
Abstract
Cavernous sinus thrombosis (CST) is a rare but life-threatening infectious disease whose diagnosis and treatment are challenging. CST can result in ocular and neurologic morbidities, as well as fatal systemic complications due to systemic thrombus. Occasionally, these clinical symptoms can be a result of contralateral sinusitis. A 75-year-old female presented with severe headache and fever. Magnetic resonance imaging revealed a multifocal filling defect in both cavernous sinuses, with heterogeneous enhancement and thrombosis of the right superior ophthalmic vein. Intravenous antibiotic was administered, and endoscopic sinus surgery was performed. The patient was discharged 40 days after admission and there were no neurologic symptoms and no evidence of sequelae during the 10-month follow-up. Symptoms of CST on the contralateral side are often missed, which delays initiation of appropriate treatment. When CST secondary to paranasal sinusitis is diagnosed, clinicians should consider contralateral as well as ipsilateral infection of the paranasal sinus. Preventing disease progression and complications through early and aggressive antibiotic administration along with sinus surgery is crucial.
Introduction
Cavernous sinus thrombosis (CST) is rare but life-threatening infectious disease. Despite antibiotics, the morbidity and mortality of CST are high and long-term sequelae are common. 1 The blood-filled space of the cavernous sinus contains the internal carotid artery, which is surrounded by cranial nerves such as the oculomotor nerve, trochlear nerve, and 2 branches of the trigeminal nerve. Blood drains into the internal jugular vein (IJV); CST can result in ocular and neurologic morbidities, as well as fatal systemic complications due to systemic thrombus.
Early diagnosis and aggressive treatment for CST are important to prevent complications. Sinusitis is a cause of CST, and the sphenoid sinuses are the most common primary site. 2 Because the cavernous sinus abuts the sphenoid sinus anatomically, infection of the latter may spread to the former.
Considering the anatomy of the cavernous sinus, clinical symptoms of CST can occasionally be caused by contralateral sinusitis. Three cases of CST secondary to contralateral sphenoid sinusitis have been reported.3 -5 We report a quite rare case of CST caused by contralateral sphenoid sinusitis with the literature review.
Case Report
A 75-year-old female presented with severe headache accompanied by a fever of 39°C. There was no underlying disease and an unremarkable medical history. In the initial laboratory test, the C-reactive protein (CRP) level was 357.8 mg/L. Brain, abdomen, and chest computed tomography (CT) was performed to identify the cause of fever, but showed unremarkable findings. The patient was treated with empirical antibiotics. On the third day of hospitalization, she developed right eyelid swelling and exophthalmos (Figure 1A), and a brain magnetic resonance imaging (MRI) was performed. The T2 image revealed sinusitis of the left sphenoid and ethmoid sinus. T1-weighted MRI with gadolinium contrast enhancement revealed multifocal filling defects in both cavernous sinuses, with heterogeneous enhancement and thrombophlebitis of the right superior ophthalmic vein (Figure 2). Paranasal sinus CT showed calcification in the left sphenoid sinus. On endoscopic examination, purulent discharge was observed in the left sphenoethmoidal recess and middle meatus. Based on the clinical and radiological findings, the diagnosis was CST by contralateral sphenoid fungal sinusitis. We added metronidazole and planned endoscopic sinus surgery and fungus ball removal. Surgery was performed under general anesthesia. First, left ethmoidectomy, antrostomy, and wide sphenoid sinusotomy were performed. A fungus ball with purulent discharge was detected in the sphenoid sinus. The fungus ball and part of the mucosa of the sphenoid sinus were removed and histological examination was performed. Discharge was collected for bacterial staining and culture. After endoscopic sinus surgery, the headache and eyelid swelling partially improved. The pathologic report cited aspergillosis with no mucosal invasion. Methicillin-resistant Staphylococcus aureus (MRSA) was identified by bacterial culture; for this reason, vancomycin was added to the treatment regimen. Fever improved after surgery. During the second week postoperatively, eyelid swelling, exophthalmos, and headache improved, and follow-up CT revealed improvement of thrombophlebitis and orbital infection. Fever had subsided and the CRP level had normalized to 2.2 mg/L. Follow-up brain MRI 1 month after surgery showed marked improvement of extensive thrombophlebitis in the cavernous sinus. The operation site was clear on endoscopic view. The patient was discharged on day 40 after admission, and there were no neurologic symptoms or evidence of sequelae during the 10-month follow-up (Figure 1B).
