
Abstract
Introduction
Peritonsillar phlegmon is a frequent emergency in ENT practice, often with a favorable prognosis. 1 However, rare but severe complications, such as Lemierre’s syndrome, can alter the disease course and compromise both functional and vital prognoses.
Lemierre’s syndrome, first described in the early 20th century, is a septic thrombosis complicating an oropharyngeal infection with predominantly pulmonary septic emboli. 2 Septic thrombosis usually affects the internal jugular vein. Its extension into the cerebral venous sinus is extremely rare, especially in the cavernous sinus. 3
Herein, we report a rare and fatal case of peritonsillar phlegmon complicated by extensive cervicofacial fasciitis, with both internal jugular vein and cavernous sinus thrombophlebitis.
Case Report
A 72-year-old male with poorly controlled type II diabetes and chronic kidney disease with preserved diuresis presented to the emergency department with a painful swelling of the right hemiface, dysphagia, and fever for 3 days. Additionally, he developed dyspnea a few hours before admission. The patient reported self-medicating with a nonsteroidal anti-inflammatory drug (ibuprofen) and an antibiotic (amoxicillin).
On physical examination, he was conscious (Glasgow Coma Scale score: 15/15), febrile at 38.5°C, tachycardic at 100 bpm, with a blood pressure of 130/80 mmHg. He exhibited dyspnea with suprasternal retraction. Oxygen saturation was 93% on room air. A painful red swelling involved the right hemiface, including the ipsilateral orbit, extending to the right lateral cervical region (levels Ib and II) (Figure 1). Oral cavity examination revealed a trismus (2-finger width), a bulging, and deformed right anterior pillar with contralateral uvula deviation. Nasofibroscopy showed right lateral pharyngeal bulging extending from the rhino pharynx to the hypopharynx. Cranial nerve examination was normal, with no signs of meningitis or sensorimotor deficits. Ophthalmologic assessment revealed moderate axial exophthalmos with normal extraocular movements and visual acuity. Laboratory tests showed leukocytosis (14,000/mm3) and an elevated C-reactive protein (150 mg/L).

Right hemiface cellulitis extending into the right cervical region (red arrow).
The patient was urgently hospitalized and started on empirical intravenous antibiotic therapy with cefotaxime (2 g 3 times daily) and metronidazole (500 mg 3 times daily). Urgent contrast-enhanced computed tomography (CT) of the brain and facial mass revealed extensive cervicofacial cellulitis centered on an ipsilateral peritonsillar phlegmon, extending into the retro-styloid and pre-styloid spaces, as well as the infratemporal fossa. Orbital involvement included moderate right exophthalmos with preseptal fat infiltration. Cervical imaging showed cellulitis extending into levels Ib and II with a poorly demarcated hydro-aerial collection (45 × 40 mm) exerting a significant mass effect on the aerodigestive axis (Figure 2A). Additionally, thrombosis of the right internal jugular vein (Figure 2B) and right transverse sinus (Figure 2C) was identified. The thoracic and pulmonary regions were unremarkable.
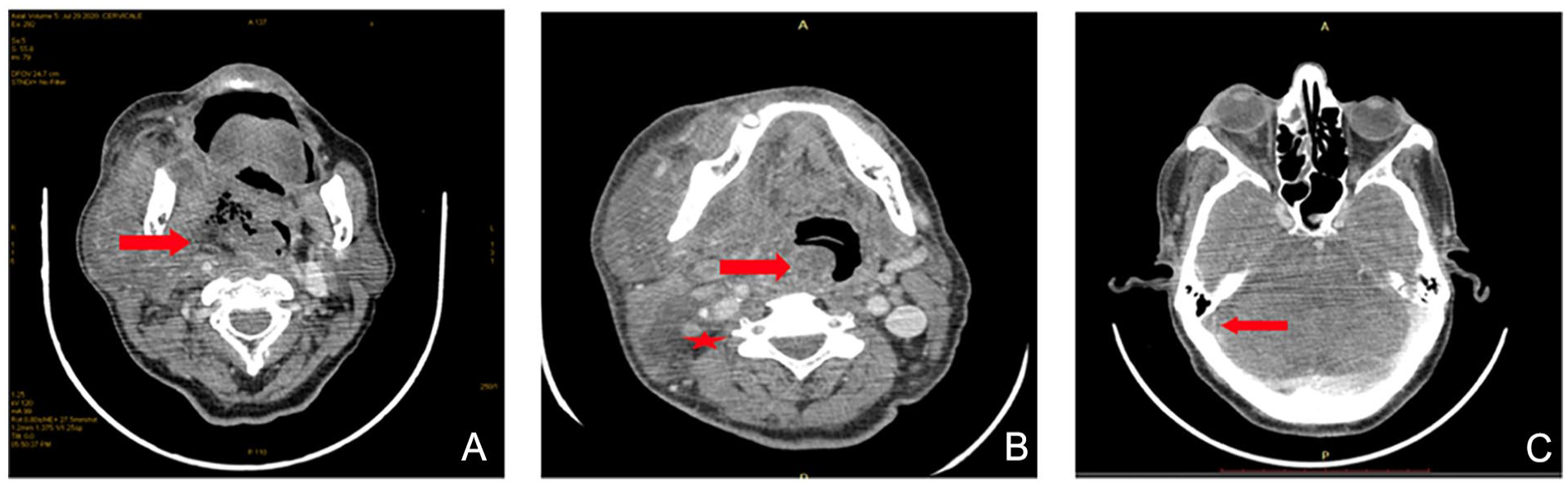
Contrast-enhanced cervical CT scan in axial section showing: (A) A right peri-tonsillar hydro-aerial collection exerting a mass effect on the pharynx (red arrow). (B) A mass effect on the aerodigestive tract (red arrow) and the absence of opacification of the right internal jugular vein (red star). (C) Absence of opacification of the right transverse sinus (red arrow). CT, computed tomography.
