
Abstract
Squamous cell carcinoma is the most common pathological type of external and middle ear malignancy. Squamous cell carcinoma of the external auditory canal and middle ear is closely associated with long-term chronic inflammatory irritation. The patient was admitted with a major complaint of a “stuffy feeling in the left ear for more than three months.” The results of the otoendoscopic examination were as follows: The left external auditory canal was filled with a granuloma-shaped mass with an unsmooth surface that showed obvious oozing of blood. The tympanic membrane was not visible. After the completion of the relevant examinations, radiofrequency resection of the external auditory canal mass was performed under otoendoscopy and the wound healed well with postoperative dressing changes. Pathological results revealed a well-differentiated keratinizing cutaneous squamous cell carcinoma and there was no recurrence throughout the next 5 years after the operation. Proper preoperative evaluation and the correct selection of surgical approaches can be of great importance. The primary complication of ear squamous cell carcinoma was local recurrence with a low incidence of metastasis. Early and complete resection was determined to be the optimal course of treatment.
Introduction
External and middle ear malignancies are easily neglected in clinical practice due to their low incidence. Squamous cell carcinoma is the most common pathological type of malignant tumor of the external and middle ear. 1 The primary complication of ear squamous cell carcinoma is local recurrence with a low incidence of metastasis. An early and complete resection is the optimal surgery to perform. Low-temperature radiofrequency under otoendoscopy is a minimally invasive procedure that was first used in 1967 by Mer et al 2 for otologic examinations and diagnoses. In the past decade, with the continuous advancement of otoendoscopic instruments and equipment, limitations have gradually decreased, and advantages have been maximized and applied. In recent years, low temperature plasma radiofrequency ablation has been widely used in otolaryngologic, head, and neck surgery, and it is believed that surgical application of this new technology has reduced the duration of the operation, reduced postoperative bleeding, and alleviated the postoperative pain of patients. 3
Case report
General characteristics
A 75-year-old male patient was admitted to the Department of Otolaryngology at the Fifth People’s Hospital of Ningxia. The patient complained of a “stuffy feeling in the left ear for more than 3 months,” accompanied by significant hearing loss, an earache, and intermittent ear discharge. The patient had visited our outpatient clinic 1 week prior. The results of the otoendoscopic examination revealed a mass in the left external auditory canal and an external otitis. The patient was hospitalized after receiving anti-inflammatory therapy. The results of the otoendoscopic examination were as follows: The left external auditory canal was filled with a granuloma-like mass with an unsmooth surface that showed obvious oozing blood; additionally, the tympanic membrane was not visible. The patient was healthy and had no history of chronic disease. Since the onset of this condition, the patient's consciousness, diet, urine, and stool had been normal, and there was no obvious change in body weight.
Physical examinations
A temperature of 35.5°C, a pulse rate of 74 beats/min, a respiration rate of 20 breaths/min, and a blood pressure of 146/82 mmHg were recorded. The patient seemed to have a clear conscience. The superficial lymph nodes were not palpable and there was no cyanosis in his mouth and lips. The respiratory movement was normal and the lungs were clear without any moist rales or rhonchi. The border of the heart was normal and the heart rate was 74 beats/min. The cardiac rhythm was regular, with no pathological murmurs. The abdomen was soft, without tenderness or rebound tenderness. The liver and spleen were intact. The special examination findings included the following: the bilateral auricles were symmetric and without deformity, redness, and tenderness. The left external auditory canal was filled with a granuloma-like mass with an unsmooth surface that showed obvious oozing blood. The tympanic membrane was not visible.
Auxiliary examinations
(1) The results of the temporal bone computed tomography (CT) were as follows: the left external auditory canal was poorly patent and a hyperdensity strip was visible inside, the inner side of which was poorly demarcated from the tympanic membrane. The plain CT value was 80 HU. The peripheral bone structure was normal. The alignment and morphology of the right external auditory canal were normal. The bilateral tympanic cavities of the inner ear were symmetric without obvious abnormal density. There was no obvious abnormality in the structure of each auditory ossicle, with no significant enlargement of the opening of the mastoid antrum and good gasification of the mastoid. There were no significant abnormalities in the bony structures of the bilateral facial nerve canal or the cochlea, vestibule, and semicircular canals. The bilateral internal auditory canal was symmetric, with no significant widening or narrowing, and there was no enlargement or disruption of the bilateral jugular foramen. (2) The results of chest CT were the following: bilateral increase in lung markings was present, with a nodule in the lower right lung and calcification in the lower left lung. Bilateral pleural thickening and slightly enlarged mediastinal lymph nodes were observed. (No special treatment was required after consultation with the respiratory department and a regular review was recommended). (3) Detection of the pure tone hearing threshold showed the following results: there was mixed deafness in the left ear, with air conduction hearing levels of 85, 105, and 110 dB at 500, 1,000, and 2,000 Hz, respectively. There was sensorineural deafness in the right ear, with air-conduction hearing levels of 60, 65, and 85 dB at 500, 1,000, and 2,000 Hz, respectively. There was a significant decrease in high frequencies.
