
Abstract
Metastasizing pleomorphic adenoma is a rare entity that has the propensity for distant metastasis despite being histologically benign. We report the case of a 56-year-old woman with a long-standing right upper neck swelling and a recent-onset swelling over the left side of the scalp. Clinical workup did not reveal any other tumor deposits in the body. Complete excision of the right submandibular gland and the scalp swelling was performed. The case was diagnosed as metastasizing pleomorphic adenoma. The exact cause of the malignant manifestation of this histologically benign entity is unclear. The time of appearance of a metastatic deposit is highly variable and is usually preceded by a local recurrence. Further research on the malignant behavior of this entity is warranted.
Keywords
Background
Pleomorphic adenoma is the most common salivary gland tumor in adults and children. 1 Among the salivary glands, 80% of pleomorphic adenoma cases occur in the parotid gland, with the remaining 20% occurring in the submandibular and minor salivary glands. Pleomorphic adenoma is one of the few benign neoplasms that can undergo malignant transformation, 2 which is then known as carcinoma expleomorphic adenoma. 3
Interestingly, a rare entity named “metastasizing pleomorphic adenoma” (MPA), which remains histologically benign but metastasizes to distant locations, has been identified. 3 The clinical course of such cases may not be benign as more than 20% of patients die of this disease. 4 The metastasis is blood-borne and usually preceded by local tumor recurrence. 3 The most common site for the metastasis is the bones, followed by the lungs and then the lymph nodes. 5
We present a case of pleomorphic adenoma arising in the submandibular gland with metastatic deposits in the skull. We obtained written informed consent from the patient for participation in this study and publication of this report, including relevant images.
Case Presentation
We report the case of a 56-year-old woman who presented to our department with a right-sided upper neck swelling with a history of 20 years and another swelling over the left side of the scalp for the last 6 months. The swellings grew slowly over time, but there were no other significant symptoms associated with them. The patient did not have any comorbidities and reported a medical history of some abdominal surgery 15 years previously, the details of which were unknown.
Systematic examination results were found to be within the normal limits. There was a spherical solitary swelling with a firm consistency in the left submandibular region with a diameter of approximately 4 cm, which was digitally palpable and mobile. No regional lymphadenopathy was noted. We noted a 4-cm hemispherical, well-defined, solitary, fixed hard swelling on the left parietal region of the scalp with normal overlying skin. The rest of the examination results were unremarkable.
Investigations
The results of the blood workup were within the normal limits. Fine-needle aspiration cytology from the submandibular tumor revealed spindle-shaped, round, and plasmacytoid cells with bland, elongated-to-ovoid nuclei, set in a chondromyxoid matrix. No nuclear atypia, mitosis, or necrosis was noted. These findings suggested the possibility of pleomorphic adenoma.
Magnetic resonance imaging of the brain with contrast enhancement was performed, which showed a well-defined T1 hypointense with hyperintensities and T2 heterogeneous predominantly hyperintense and heterogeneously enhancing transcalvarial lesion with separations and central necrotic areas in the left parietal bone. It abutted the left parietal dura without involvement but with a mild mass effect over the parietal lobe. There was no infiltration of the superior sagittal sinus.
Ultrasonography of the neck showed a mass in the right level 1b region with internal vascularity. The thyroid gland was found to be normal. Positron emission tomography did not reveal any other suspicious foci in the body. A diagnosis of MPA of the right submandibular gland was made.
Management
We planned for right submandibular gland excision and excision of the scalp lesion in collaboration with the neurosurgical team. We performed an excision of the gland, which revealed a smooth firm yellowish mass arising from the lower pole of the gland (Figure 1A). The neurosurgical team performed a left parietal craniotomy with total gross excision of the mass with polymethyl methacrylate cranioplasty in a single sitting (Figure 1B-D). They reported that the mass had eroded the skull bone and invaded the periosteal layer of the dura. Postoperatively, the patient made an uneventful recovery.
