerve, and entry into the pharyngeal cavity, could not be ignored. These findings valuable insights for improving the efficacy in the treatment of children with recurrent and refractory TGDC after repeated surgeries.
Leision size
In addition, some researchers proposed a correlation between the cyst size and recurrence. 21 Clinically, the volume of the cyst remains stable or changes slowly over time. If the cyst is infected, the volume may rapidly increase but decreases swiftly once the infection is controlled. The present study found that the diameter of the lesion (>2 cm) is a significant risk factor for recurrence. Thus, it is speculated that large cysts are prone to rupture during surgery and leak into surrounding tissues, resulting in indistinct boundaries. In addition, some children may still be in the recovery stage postinfection.
Limitations
However, the present study is not without its limitations. First, due to the limited sample size, coupled with the lower recurrence rate, the sample size of the recurrence and the nonrecurrence groups was significantly different, causing bias in the results. Second, the follow-up time was limited. Although the minimum follow-up time of this study (15 months) exceeded the recurrence time (<7 months) of most recurrent children (8/9), there remains a possibility of undetected relapses. Third, the duration of the case included in the present study was prolonged, allowing for the accumulation of the experience with the mSis procedure. During the continuous unification of surgical details, the surgical habits of different surgeons also have a potential impact on the findings. Fourth, the study comprised cases from 2 hospital districts. Although they both came from the North China region and underwent surgery by the same team of doctors, heterogeneity in medical services may have influenced the results.
Conclusions
The mSis procedure is currently the most widely used procedure in the clinical treatment of children with TGDC, offering a safe and effective treatment with fewer complications and a low recurrence rate of 2.30% in the study. In addition, the indistinct lesion boundaries, surgical history, and large diameter of the lesion are independent risk factors for TGDC recurrence in children.
Supplemental Material
sj-xlsx-1-ear-10.1177_01455613241257353 – Supplemental material for Modified Sistrunk Procedure in 391 Pediatric Thyroglossal Duct Cyst Cases: Clinical Analysis of Efficacy and Recurrence Risk
Supplemental material, sj-xlsx-1-ear-10.1177_01455613241257353 for Modified Sistrunk Procedure in 391 Pediatric Thyroglossal Duct Cyst Cases: Clinical Analysis of Efficacy and Recurrence Risk by Xiaodan Li, Ge Zhang, Yanzhen Li, Xuexi Zhang, Qiaoyin Liu, Nian Sun, Zhiyong Liu, Jinsheng Hao, Ziwei Chen, Yuwei Liu, Jie Zhang, Shengcai Wang and Xin Ni in Ear, Nose & Throat Journal
Footnotes
Acknowledgements
We would like to thank MedSci Healthcare for English language editing.
Data Availability Statement
All the authors listed have read through the article, approved for publication, and declared no conflict of interest. The data used to support the findings of this study are available from the corresponding author on request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Natural Science Foundation of China (82000991); Capital Health Development Scientific Research Project (2022-1-2092); National Natural Science Foundation of China (82271184); Respiratory Research Project of National Clinical Research Center for Respiratory Diseases (HXZX-20210202).
Ethical Statement
This study was approved by the Medical Ethics Committee of Beijing Children’s Hospital, Capital Medical University [approval no.(2022)-E-228-R] on December 9, 2022.
Patient Consent
All Patients’ parents signed the informed consent form for surgery. This study was a retrospective study that did not involve additional blood sampling and testing for the patient, nor does it increase the additional risk of the patient. Only clinical data of the patient were collected, and the true identity information of the patient was erased during statistical data collection, without involving any leakage of the patient’s privacy. Therefore, an application for exemption from signing an informed consent form of the study with the subject was submitted to the Ethics Committee and approved.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.