
Abstract
Introduction
Attic cholesteatoma is a prevalent clinical disease of the middle ear characterized by keratinized squamous epithelial cystic lesions and bone destruction and resorption. 1 This condition can lead to the destruction of several structures, including the lumen of the tympanic chamber, tympanic antrum mastoid process, petrous apex, and eustachian tubes. Cholesteatomas are surrounded by varying thicknesses of epithelial tissue, forming multilayered keratin fibers that create a cystic mass wrapped in an inflammatory response. 2 Historically, the treatment of attic cholesteatoma primarily involved microscopic surgery, including intact canal wall mastoidectomy and modified radical mastoidectomy, both of which have been in use for several decades. 3 However, otoscopy has become increasingly popular for middle ear surgical procedures since the 1990s, particularly for tympanoplasty type I and cholesteatoma confined to the tympanic cavity. 4
In recent years, advancements in perfusion techniques have eliminated factors that previously constrained one-handed operations during otoscopy, such as a blurred field of view, making otoscopic surgical treatment of cholesteatomas more feasible. 5 Otoscopy provides better visualization of the tympanic chamber, tympanic antrum, middle and posterior tympanic chambers, and eustachian tube. Therefore, in this study, we primarily used otoscopy to operate on cholesteatomas in the mastoid and tympanic antrum and compared it to conventional microscopic surgery. 6
We hypothesized that otoscopic continuous perfusion cholesteatoma surgery would have a lower recurrence rate and significant surgical outcomes. Therefore, this prospective study aimed to test this hypothesis and provide more experience with otoscopic surgery.
Data Availability Statement
We affirm that all raw data can be shared. The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request. We affirm that all raw data can be shared. Data are provided within the manuscript or Supplemental Information files.
Materials and Methods
This study was approved by the Ethics Committee of North Jiangsu People’s Hospital (Batch number: 2021ky235), and all methods comply with relevant guidelines and regulations. The hospitalizations for attic cholesteatoma admitted to the Department of Otorhinolaryngology at North Jiangsu People’s Hospital since 2019 were numbered and randomly divided into an experimental group and a control group. We adopted a completely randomized grouping method and used coin toss (ESS group on the front and MES group on the back). The experimental group comprised 38 affected ears, while the control group comprised 42 affected ears. Microscopic ear surgery (MES) was utilized in the control group, whereas endoscopic surgery with a Y-shaped (ESS) under continuous irrigation (ESS) was employed in the experimental group to address cholesteatoma in the mastoid and tympanic antrum, along with reconstruction of the external auditory canal. All patients underwent postoperative follow-up for a maximum of 48 months, a minimum of 24 months, and an average of 30 months.
Inclusion Criteria
a. CT suggests attic cholesteatoma encroaching on the tympanic antrum, not exceeding the entrance of the tympanic inlet.
b. Long-term recurrent pus flow, but in the dry ear stage at the time of surgery.
c. Age greater than 18 years.
Preparation for Surgery
All surgeries were performed under general anesthesia. Preoperative examinations included chest CT, routine electrocardiogram, blood tests, liver and kidney function tests, coagulation profiles, and infectious markers. Specialized examinations included CT of the temporal bone, self-diagnostic audiometry, acoustic impedance audiometry, otoacoustic emission, and otoscopy.
Surgical Instruments
Fiber optics for the surgical endoscopic monitor in the experimental group were provided by STORZ. The surgical endoscopes included 0°, 30°, 45°, and 70° 2.7-mm rigid otoscopes (Hopkins telescope; Karl Storz, Tuttlingen, Germany). This equipment was paired with a 3-chip camera (Karl Storz) and a 20-inch high-resolution monitor, a continuous perfusion system from Shentu, China, and a Bien Air special otological drill. In the control group, a ZISS microscope (Carl Zeiss AG, Germany) was used. In addition to the conventional microscopic instruments, a set of special STORZ microscopic instruments was provided.