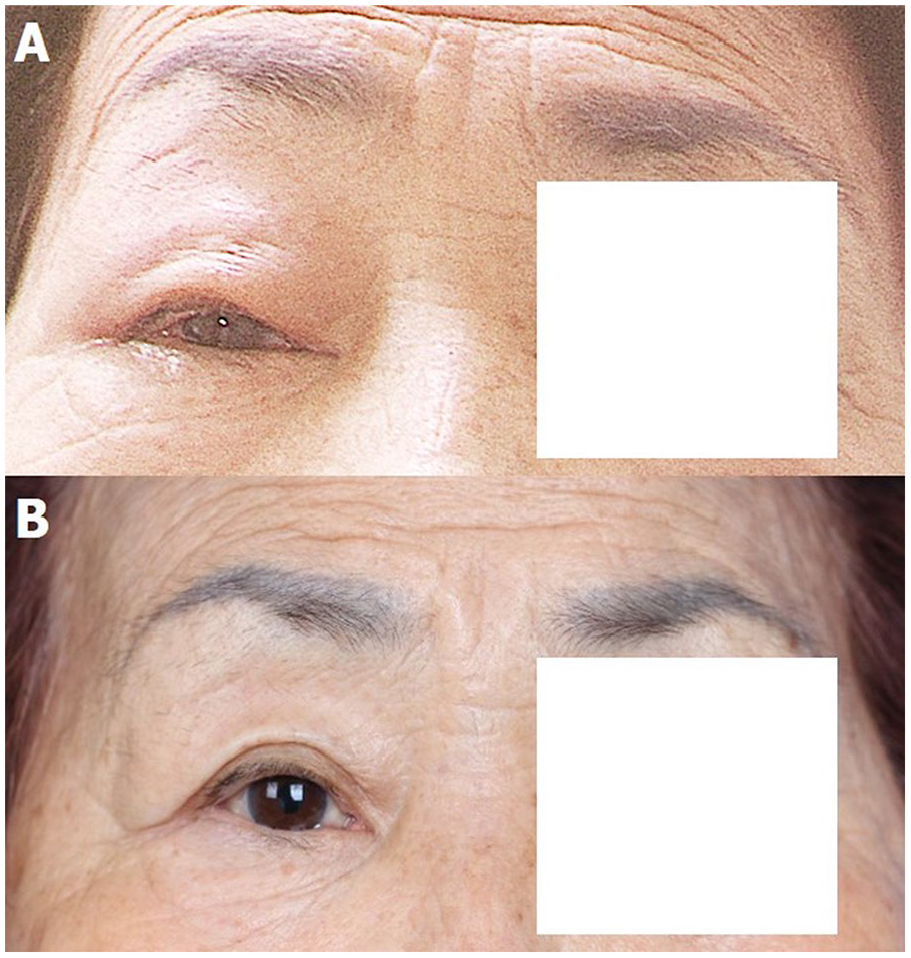
Clinical photograph. At initial presentation, the right eye showed ptosis, edema of the upper lids, periorbital edema, and congestion of the conjunctiva (A). After treatment, the orbital symptoms improved (B).