The patient underwent emergency surgery under general anesthesia with awake nasofibroscopic intubation. A wide peritonsillar incision allowed endo-buccal drainage, followed by a prophylactic tracheostomy to prevent potential laryngospasm and facilitate postoperative care. Microbiological samples were collected. The patient was transferred to the intensive care unit (ICU) postoperatively.
One hour after awakening, the patient exhibited a decline in consciousness without fever or meningitis signs. This was accompanied by rapid visual deterioration on the right side, characterized by ptosis, severe exophthalmos, significant chemosis preventing eyelid closure (Figure 3), ophthalmoplegia, and asymmetric pupils with a positive Marcus Gunn sign indicating an afferent pupillary defect. Based on clinical progression, the patient was diagnosed with Cavernous Sinus Thrombosis (CST). Due to renal insufficiency, a second contrast-enhanced CT was deemed harmful, and urgent magnetic resonance angiography was unavailable.

Chemosis of the right eye (right arrow).
In the ICU, the patient continued on cefotaxime and metronidazole, with the addition of gentamicin (320 mg daily). On the third day of hospitalization, microbiological cultures identified Klebsiella pneumonia and Candida spp. Antibiotic therapy was modified to piperacillin/tazobactam (4 g 4 times daily), vancomycin (1 g over 1 hour followed by 2 g daily via syringe pump), and fluconazole (400 mg twice daily). The patient also received therapeutic anticoagulation with unfractionated heparin (4 mg/kg daily) and continuous insulin infusion (adjusted every 2 hours based on finger-stick glucose monitoring).
On the fourth day of hospitalization, the patient developed septic shock, requiring norepinephrine infusion. His condition rapidly deteriorated, leading to multiorgan failure. Despite aggressive resuscitation, he suffered cardiac arrest and could not be revived.
Discussion
Lemierre’s syndrome most commonly occurs in immunocompetent adolescents and young adults. However, it has also been observed in its severe complicated form in immunocompromised patients, as was the case with our patient. 4 Most cases develop from oropharyngeal infections such as pharyngitis and tonsillitis. 5 A dental origin is rarely implicated, accounting for less than 2% of all cases. 3
Septic pulmonary embolism is the most frequent complication of Lemierre’s syndrome, occurring in 79% of cases. 3 In contrast, neurological complications are much rarer. It may involve cranial nerves IX, X, and XII due to local spread of infection and/or central nervous system involvement, such as meningitis or ischemic stroke. 6 Extension into the cerebral venous sinuses, especially the cavernous sinus, is extremely rare. CST has an incidence of 3 cases per million people per year. 7 It is more commonly associated with facial skin infections and sphenoethmoidal sinusitis than with peritonsillar abscesses. 8 In the case of sphenoethmoidal sinusitis, CST is explicated by retrograde infection via the ophthalmic veins, which, being valveless, facilitate infection retrograde spread from the face or orbits to the cavernous sinus. 9 However, in the case of internal jugular vein thrombosis, it may be explicated by retrograde propagation of the internal jugular thrombosis to the cavernous sinus. 10 In addition, different infection spread pathways have been proposed, including venous, arterial, and lymphatic routes. 6 The bilateral anastomosis between the 2 cavernous sinuses explains why thrombosis can become bilateral. 11
The most commonly implicated pathogens are Fusobacterium necrophorum and Staphylococcus aureus. Rarer bacteria, such as Streptococcus constellatus and Prevotella intermedia, have been isolated in cases of Lemierre’s syndrome with cavernous sinus involvement. 3 Additionally, fungal agents like Aspergillus and Rhizopus have been reported in CST secondary to sinusitis. 8 In our patient, microbiological cultures identified Klebsiella pneumonia and Candida spp. To our knowledge, these pathogens have not been previously reported in other cases of septic thrombosis.