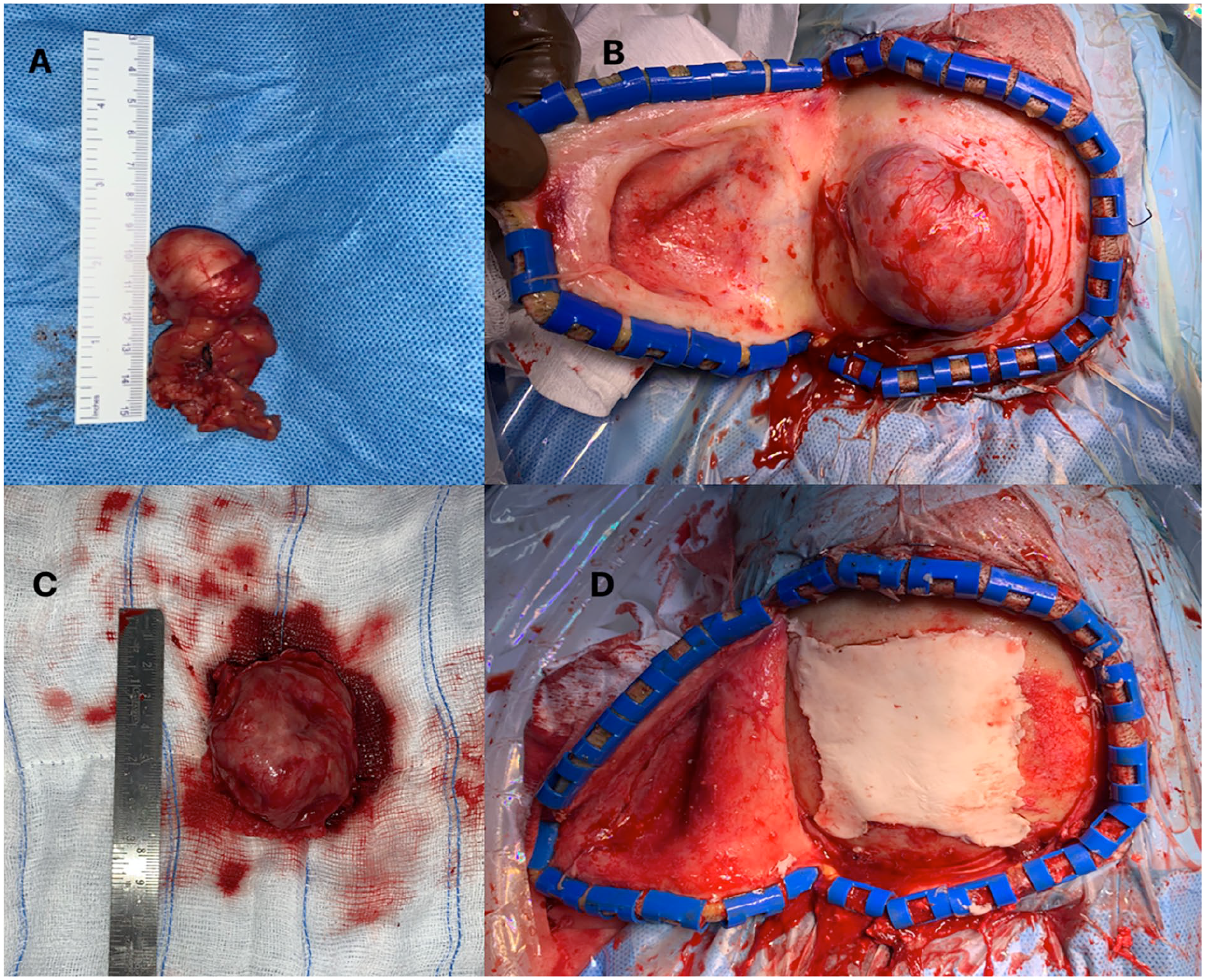
(A) Excised right submandibular gland showing a smooth yellowish tumor arising from the lower pole. (B) The operative photograph of the left skull lesion shows a firm tumor deposit fixed to the parietal bone. (C) Total gross excision of the skull lesion. (D) Cranioplasty using polymethyl methacrylate cement.
Postoperative Results
Surgical histopathology revealed a tumor composed of an admixture of epithelial, myoepithelial, and stromal elements (Figure 2A). The tumor was seen invading into the skull bone (Figure 2B). Immunohistochemistry was performed, which showed diffuse positivity for Glial fibrillary acidic protein (GFAP) (Figure 3A) and p63 (Figure 3B). The MIB1 proliferative index was approximately 5% to 15% (Figure 3C). Based on the histomorphology and immunohistochemistry, a diagnosis of MPA was made.
