
Abstract
Objectives:
The transoral approach for parapharyngeal space tumors has been criticized due to its restrictive exposure and increased rate of vascular and nerve injuries. However, for certain tumors—namely those that are prestyloid, benign, and well-encapsulated—the transoral approach reduces overall morbidity while providing direct access. Transoral surgeons can rely on this approach for select tumors seen clearly on intraoral examination in the bulging lateral pharynx. In this article and with a supplemental operative technique video, we demonstrate our transoral approach in these select patients.
Methods:
We reviewed our 26 cases using this approach and chose a representative case of a 50-year-old man who presented with a large, prestyloid, encapsulated parapharyngeal mass affecting his voice and swallowing. A transoral approach to the parapharyngeal tumor is illustrated.
Results:
A vertical curvilinear incision is completed from the hamulus to below the inferior extent of the tumor. Blunt dissection of the tumor capsule proceeds inferiorly. Controlled violation of the tumor capsule can aid in visualization. After tumor delivery, the wound is irrigated and closed.
Conclusions:
In our experience, the transoral approach is an effective method to access well-encapsulated, prestyloid parapharyngeal space tumors. Patient selection is important when considering a transoral approach.
Keywords
Introduction
Multiple surgical approaches to the parapharyngeal space (PPS) have been described for PPS tumor resection. The choice of surgical approach is dependent on tumor size, location, and proximity to important neurovascular structures. Of the varying surgical approaches, the transoral approach has been the most criticized when compared to the well-established transcervical approach. This has been attributed to inadequate exposure leading to reportedly increased rates of major vessel and nerve injuries when compared to the transcervical approach. 1
However, limited studies suggest that the transoral approach is an effective and adequate method for the resection of certain PPS tumors, namely prestyloid, small, benign parapharyngeal tumors.2,3 At our institution, we have found this to be true and have been using a transoral approach for selected well encapsulated PPS tumors with minimal complications. In this study, we describe our preferred transoral technique in the resection of parapharyngeal tumors.
Methods
A survey of all patients undergoing a transoral approach to parapharyngeal tumors between 2008 and 2019 at our institution was performed. Twenty-six patients were found who had this approach to address a parapharyngeal tumor. The patient featured in our video presentation is a 50-year-old gentleman who presented with a 5-year history of a right parapharyngeal mass which was affecting his voice and swallowing. On computed tomography imaging, this was noted to be a large 4.2 × 4.4 × 7.6 cm, ovaloid, prestyloid, well-defined (encapsulated), heterogenous mass with several cystic and necrotic foci and resultant leftward deviation of the pharynx. The mass was obvious on intraoral examination with a normal appearing tonsil medialized over the midline. Intraoral palpation revealed a firm, semimobile mass in the anterior–posterior plane. The mass was not palpable in the neck or behind the angle of the mandible. The patient was counseled on the different approaches to the tumor and a transoral approach was chosen due to the tumor’s location and radiographic appearance.
Results
Operative Technique
After initiation of general anesthesia and contralateral nasal intubation, a Crow-Davis straight blade retractor and lip protector are placed. Gentle neck extension allows for optimal surgical ergonomics. Special care is given to protect and cover the eyes. The tumor and surrounding soft tissues are inspected and palpated to ensure adequate exposure (see Figure 1). Local anesthesia with 1% lidocaine with 1:100 000 epinephrine is infiltrated around the lesion. A vertical curvilinear incision is completed from the hamulus to below the inferior extent of the tumor with an extended protected tip Bovie (see Figure 2). Mucosa and submucosa are divided to the tumor capsule lateral to the anterior tonsillar pillar. This incision is most helpful when placed over the maximal convexity of the tumor capsule; caution should be taken to leave a healthy mucosal cuff on the anterior pillar to help with closure and lateralization of the preserved tonsil.

The transoral tumor and surrounding soft tissue is inspected and palpated with a Kittner sponge on a tonsil clamp seen on the right. Adequate exposure of the intraoral lesion is attained with a Crow-Davis straight blade retractor and lip protector.
