
Abstract
Warthin tumor (WT) is the second most common benign tumor of the parotid gland with male predominance and is seen in the elderly population in the left mandibular and cervical regions. Extraparotid WT rarely presents as a mass in the right cervical region in middle-aged adults. Here, we present two extraordinary cases of WT seen in middle age, both in the right cervical region. The first is a 50-year-old man with an asymptomatic neck mass, and the second is a 60-year-old woman with a fast-growing mass with enhancement in positron emission tomography-computed tomography (PET-CT) with suspicions of malignancy.
Introduction
Warthin tumor (WT), or papillary cystadenoma lymphomatosum, is a benign neoplasm of the salivary glands, originally described by Hildebrand in 1895, but detailed identification in the literature was first made by Dr. Aldred Scott Warthin in 1929.
1
It is histologically characterized by a dense lymphoid matrix and a double layer of oncocytic epithelium with cystic properties and papillary projections.
2
Among all salivary gland tumors, WT is the second most common benign tumor of the parotid gland, and 3–17% of all parotid gland masses. 3 WT in the submandibular glands and cervical lymph nodes is rare, with percentages of .4–6.9% and 8%, respectively. 4 WT of minor salivary gland origin is extremely rare; the latest incidence is merely .1–1.2%. 4 Some literature also reports WT arising from the hard palate, lip, and oropharynx. 3
We present two cases of atypical presentations of WT in the minor salivary gland: the first resembling lymphadenitis and the second with suspicion of malignancy due to the enhancement of positron emission tomography-computed tomography (PET-CT).
Case Presentations
Case 1
A 50-year-old male patient was referred to the Otorhinolaryngology Department with a non-tender neck mass that remained for 3 months. His medical history revealed an allergy to penicillin and 40 years of smoking. During the physical examination, a 4 cm semisolid, mobile, and untender mass was palpated in the right middle cervical area. There were no other pathological findings.
A neck ultrasound (US) was performed at another hospital, revealing a 39 × 30 × 22 mm lymphadenopathy with cortical thickening in the right submandibular area. Bilateral parotid glands, submandibular glands, thyroid glands, and vascular structures presented normally.
He received 14 days of clarithromycin. After antibiotic treatment, a subsequent US was performed at the initial center, and the diameter did not show significant differences. The clinical diagnosis was undifferentiated lymphadenopathy. For further diagnosis and treatment, an excisional biopsy was planned.
Under general anesthesia, a 5 cm incision was made in the right submandibular region. After passing the cervical branch of the facial nerve medial to the submandibular gland, a heterogeneous vascular mass of 35 × 25 × 20 mm was observed. When trying to excise, the mass ruptured, revealing a pus-like fluid that was aspirated and sent to microbiology. Our initial suspicion was a possible abscess formation within the mass. The submandibular salivary gland was located normally and had no relationship to the tumor. The excised material was sent to pathology.