Pathological results
A well differentiated keratinizing cutaneous squamous cell carcinoma was discovered in the left external auditory canal.
Diagnosis and treatment
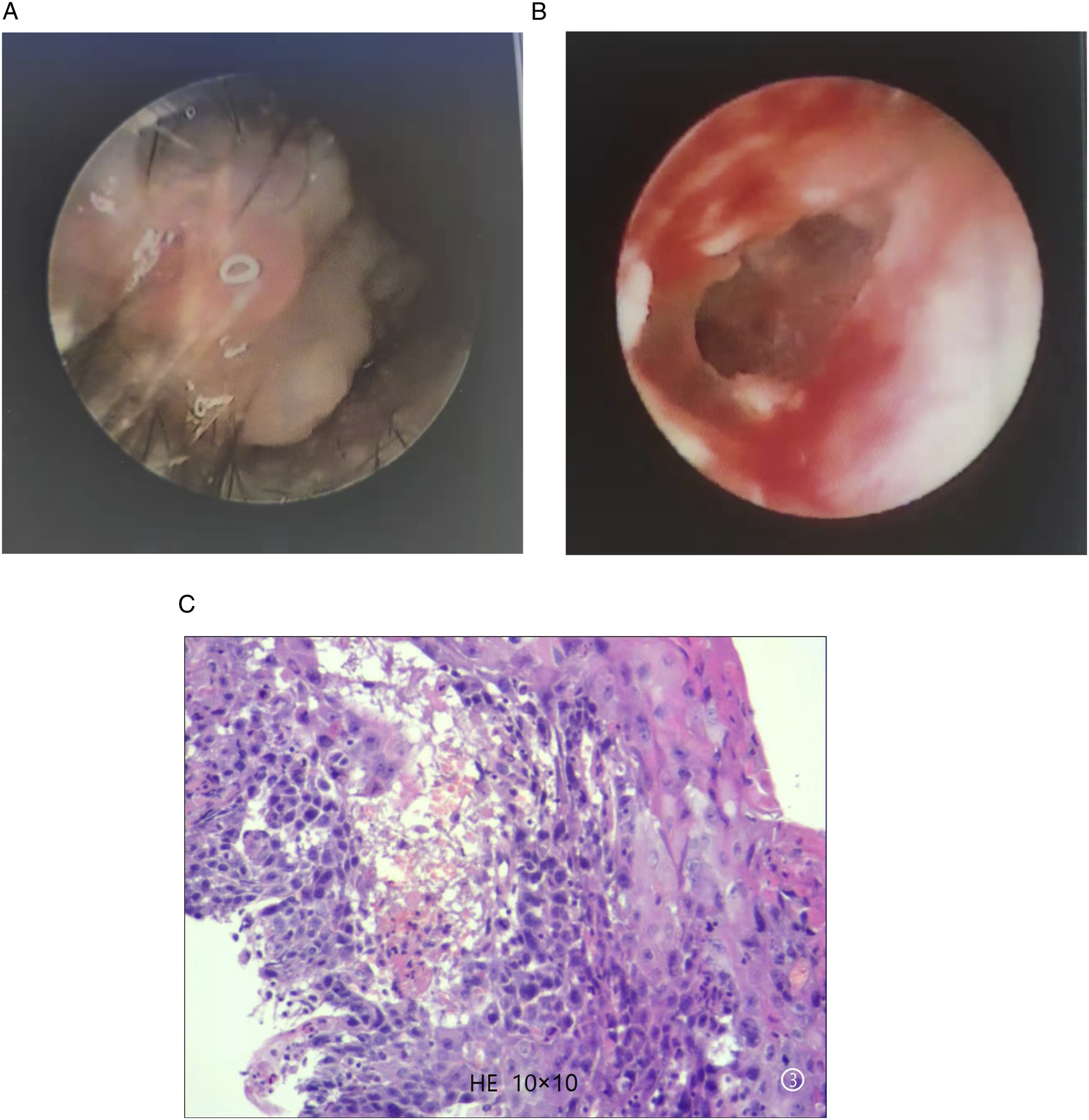
The preliminary diagnosis was a tumor of the left external auditory canal of unknown nature and the definitive diagnosis was squamous cell carcinoma of the left external auditory canal. After completion of the relevant preoperative examinations, a low temperature radiofrequency resection of the external auditory canal mass was performed under otoendoscopy and general anesthesia. The host machine adopted the BM780- integrated radiofrequency therapy instrument (German Sutter), the instrument’s special radiofrequency needle length was about 6 cm, the radiofrequency location was about 3-6 mm, ablation and cutting could be performed, according to operation needs, choosing the corresponding ablation or cutting mode with ear endoscope (diameter 2-3 mm, length 9-11 cm), see Figure 1. The left external auditory canal was filled with a granuloma-like mass (Figure 2A). Some of the tumors were sampled and then sent for pathological examination. The low-temperature radiofrequency machine was set to the coagulation mode, with a cutting power of 2.5. A low temperature radiofrequency needle was adopted to cut and ablate the gap between the mass and the external auditory canal. The granuloma-like tumor in the external auditory canal was excised in turn from the outside to the inside, and the base of the tumor was ablated. In case of obvious bleeding, a small cotton ball stained with epinephrine was used in the area for homeostasis before resection. During the operation, the tumor was observed on the bottom, anterior, posterior, and top wall of the external auditory canal. There was superficial erosion on the bony wall of the external auditory canal. A cerumen obstruction was visible deep in the external auditory canal, near the tympanic membrane. A large perforation of the tympanic membrane was visible after rinsing with normal saline, with a residual tympanic annulus. Hyperemia and edema of the tympanic mucosa were observed and the auditory ossicles disappeared (Figure 2B). The suspected mass was thoroughly resected and, after