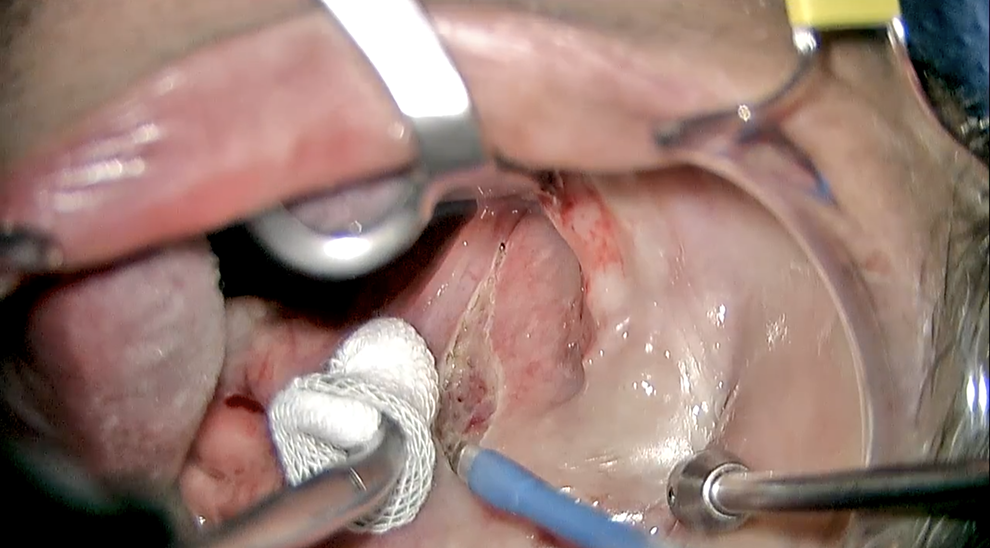
A curvilinear incision is being made through the mucosa and submucosa with an extended tip Bovie. Gentle medial traction is seen with a Kittner sponge on a tonsil clamp on the left. The metal pediatric Yankauer suction tip, seen on the right is aiding with dissection by providing lateral traction and maintaining a clear operative site.
The constrictor muscle over the tumor is split and blunt dissection commences on the tumor capsule at the superior aspect of the mass and proceeded inferiorly, working medially and laterally. Dissection is always carried out from areas where visualization, tissue mobilization, and retraction is easiest and works toward more limited areas. Dissection becomes easier as the tumor becomes more mobile. This dissection is done using a combination of instruments—Kittner sponge dissectors on tonsil clamps, pediatric Yankauer suction (small metal), Herd retractor, DeBakey forceps (long), long suction freers, pledgets, a long straight bipolar, and blunt finger dissection—which slowly and methodically exposes and releases the tumor from its loose attachments within the PPS. We have found that the back end of the DeBakey forceps is helpful as a pushing retractor in the primary surgeon’s hand while dissecting with the bipolar in the other hand. Pushing capsular blunt dissection is ideal with frequent use of the bipolar, similar to its use in the delivery of a substernal goiter or capsular dissection of a parotid tumor (see Figure 3). The pediatric Yankauer is also very helpful as a pushing suction retractor.