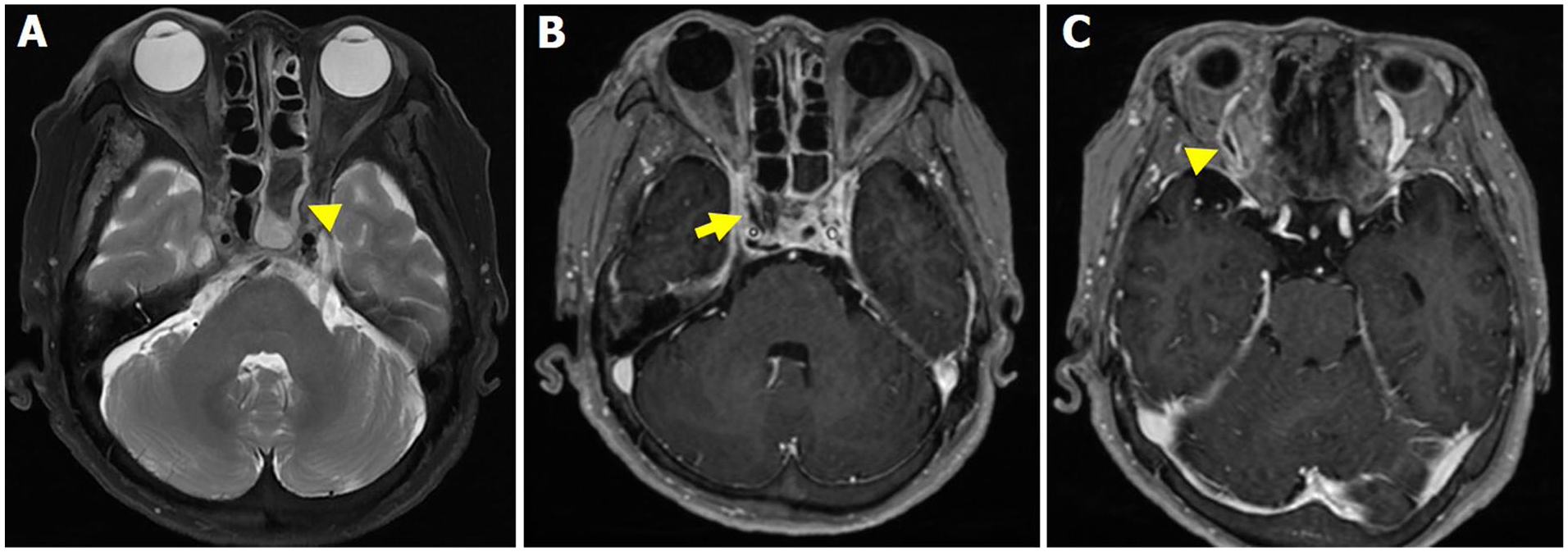
Brain MRI. Axial T2-weighted MRI shows a markedly hypointense fungus ball (arrowhead) with a hyperintense mucosal membrane of the left sphenoid sinus (A). Axial T1-weighted MRI with gadolinium contrast enhancement demonstrates multifocal filling defect (arrow) in the right cavernous sinus secondary to a thrombus (B). Axial T1-weighted MRI with gadolinium contrast enhancement demonstrates marked dilatation of the right superior ophthalmic vein (arrowhead) secondary to a thrombus; the left superior ophthalmic vein appeared normal (C). MRI, magnetic resonance imaging.
Discussion
CST, defined as the formation of a blood clot in the cavernous sinus, is a rare but fatal disease. There are 2 types of CST: aseptic and septic CST. Aseptic CST can occur after surgery or trauma, while septic CST can spread from a nasal furuncle, sphenoidal, or ethmoidal sinus or dental infection. 2 The most common causative bacterium is S. aureus, followed by Streptococcus. 6 Microorganisms can spread directly from an infected sphenoid to cavernous sinus through a communicating vein, osteomyelitis, or accompanying mucosal and bone defects. 7 In this case, CST developed from sphenoid sinusitis, and a fungus ball and mucosal defect of the posterior wall of the sphenoid sinus were found during surgery. MRSA was identified by bacterial culture.
Symptoms of CST with involvement of cranial nerves include ocular and neurologic morbidities such as ptosis, ophthalmoplegia, loss of vision, and trigeminal sensory loss. Wang et al reported 8 cases of CST secondary to sphenoid sinusitis. 8 All 8 patients had headache and ocular symptoms such as diplopia, optic nerve paralysis, or proptosis. Five of the patients had fever. If ocular symptoms are accompanied by headache and fever, CBT should be considered. All 3 symptoms, including ocular symptoms of right eyelid swelling and exophthalmos, were present in this case.