Histopathological examination revealed a WT originating in the right minor salivary gland. The immunohistochemical study resulted in CD3, CD20, CD30, Bcl-2, and focal positivity for Bcl-6 (Figure 1). The surgical margin was free of tumors, and there was no indication of malignancy. CD 3 dye showing T lymphocytes in tissue, at ×200. Both arrows point to the clusters of T lymphocytes in the lymphoid stroma.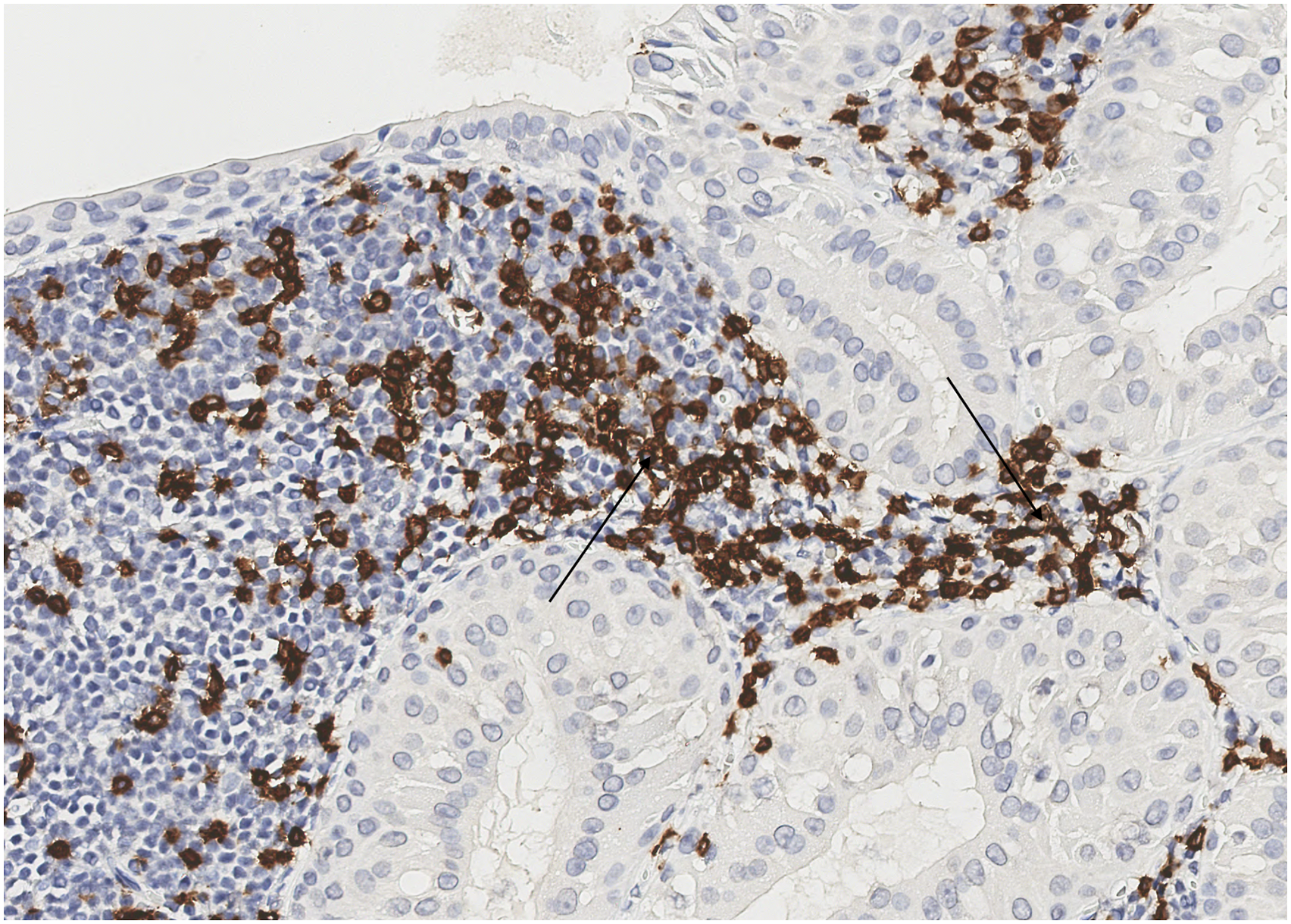
The results of aerobic, anaerobic, and tuberculosis cultures obtained from the liquid were negative. Microbiological examination showed lymphocytic cells, but this finding was not sufficient to diagnose abscess formation. Subsequently, the fluid was defined as a material rich in protein. No immediate or late complications were observed.