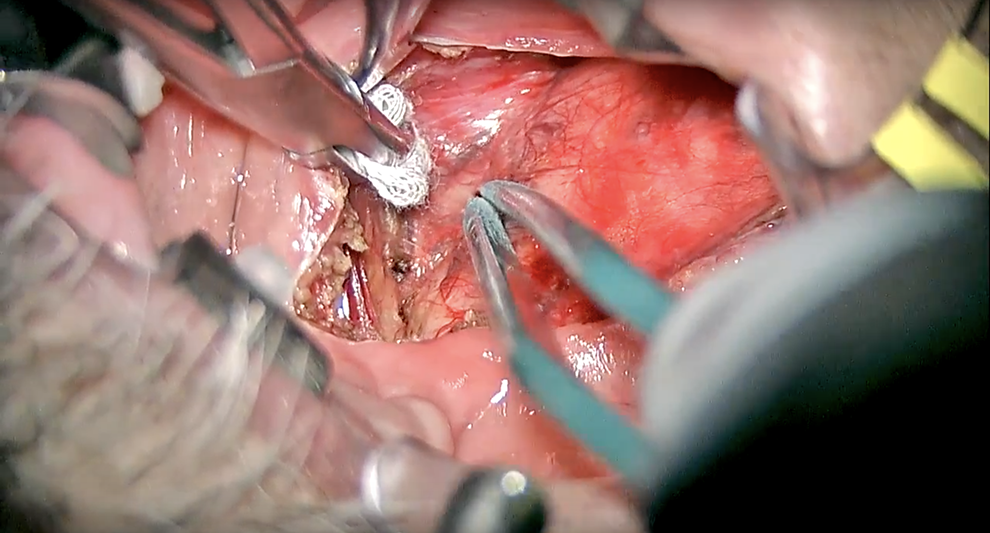
The long straight bipolar is seen maintaining hemostasis as it simultaneously frees the tumor from loose connections to the surrounding soft tissue of the parapharyngeal space. The Kittner sponge on a tonsil clamp is pushing normal adjacent tissue superiorly as the long straight bipolar is bluntly dissecting the tumor inferiorly.
The goal is complete tumor mobility while preserving the normal adjacent tissues. Progressive quadrant dissection, with only targeted retraction, helps with visualization. In oozing areas and areas of difficult dissection, packing the area with ½ × ½ or ½ × 3 cm neuro sponges soaked in oxymetazoline or topical epinephrine can aide in visualization. Finger dissection with finger delivery is often required of larger tumors (see Figure 4). Importantly, as larger tumor sizes, limited incision sizes, and visualization hindrances make dissection and delivery difficult, we find it occasionally helpful to perform a controlled violation of the already dissected most anterior portion of the capsule and remove up to 50% of the tumor volume intracapsularly after which we close the capsule and proceed with repeated quadrant dissection. This process can be repeated for large tumors until complete mobilization and delivery is possible. We have found this technique especially helpful for very large tumors. It can aide in prevention of an uncontrolled capsular rupture posteriorly, or in areas where you cannot directly see, from the pressure of retraction, dissection, and finger delivery of the tumor. This aide can also help when the surgeon feels that the retraction or blunt dissection is too forceful on the tumor capsule, putting it at risk of an uncontrolled capsular rupture on the deep margin where tumor spillage will occur in an uncontrolled fashion until the tumor is delivered.
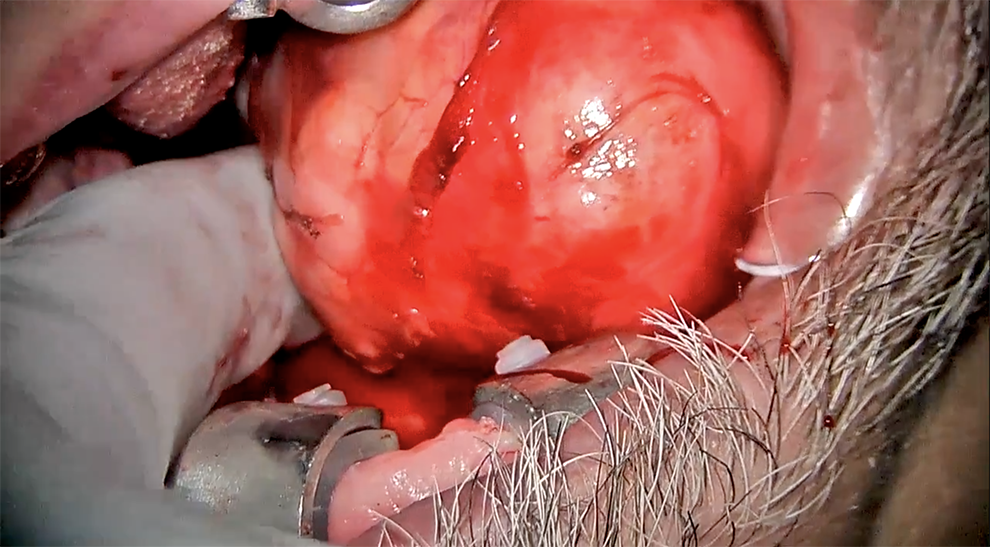
Seen on the medial edge of the tumor, finger dissection is being used to mobilize and free the tumor from surrounding soft tissue. Finger palpation is simultaneously being used to detect areas of tumor adherence and tethering to the surrounding soft tissue.