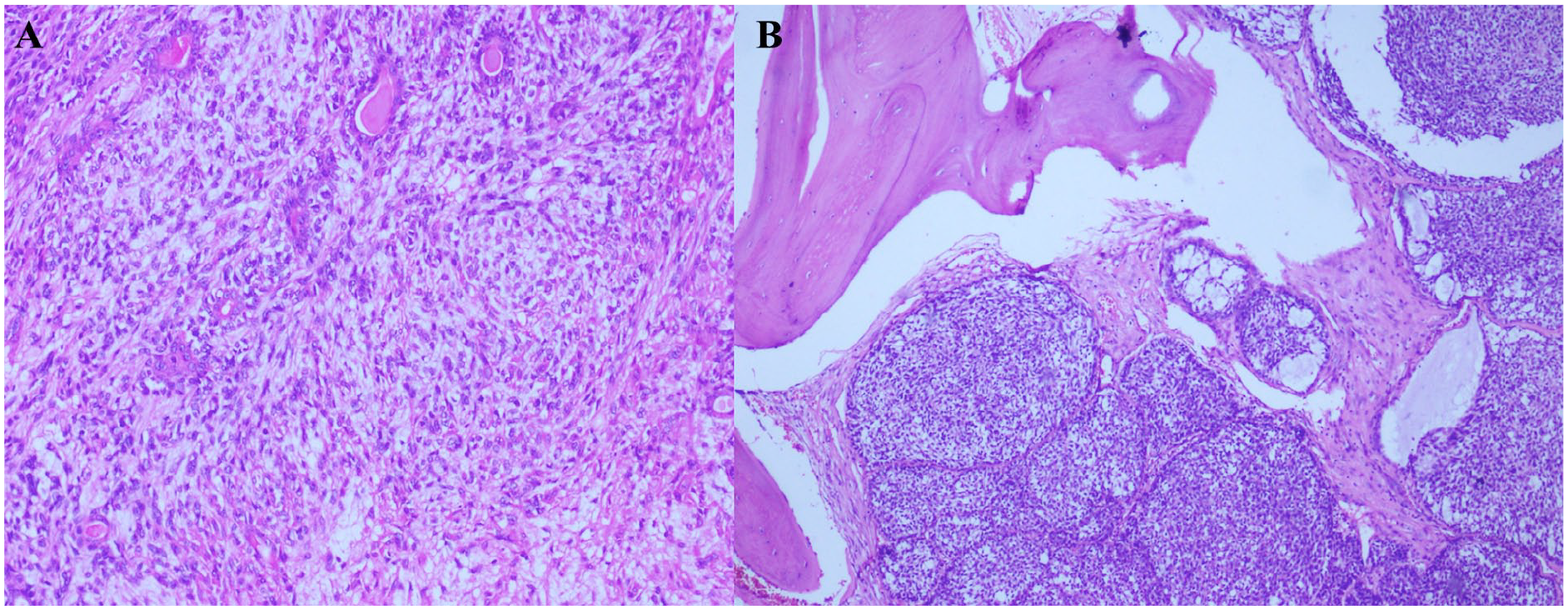
(A) Tumor arranged in sheets and tubules (H&E, original magnification ×20). (B) Bone invasion by the tumor (H&E, original magnification ×20).
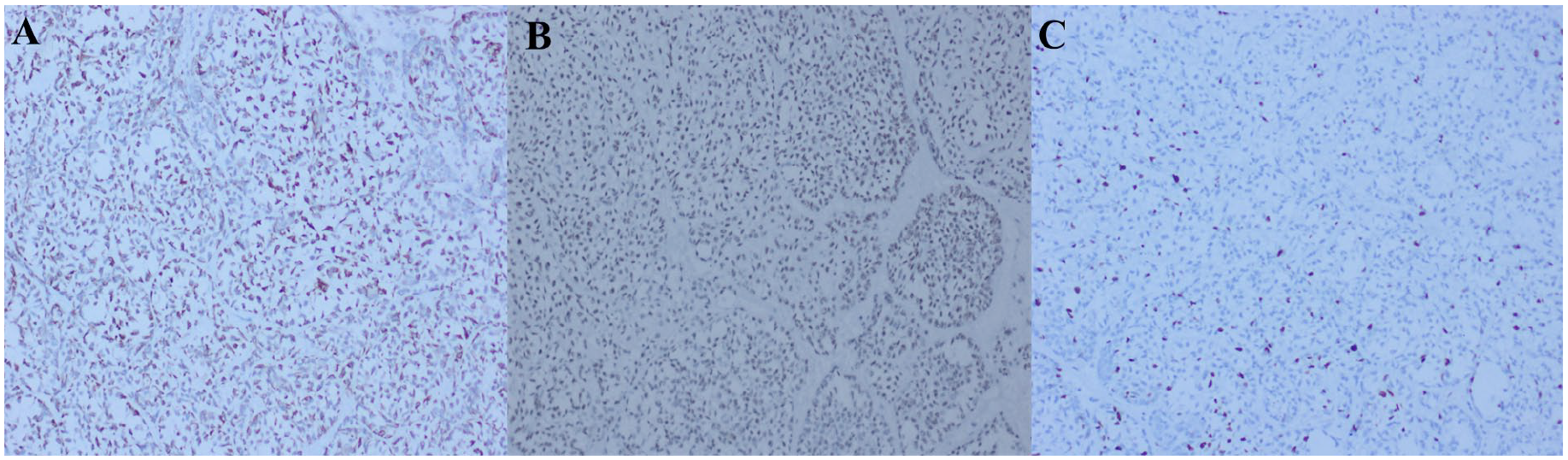
(A) Tumor cells diffusely positive for GFAP (IHC, original magnification ×20). (B) Tumor cells positive for p63 (IHC, original magnification ×20). (C) MIB1 proliferative index ~5% to 15% (IHC, original magnification ×20).