Case 2
A 60-year-old woman was referred to the Otorhinolaryngology Department by a pulmonologist. The patient had symptoms of cough and dyspnea. A subsequent SARS-Cov-2 polymerase chain reaction test was negative, and thorax CT revealed signs of pneumonia and a hypodense tubulonodular lesion in the superior segment of the lower lobe of the left lung. To further identify the lesion, a PET-CT was ordered, showing a fluorodeoxyglucose (FDG)-enhanced mass in the right cervical area with suspicion of malignancy, while the pulmonary lesion was free of enhancement (Figure 2). During the ear, nose, and throat (ENT) examination, the patient revealed that the cervical mass had persisted for 3 months but had gotten larger in the past week. Her medical history was significant for 30 pack years of cigarette smoking. A physical exam revealed a semi-hard, non-tender mobile mass in the right upper cervical area. The PET-CT scan of the second patient. There are 3 different sections of images that have been obtained. The first line is the axial cervical region; the white arrow points to the mass posterior to the mandibular bone. The second and third lines of images were obtained because the patient had cancer suspicion. The black arrow points to the mass on the right cervical area.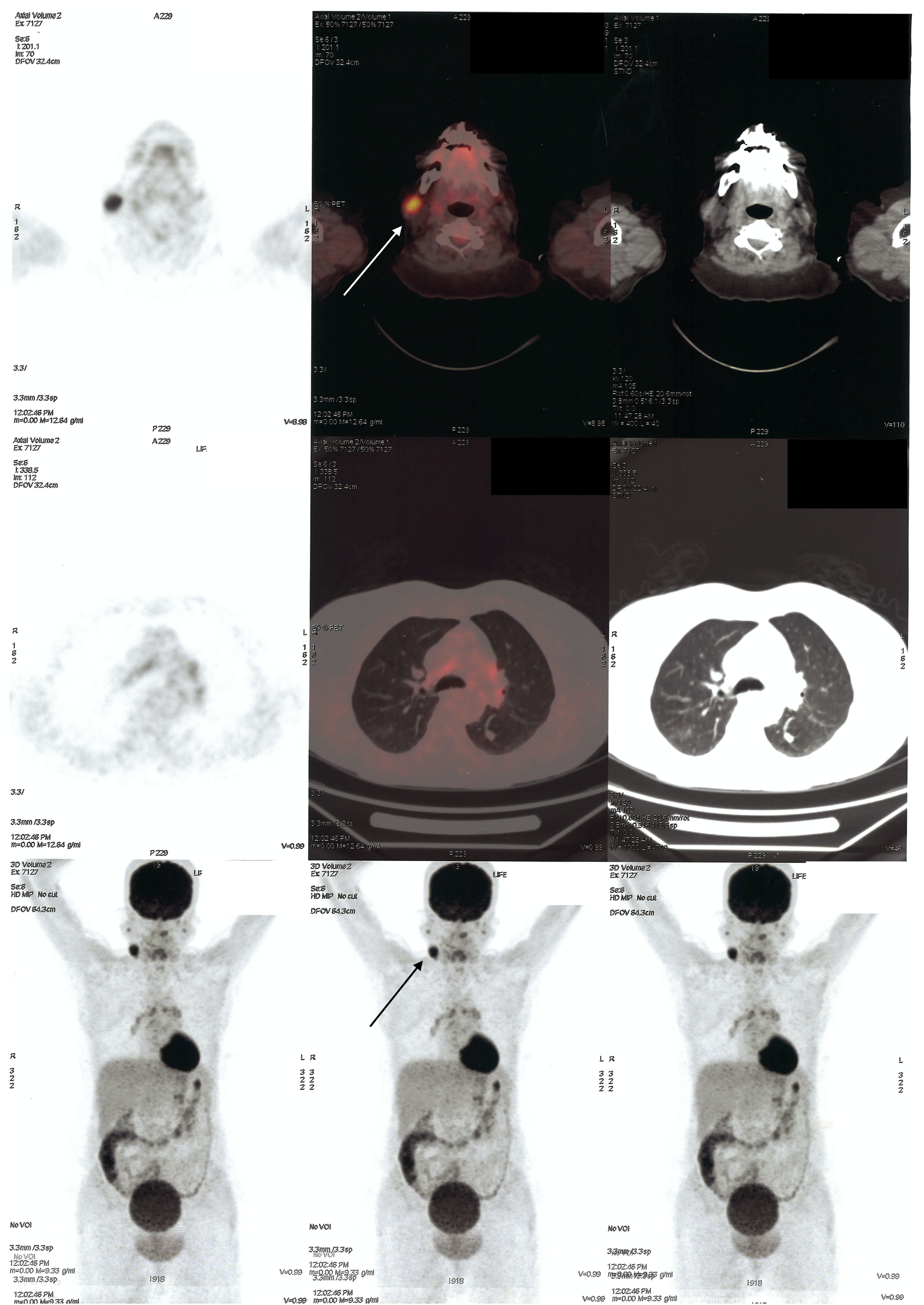
Ultrasonography was performed. At the right submandibular level, there was hypoechoic lymphadenopathy with an increased round index of 22 × 18 mm and an intense cortical blood supply. Lymph nodes with cortical thickening were also described at all levels of the neck. An excisional biopsy was planned for the FDG-enhanced lymph node at the right submandibular level. Under general anesthesia, a 4 cm incision was made in the right upper neck, and approximately 3.5 cm of lymphoid tissue was removed from the right jugular vein.