The deep aspect (posterior and lateral-posterior along the parotid margin) is dissected last, allowing complete tumor delivery. The wound is irrigated, examined, and hemostasis is maintained with bipolar. The wound is closed in layers using interrupted absorbable sutures—preferred mucosal sutures are 2-0 or 3-0 braided polyglycolic acid sutures.
Discussion
The PPS is classically described as an inverted pyramid, bounded superiorly by the skull base, inferiorly by the superior cornu of the hyoid bone, anteriorly by the pterygomandibular raphe, posteriorly by the cervical vertebrae and paravertebral muscles, medially by the oropharynx and nasopharynx, and laterally by the mandible ramus and the deep lobe of the parotid gland.4,5 Within this anatomically complex space, tumors are referenced by their relation to the styloid process. Prestyloid compartment tumors are more common and tend to be pleomorphic adenomas or other salivary gland tumors while poststyloid compartment tumors typically are neurogenic tumors such as schwannomas, paragangliomas, and neurofibromas.6,7 Of these tumors, approximately, 80% are typically benign. 8
Parapharyngeal space tumors are often difficult tumors to resect due to their deep location in the neck as well as their proximity to vital neurovascular structures. These tumors have been historically resected using a transcervical approach. However, due to a better understanding of cervical anatomy and advances in imaging, 6 main surgical approach have been described—the transcervical, cervicoparotid, mandibular split, transcervical–transmastoid, infratemporal fossa, and transoral approaches. 9
Traditionally, the transcervical approach has been described as being best for tumors with limited mobility and submandibular extension, such as those residing in the prestyloid compartment and tumors originating from the deep lobe of the parotid gland.6,10 Conversely, limitations to this approach include poor access to the medial and superior aspects of the PPSs, severely limiting access to the skull base portion of the PPS. 9
The transoral approach addresses some of the constraints of the external approach. The transoral approach is preferred for tumors with superomedial extension toward the skull base and should be considered for tumors that occupy the prestyloid compartment medial to the great vessels. Other authors have suggested restricted exposure dictating smaller, avascular, and benign tumors as ideal candidates where margin control is not paramount. In the literature, the largest study using the transoral approach had a mean tumor volume of 133.2 cm3 and size of 6.1 cm. 11 In our experience, tumors size is not as important as the tumors capsular margin and mobility, and most can be safely removed with a transoral approach with certain technical modifications such as blunt pushing dissection and consideration of controlled intracapsular volume depletion. Ideally, the transoral candidate should have a wide mouth opening with a low Mallampati score in addition to adequate neck extension. The tumor should be well visualized intraorally, medializing the tonsil, and easily palpated above the inferior border of the mandible. Most oropharynx transoral surgeons will be confidently familiar with removing tumors that lie above the submandibular gland from this transoral approach as the visualization and equipment is similar to what would be used in a radical tonsillectomy.