satisfactory hemostasis, an expanding sponge was adopted to fill the wound in the external auditory canal. The resected mass was then sent for pathological examination (Figure 2C). (A) The host machine. (B) Radiofrequency needle. (C) Ear endoscope. (A) The left external auditory canal in the patient was filled with a granuloma-like mass. (B) Large tympanic membrane perforation with residual tympanic annulus was visible after tumor resection during the operation. There existed hyperemia and edema of the tympanic mucosa and disappearance of auditory ossicles. (C) The pathological results of the mass in the left external auditory canal in the patient: A keratinizing cutaneous well-differentiated squamous cell carcinoma.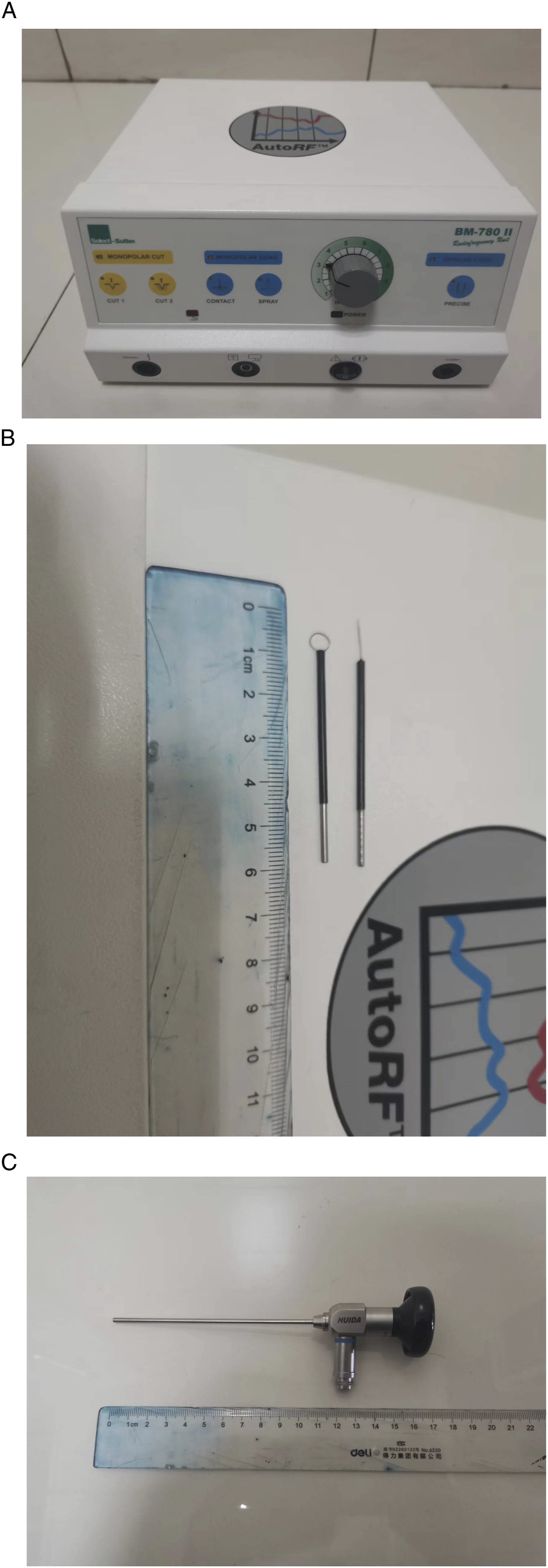
Anti-inflammation therapy was performed postoperatively and the expanding sponge was removed on the 2nd day. The results of the otoendoscopy were as follows: the surgical wound was slightly congested, without obvious edema, and the external auditory canal was unobstructed. There was a large perforation of the tympanic membrane with a residual tympanic annulus and hyperemia and edema of the tympanic mucosa. Furthermore, a disappearance of the auditory ossicles had occurred. The external auditory canal was disinfected with an iodophor cotton swab, and a urinary catheter for children was smeared with tobramycin/dimethylasone eye drops and placed in the left external auditory canal for support. On the 6th day after the operation, the external auditory canal support catheter was removed. The skin of the external auditory canal was found to have healed well and there was no obvious redness and swelling, so the patient was discharged after cleaning and dressing changes had been performed. The results of the pathological biopsy in a higher level hospital (The Affiliated Hospital of the Ningxia Medical College) were consistent with those of our hospital. After a consultation with ear specialists from the aforementioned hospital, it was recommended that observation, treatment, and review be conducted regularly. There was no extended postoperative excision and radiotherapy and no recurrence in the following 5 years after the operation.
Discussion