The material was sent for pathology and immunohistochemistry, revealing positivity in epithelial tissue and CD20 and PAX5 positivity in lymphoid follicles. CD23 PanCK revealed dendritic mash, and CD10 and bcl6 dyed the germinal center. The Ki67 proliferation index was high in the germinal center and 5–10% in other areas, which was suggestive of WT. The patient was discharged without complications, and further follow-up examinations were normal.
Discussion
WT, also known as lymphomatosum papillary cystadenoma, monomorphic adenoma, or adenolymphoma, is a benign tumor of the salivary glands. Most WTs are seen in the superficial lobes of the parotid glands and periparotid lymph nodes. 2 Extraparotid WT occurs in 2.7–12% of cases, most commonly in the cervical and periparotid regions. 5 WT is multicentric in 25% of patients and bilateral in up to 15%. 2
Patients most commonly present with an asymptomatic, slow-growing mass in the parotid gland, although there are cases of rapid growth and pain due to inflammation in the literature. 2 The symptoms of extraparotid WT can be masses in the cervical region and buccal mucosa, oropharyngeal fullness, and dysphagia.1,3 In our first case, the patient presented with an asymptomatic mass in the right cervical area, whereas in our second case, the patient presented with a rapidly growing cervical mass on the right side.
Although not yet fully explored, there are theories on the pathogenesis of WT. Autoimmune reactions and developmental abnormalities are the two main theories. There is also a focus on genetic background, although it has not yet been proven. 2
US, CT, magnetic resonance imaging, and Tc-99 scintigraphy are used in the differential diagnosis and imaging of WT, depending on the patient’s medical history. Fine needle biopsy (FNB) is one of the most commonly used techniques. Excisional biopsy was preferred over FNB in both cases due to the increased burden of invasive approaches in these patients, since if FNB had revealed a pathology, a subsequent excision would have to be performed, cost-ineffectiveness, and an increased risk of infections caused by the invasive nature of these procedures.
A definitive diagnosis is based on a pathological examination. WTs are benign masses capsulated with smooth or lobulated surfaces. They commonly contain mucoid brown fluid. Solid gray tissue encapsulates white nodules of lymphoid tissue.
2
Differential diagnosis is easy due to its distinctive properties, papillary formation, and prominent lymphoid content (Figure 3).