Surgical Approach
The surgical steps of the experimental group
a. After general anesthesia, position the patient lying down with the head inclined to the healthy side. For obese patients, a pillow can be placed under the shoulder to facilitate turning the head to the opposite side.
b. 1% lidocaine with 1 ml of solution plus 1 drop of epinephrine was used for local infiltration anesthesia. Administer this to the lower wall, posterior wall, and upper wall of the external auditory canal to reduce intraoperative bleeding. Inject the anesthetic until the skin of the external auditory canal appears white, indicating adequate anesthesia extending from the skin to the tympanic membrane.
c. A hook needle was used to create an incision around the tympanic membrane perforation to induce trauma. A loop cutter was then used to repeatedly scrape the inner side of the tympanic membrane to remove hyperplastic granulation tissue. Scraping continued until bleeding occurred, forming a fresh trauma.
d. At the juncture of the anterior and inferior walls of the external auditory canal, employ a ring cutter to incise up to the intersection of the anterior and superior walls. Make a cut in the skin of the external auditory canal from the 3 o’clock to the 12 o’clock position (Figure 1A). Ensure that the initiation and termination points of the incision are not on the same plane, maintaining a staggered distance of at least 5 mm. If necessary, perform a longitudinal incision parallel to the canal on the upper wall of the external auditory canal, meticulously separating the skin until reaching the osseous ring, and then detach the tympanic membrane from the ossicles. In the upper tympanic region, identifying the short protrusion of the malleus bone can aid in its separation from the tympanic membrane, enabling a complete 360° elevation of the tympanic membrane. For cases involving cholesteatoma in the mastoid cavity, create a longitudinal incision in the anterior wall of the external auditory canal (Figure 1B), extending from the ear tragus to the anterior foot of the helix (Figure 1C), reaching the osseous part of the external auditory canal, thereby forming a Y-shaped incision. Utilize a spacer to adequately expose the posterior and superior osseous portions of the external auditory canal (Figure 1D).
e. Commence by connecting the otoscope to the perfusion scope sheath, followed by attaching the perfusion pump. Set the pump pressure within the range of 110 to 120 mmHg and adjust the flow rate to be between 0.2 and 0.3 L/min. Continuously infuse room temperature saline to establish a unidirectional circulation of water flow within the otologic cavity. Utilize the saline to thoroughly irrigate and maintain a clear surgical field at a specified pressure. During the bone grinding process, employ an intermittent grinding technique, ensuring meticulous attention to detail. Complete bone grinding to clear the area is achievable upon reaching the entrance of the tympanic antrum surrounding the cholesteatoma.