CST is clinically revealed by ophthalmic signs. The combination of ptosis, painful ophthalmoplegia, and chemosis forms a characteristic triad suggestive of the diagnosis. In fact, in our patient, the diagnosis of CST was strongly suspected due to the acute onset of this triad following Lemierre’s syndrome. Neurological signs may also be observed, such as headaches, cranial nerve involvement, and even altered consciousness. 12
Contrast-enhancement cerebral and facial CT scan reveals the causal infection (in our case, the right peritonsillar phlegmon and cervicofacial cellulitis), often showing indirect signs of CST, such as thickening of the superior ophthalmic vein and irregular filling defects in the cavernous sinus. Angio-MRI is more sensitive. It highlights an abnormal heterogeneous signal from the cavernous sinus and a hyperintense signal from the thrombotic vascular sinuses, along with the deformation of the cavernous portion of the internal carotid artery. 13 The extent of the thrombi should then be assessed, and central complications such as ischemic stroke should be investigated. 13
In our patient, thrombosis of the right internal jugular vein and the ipsilateral transverse sinus was confirmed by CT. However, CST, which developed within a few hours, could not be radiologically confirmed due to renal insufficiency, which contraindicated a second contrast injection.
Blood cultures can help identify the causative pathogen. Repeated local microbiological samples and blood cultures may pinpoint the causative organism. The treatment for Lemierre’s syndrome, with or without extension to CST, is medical and surgical, primarily relying on antibiotics and surgical drainage of the infectious entry point. 14
A broad-spectrum empirical antibiotic therapy is used as a first-line treatment, typically combining a third-generation cephalosporin, an anti-staphylococcal agent, and metronidazole. Intravenous antibiotic therapy is continued for at least 3 to 4 weeks until clinical improvement is achieved.
An antifungal agent may be added if a fungal etiology is suspected. In our patient, fluconazole was prescribed following the isolation of Candida spp., guided by antifungal susceptibility testing.
In typical Lemierre’s syndrome, the use of anticoagulation remains controversial, with most authors opposing its routine prescription.15,16 However, in the case of extension to CST, anticoagulation is generally recommended, although no clinical trials have been conducted. Retrospective studies have reported a significant reduction in ocular and neurological complications, such as blindness, ophthalmoplegia, seizures, and strokes, in patients receiving anticoagulation for 2 to 6 weeks.15,16
The use of corticosteroids is also controversial. They are mainly indicated in cases of cranial nerve involvement, severe orbital congestion to reduce pressure around the optic nerve, or adrenal insufficiency secondary to pituitary dysfunction. 8 The recommended drug is dexamethasone, administered at 10 mg every 6 hours. 17
Surgical drainage is indicated to control the primary infectious source.
The mortality rate in case of extension to cavernous sinus has significantly decreased from 100% before the advent of antibiotics to 20% since 1940. 18 However, this decline has come at the expense of an increased rate of severe long-term functional sequelae such as blindness and ophthalmoplegia. 7
The rapidly fatal outcome in our patient was not only due to Lemierre’s syndrome cerebral extension but was also influenced by immunosuppression, diabetic decompensation, extensive infection, and hypoxia.
Conclusion
Any oropharyngeal infection, no matter how minor, must be properly and promptly managed, as it carries the risk of leading to severe, potentially life-threatening complications, such as Lemierre’s syndrome. Lemierre’s syndrome prognosis is particularly worsened by the extension to intracranial sinuses. A rapid diagnosis remains the best guarantee for optimizing patient management.
Footnotes
Acknowledgements
There were no acknowledgments to mention.
Author Contributions
All authors contributed substantially to the acquisition, analysis, and interpretation of data in addition to writing &editing. All authors approved the final version.
Data Availability Statement
The data underlying this case report will be shared on request with the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series. We anonymously reported clinical and imaging information concerning our patient’s case.
Ethical Principles
The authors declare that this work was conducted following ethical principles and with full respect for the anonymity of the patients.
Consent
Written informed consent was obtained to publish this case report and accompanying images. On request, a copy of the written consent form is available for review by the editor-in-chief of this journal.