Discussion
The World Health Organization defines MPA as a “histologically benign pleomorphic adenoma that inexplicably manifests local or distant metastasis.” 6 The International Classification of Diseases for Oncology assigns this disease a behavioral code of /1, which corresponds to neoplasia of uncertain and unknown behavior.6,7 Most patients (81%) with MPA have a history of at least one local recurrence of pleomorphic adenoma prior to the detection of distant metastasis. 6 The time of appearance of the metastasis has been reported to be between 1.5 and 55 years after surgery.6,8 Almost 73% of the reported cases of MPA have a history of local recurrence, with 37% of them showing multiple relapses. 5
It is unclear whether the metastasis occurs due to surgical manipulation of the primary tumor causing permeation of blood vessels or lymphatic vessels by the tumor cells, followed by metastatic spread later on, or is due to any preexisting or de novo genetic variation in the tumor cells. 9 Moreover, MPA manifests as a benign disease even at metastatic sites. 10 It is believed that MPA can arise when enucleation of the pleomorphic adenoma is incomplete, during surgery, contributing to recurrence; vascular seeding of tumor cells can occur, favoring metastasis by the hematogenous route. 11 However, the seeding of blood or lymph vessels may not explain why metastasis occurs years after the initial presentation of the primary disease, and the relationship of genetic variations to metastasis is also unclear since the metastasis is microscopically identical to a benign PA, and it is currently not possible to histologically differentiate an MPA from a benign PA. Some have even suggested MPA to be a second primary disease arising in ectopic salivary tissue. Mariano et al. conducted a genomic hybridization investigation on MPAs. Analysis of the primary and secondary tumors showed the clonal origin of the secondary MPA, with a specific pattern of copy number alterations [copy number losses affecting 3p22.2p14.3 and 19p13.3p123], and a complex pattern of 4 different deletions at chromosome 6 in the primary tumor, suggesting an innate metastasizing characteristic. By contrast, the secondary MPA showed a more unbalanced genome [additional copy number changes affecting 9p24.3p13.1 (loss), 19q11q13.43 (gain), and 22q11.1q13.33 (gain)]. 12 Thus, the paradoxical nature of MPA, with its benign histological appearance and its capacity for metastatic spread, intrigues clinicians and researchers. 9
Conclusion
The malignant potential of a long-standing pleomorphic adenoma should not be ignored, so long-term surveillance should be maintained for such patients. The exact cause of the metastatic potential, whether it is a new genetic development or a preexisting one, remains enigmatic, and it is not proven that it occurs due to surgical manipulation of the primary tumor. Owing to its rarity, there has been little research on tumor biology, although various studies have analyzed molecular and genetic changes in this condition.
Footnotes
Author Contributions
P.V. wrote a draft of the manuscript and acquired the images. A.J.T. conceptualized the study, performed the salivary gland surgery, and supervised the writing of a draft of the manuscript. G.V.J. contributed to the content of the manuscript. V.S. did the pathological assessment and provided the histopathological images. E.J.G. supervised the work and performed the cranial surgery. All of the authors have read and approved the final manuscript.
Data Availability Statement
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Approval from the Institutional Review Board was obtained prior to the preparation of the manuscript.
Consent to Participate
Consent for participation in the study and publication of this report including relevant images was obtained from the patient.