External and middle ear malignancies are easily neglected in clinical practice due to their low incidence. External and middle ear malignancies have been reported to account for 0.7% to 1.5% of malignant tumors in the head and neck, with an annual incidence of one in one million. The vast majority of patients with malignant tumors of the external auditory canal are between the ages of 50 and 60 and comprise more women than men. Squamous cell carcinoma is the most common pathological type of external and middle ear malignancies 1 and is closely associated with long-term chronic inflammatory irritation. 4 Squamous cell carcinoma can infiltrate the surrounding skin and adjacent tissues, as well as distant metastases. It may be accompanied by perineural invasion, and direct intracranial spread along nerve fibers is possible. 5 The primary symptom of external auditory canal malignancy is swelling in the ear canal, which can present as a nodular or granulomatous type. Patients with nodular type generally do not have otorrhea, while those with granulomatous type often have ear bleeding or pus and bloody discharge. Patients may have otalgia, conductive deafness, and facial palsy in advanced stages of invasion of the middle ear. Lymph node metastases are more common in the deep part of the upper neck, the parotid region, and the retroauricular lymph nodes. A clinical examination may reveal a brittle granulation or neoplasm that is easy to bleed in the external auditory canal, and a diagnosis can generally be confirmed by biopsy. Magnetic resonance imaging and computed tomography can determine the location and extent of invasion and damage from a tumor. Cancer in the external auditory canal is difficult to discover early. Otalgia is the primary symptom of this cancer and initially presents as intermittent dull or tingling pain that gradually turns into persistent severe pain that radiates to the ipsilateral temporal, neck, and shoulder areas. Pain is caused by an easy invasion of the nerves, which is also an early symptom of recurrence. Adenoid cystic carcinoma and squamous epithelial carcinoma of the external auditory canal have been reported to be characterized by neurophilic growth, 6 which may be related to early pain in external auditory canal cancer.