Contrast-enhanced CT and MRI are useful for diagnosing CST. Filling defects, a bulging contour, and asymmetrical opacification of the cavernous sinuses are direct indications of CST. Signs related to concomitant venous obstruction, including exophthalmos or congestion and dilatation of the superior ophthalmic vein, indirectly suggest of CST. 9 In this case, typical imaging findings including filling defect of the cavernous sinus and enlargement of the ipsilateral superior ophthalmic vein were observed, as in other CST cases.4,5,10
The ophthalmic and cerebral veins drain into the cavernous sinus, and the cavernous sinuses in turn drain into the superior and inferior petrosal sinuses, and ultimately into the IJV. Venous obstruction by CST may cause proptosis, chemosis, and edema of the eyelids. Furthermore, septic thrombophlebitis of the IJV can spread to the lung, kidney, and other organs; this condition is termed as Lemierre syndrome, which is life-threatening.
The mainstay of treatment of septic CST is early and aggressive antibiotic administration. To treat CST caused by paranasal sinusitis, antibiotics plus sinus surgery is the optimal strategy. 8 Endoscopic sinus surgery is necessary to address the source of infection in the paranasal sinus, and accelerates the resolution of clinical symptoms. The causative bacterium can be identified by culture of surgical specimens. Lize et al reported 7 cases of CST secondary to acute bacterial sinusitis, all of which underwent sinus surgery. 11
While awaiting culture results, empiric therapy using antibiotics effective against the most common causative bacteria, S. aureus and Streptococcus, should be administered. In cases arising from sinusitis, periodontitis, or facial cellulitis, regimens should include a third-generation cephalosporin and metronidazole. 12 Vancomycin can be administered if MRSA is identified. Because bacteria in the thrombus may survive until reperfusion of the dural venous sinuses, antibiotics should be administered for at least 2 weeks after the clinical symptoms have improved. 13 Antifungal agents are used if a fungus is the causative organism. 14 However, this is not necessary if the fungus is detected in the sinus as a fungal ball without mucosal invasion. In this case, antifungal agent was not initiated due to the absence of mucosal invasion, and the presence of only isolated fungal balls.
Anticoagulation treatment for patients with CST is controversial. Anticoagulants can be used to prevent propagation of the thrombus, but there is a risk of intracranial bleeding. According to a review of the role of anticoagulants in CST secondary to sinusitis by Bhatia et al, hemorrhage caused by anticoagulation is rare, and early adjunctive anticoagulation is beneficial in some patients with CST. 9 Early addition of anticoagulants can significantly reduce morbidity.8,15 However, there is no standardized type, dosage, or route of administration of anticoagulants, and the administration duration ranges from 2 weeks to several months. The authors suggested that long-term anticoagulation is not required unless thrombosis is persistent. Unfractionated or low-molecular-weight heparin can be used for short periods because the cavernous sinus is completely recanalized within 6 weeks. 11 In our case, anticoagulant treatment was not used.
The role of corticosteroid treatment for CST is controversial other than in cases with cerebral edema. Immunosuppressive effects of corticosteroids can accelerate sepsis, but also ameliorate cranial nerve dysfunction and orbital inflammation. 9
Permanent or transient neurologic deficits can develop despite treatment. Blindness, Horner’s syndrome, and V2 nerve hypoesthesia have been reported as long-term sequalae. 11 Seizure, pituitary insufficiency, and prolonged headache may occur as indirect complications. 9 The thrombus can spread to the IJV, potentially inducing Lemierre syndrome.
Conclusions
CST is rarely encountered, and diagnosis and treatment are challenging. Thus, despite advanced imaging techniques, the initiation of appropriate treatment is often delayed. CST may be missed when symptoms occur on the contralateral side of sinusitis, and clinicians should consider contralateral as well as ipsilateral infections of the paranasal sinus. When CST secondary to paranasal sinusitis is diagnosed, preventing progression and complications through early and aggressive antibiotic administration together with sinus surgery is crucial.
Footnotes
Authors’ Note
Consent
The authors obtained informed consent for the copyright and publication from the patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This work is original, and no portion thereof has been published previously, or is not under consideration for publication elsewhere.