2
Treatment is the excision of the tumor. H&E x4 magnification. An encapsulated tumor composed of cystic spaces and polypoid projections. The black arrow shows polypoid projections, and the white arrow points to the cystic space.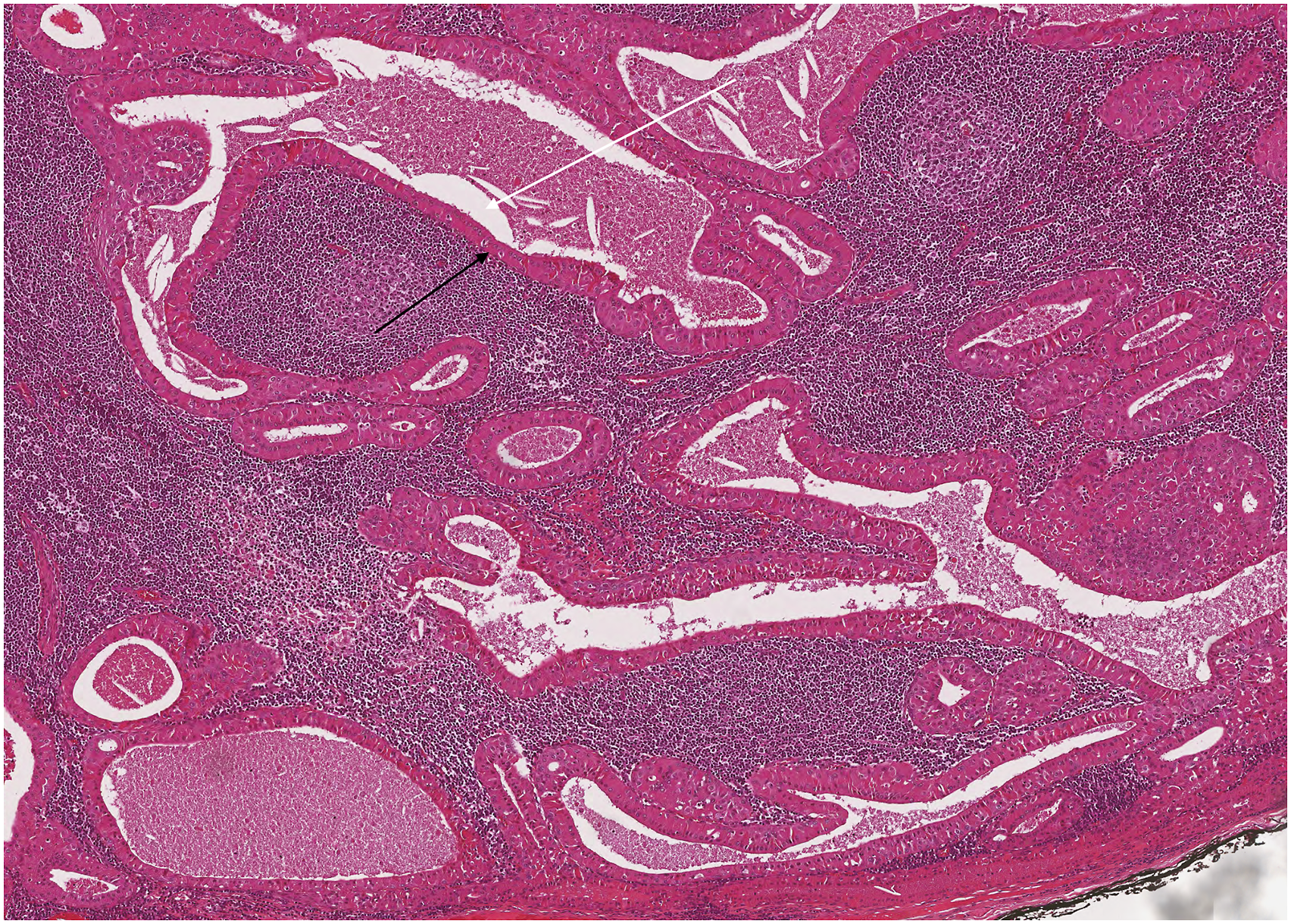
Recurrence of these tumors after complete excision is unexpected, although some cases have been reported. Although we do not have enough evidence, some tumors are believed to be synchronously multicentric.1,6
Conclusion
In the literature, WT is seen primarily in the parotid gland and is rarely present in the cervical area, which resembles lymphadenopathy. This report aims to draw attention to the locational and presentational varieties of WT. WT should be included in the differential diagnosis of neck masses as possible benign tumors. It should not be considered exclusive to the parotid gland or salivary glands but also lymph nodes. This knowledge can be useful for physicians as they choose the appropriate and cost-effective treatment for their patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Separate informed consent was obtained from both patients.