Low-temperature radiofrequency under otoendoscopy is a minimally invasive procedure that was first used in 1967 by Mer et al 2 for otologic examinations and diagnoses. In the past decade, with the continuous advancement of otoendoscopic instruments and equipment, limitations have gradually decreased, and advantages have been maximized and applied. Otoendoscopic surgery is a simple, efficient and safe procedure for otologists to perform, and the treatment process is minimally invasive and comfortable for patients, offering faster recovery. Measures should be taken to prevent an iatrogenic injury that could be caused by an operation under otoendoscopy. The light source of the otoendoscopy is prone to thermal damage 7 ; therefore, appropriate dimming of the brightness (no more than 50%), avoiding prolonged operation in a particular area, and using suction for rapid cooling should be adopted. Additionally, lens antifoggants that may be ototoxic should be avoided. 8
In recent years, low-temperature plasma radiofrequency ablation has been widely utilized in otolaryngologic, head, and neck surgery, and it is believed that the surgical application of this new technology has reduced the duration of the operation, reduced postoperative hemorrhage, and alleviated the postoperative pain of patients. 3 Low-temperature plasma radiofrequency ablation is a minimally invasive electrochemical technology that has been developed in recent years. Through the 100 kHz plasma radiofrequency electrical field, generated energy can turn the electrolyte liquid between the electrode of the radiofrequency needle and the tissue into a low-temperature plasma state, forming a thin plasma layer that is 100-μm thick in and around the front of the electrode. The ions in the area are accelerated by the electrical field and then transferred the energy to the tissue. Therefore, free-charged ions in the target tissue obtain sufficient kinetic energy and molecular bonds in cells are broken down at a low temperature of 40°C-70°C and decomposed into carbohydrates and oxides, causing protein coagulation and necrosis, as well as cell and tissue fluid dehydration. After the necrotic portion is shed and absorbed, it is repaired by fibrous tissue, resulting in the contraction of the scar, thus achieving the effect of reducing the volume of the target tissue and reducing the capacity. 9
In the present case, the mass in the external ear canal was removed at a low temperature of 40°C-70°C during the operation and the base was ablated, causing coagulative necrosis of the tissue and then shedding of the necrotic tissue, facilitating complete tumor resection and preventing recurrence. The external auditory canal arterial system originates from the maxillary, superficial temporal, and posterior auricular branches of the external carotid artery. The deep auricular artery of the maxillary artery penetrates the anterior wall of the bony external auditory canal through the back of the mandibular joint and then divides into many small branches around the tympanic membrane, entering the surface of the tympanic membrane from the surroundings. The superficial temporal artery runs from bottom to top in front of the tragus and branches into the external auditory canal. The posterior auricular artery runs from bottom to top between the external auditory canal and the mastoid and branches into the external auditory canal through the back of the ear. 10 Low-temperature radiofrequency has the functions of burning and hemostasis at the same time. With the selection of the coagulation mode during the incision, hemostasis was performed while the tumor was resectrated, reducing intraoperative bleeding, ensuring a clear surgical field in the narrow external auditory canal, and making the operation smoother with a shorter operation duration. The characteristic temperature (40°C-70°C) of the low temperature radiofrequency reduced the risk of thermal damage to the nontargeted surrounding tissue, and the heat energy of the continuously generated radiofrequency wave was transferred between the two electrodes, with the temperature generated by the radiofrequency confined to a very small range. Furthermore, the adoption of rinsing with normal saline during the operation further reduced thermal damage and injury to the middle ear, ensuring less trauma, significantly reducing tissue damage, and greatly reducing the degree of postoperative pain. Therefore, the patient experienced less pain and achieved rapid recovery.
A highly differentiated tumor is more common in individuals with squamous cell carcinoma of the ear, which is an aggressive tumor in terms of biological behavior. Proper preoperative evaluation and the correct selection of surgical approaches can be of great importance. In the present case, the effect of the operation was good and there was no recurrence throughout the following 5 years after the operation. It was considered that the cartilage and bone of the external auditory canal could have a certain barrier effect; the tumor did not penetrate the Santorini gap of the external auditory canal or the junction of bone and cartilage and there was no infiltration in the soft tissue around the ear. The primary complication of ear squamous cell carcinoma is local recurrence with a low incidence of metastasis. Early and complete resection is determined to be the optimal course of treatment. The tumor in the external auditory canal in the present case spread to the bottom, anterior, posterior, and top wall, and developed from the outside to the inside with a wide range. During the postoperative dressing change, a catheter with the same diameter as the external auditory canal was indwelled to prevent adhesion and stenosis of the external auditory canal. In addition, a urinary catheter was smeared with tobramycin/diazepamone eye drops to alleviate local edema and inflammation in the external auditory canal.
Conclusions
A highly differentiated tumor is more common in individuals with squamous cell carcinoma of the ear, which is an aggressive tumor in terms of biological behavior. Proper preoperative evaluation and the correct selection of a surgical approach can be of great importance. The effect of the operation was good in the present case and there was no recurrence throughout the following 5 years after the operation. The primary complication of ear squamous cell carcinoma is local recurrence with a low incidence of metastasis. Early and complete resection is the optimal treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.