We have found this approach more teachable and reproducible than the described robotic technique for the PPS tumors which we find more expensive, time consuming, and harder to manipulate and retract tumors as larger volume tumors are encountered. We understand that the availability of a robot is largely institution dependent as its use is not without significant costs. In a study done by Weinstein et al, cost effectiveness of utilizing the da Vinci Surgical System (Intuitive Surgical Inc, Sunnyvale, California) for transoral robotic surgery (TORS) is justified only when other surgical specialties such as Urology, General Surgery, Cardiac Surgery, and Gynecology utilize the robot. Profitability is generated by surgical volume; therefore, TORS alone cannot outweigh the costs of robotic disposables. 12 With cost efficiency playing a major role in medical practice, robotic surgery comes with financial disadvantages. Additionally, the success and efficacy of robotic surgery is operator-dependent and obviates a required experienced robotic surgeon. 13 In contrast, traditional surgical resection of PPS tumors is commonplace in virtually all head and neck practice. General indications and contraindications of TORS proposed by O’Malley et al for PPS tumors are considerably similar to what we propose for our transoral approach previously described. One difference is that a poststyloid tumor was not considered a contraindication for a TORS procedure. 14 We propose that transoral resection of certain PPS tumors in select patients does not necessitate the use of a robot due to the aforementioned constraints. In our experience, transoral laser or robotic surgeons will see a benefit to transitioning PPS tumor resection, especially with larger tumor sizes, to transoral nonrobotic approaches using techniques and instrumentation more similar to a conventional radical tonsillectomy and specifically employing pushing capsular dissection and controlled anterior capsular incision with intracapsular debulking.
In the right patient, the transoral approach allows for a more direct route to the tumor, reduced dissection of surrounding tissues, and leaves no external scar.15,16 As the overall trend in surgery moves toward minimally invasive techniques, minimally invasive approaches are becoming more favored as they have been shown to decrease hospitalization length, blood loss, and postoperative pain. 1
Suggested limitations of the transoral approach include poor illumination and maneuverability of instruments in the surgical field, facial nerve injuries—most often to branches adjacent to the deep lobe of the parotid gland—in addition to carotid sheath injuries, poor hemostatic control in the event of hemorrhage, and direct contact with oral flora1,6 Decreased visibility and maneuverability have also been associated with an increased probability of capsular disruption with possible tumor spillage, recurrence of tumor, and the possibility of neurovascular damage.
Interestingly, there have been no reported complications of unintentional vascular damage during transoral dissection. Ducic et al establish that visualization and control of the internal carotid artery is adequately obtained in the transoral approach 17 ; this has been our experience as well, including several cases of poststyloid tumor removal, where the internal carotid was mobilized off of the tumor anteriorly with relative ease due to the robust capsule that these tumors usually possess.
Reported nerve injuries during transoral dissection has been noted to be expected as those tumors resected were vagal schwannomas. 17 In a study by Chen et al, 1 inadvertent facial nerve injury was found within a cohort of 12 transcervical parapharyngeal tumor excisions; the transoral approach was suggested to be beneficial secondary to its avoidance of the marginal mandibular, facial, and inferior alveolar nerves. 18
The transoral approach has also been thought to be associated with an increased chance of tumor spillage and recurrence. In one of the first studies assessing the efficacy of the transoral approach in 1988, Goodwin and Chandler reported a 25% recurrence rate of transorally resected pleomorphic adenoma tumors after 5-year follow-up. 19 However, Betka et al reported no recurrences in 26 transorally resected benign tumors—most of which were pleomorphic adenomas—after 6-year follow up, despite 2 cases of pseudocapsular rupture. 11 The authors describe nearly nonexistent complications when preoperative evaluation excluded tumor malignancy, hypervascular tumors, dumbbell-shaped tumors, poorly demarcated tumors, and tumors in close proximity with major neck vessels from approaching the mass transorally.11,20 This reiterates the need for proper patient and tumor selection when considering a transoral approach. As we described in the techniques portion, our approach for larger tumors—when it is felt that an uncontrolled rupture may occur—involves purposefully incising the already dissected anterior-most tumor edge and decompressing the intracapsular volume, sewing the capsule back together, and continuing the dissection. Uncontrolled rupture, we feel, is the most significant, often preventable, complication of this technique.
Conclusions
In a carefully selected patient with a parapharyngeal tumor, the transoral approach can be a powerful way within the head and neck surgeon’s armament to access prestyloid tumors with overall decreased morbidity, a shorter surgical and hospitalization course, good functional outcomes, and avoidance of an external scar.
Footnotes
Authors’ Note
Material has not been published previously.
Author Contributions
All authors contributed substantially and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.