f. During tympanoplasty, auricular cartilage and cartilaginous membrane can be harvested anterior to the Y-shaped incision. In cases of larger defects, auricular cavity cartilage can be utilized to repair the posterior upper wall of the external auditory canal. Gelatin sponges are inserted into the tympanic chamber, followed by resetting the tympanic membrane and external auditory canal flap after placing auditory ossicles and cartilage. Finally, all harvested cartilage and cartilaginous membranes are buried under the skin.
g. The external auditory canal was filled with a gelatin sponge, and gauze was applied to compress the ear screen area. The incision was sutured without requiring a pressure dressing.
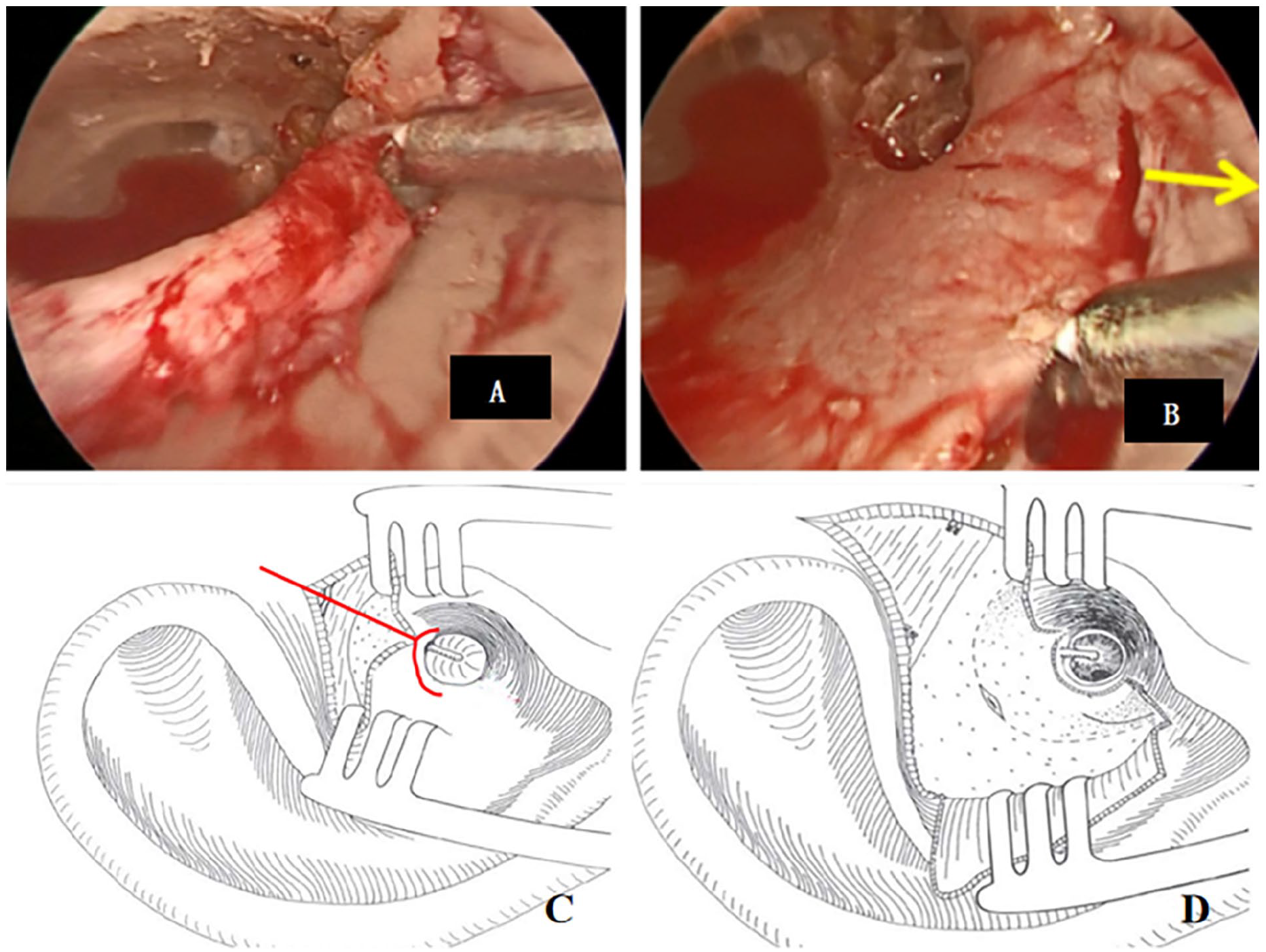
Otoscopic incisions. (A) The first incision in the external auditory canal is known as the C-incision. (B) The second incision is made on the anterior wall of the external auditory canal, extending outward as indicated by the yellow arrows. (C) The caudal part of the Y-shaped incision is positioned directly in front of the cartilage of the ear screen near the anterior foot of the olecranon. (D) Braced incision to maintain exposure during the procedure.
The surgical steps of the control group
a. Administer general anesthesia and position the patient supine with the head inclined toward the healthy side. For obese patients, place a pillow under the shoulder to facilitate easier head positioning.
b. Administer local infiltration anesthesia using 1% lidocaine with 1 drop of epinephrine per 1 ml of solution at the site of the post-auricular incision.
c. Make an incision and prop it open to harvest spare temporal muscle fascia. Incise the posterior, upper, and lower walls of the external auditory canal. Fully expand the incision using a propping device to expose the tympanic membrane. Employ a hooked needle to remove tissue around the tympanic membrane perforation, creating a fresh wound. Use a ring cutter to repeatedly abrade the inner surface of the tympanic membrane to remove proliferative tissue and induce bleeding.
d. Grind the surface bone of the mastoid along the superior spine of the external auditory canal, collect bone powder for backup, and expose the entrance of the tympanic antrum. All patients undergo an open mastoidectomy with canalization due to the presence of cholesteatoma.
e. Excise the cholesteatoma in the upper tympanic chamber and of the tympanic antrum, grind down the facial nerve crest, place artificial auditory ossicles, and use temporal myofascia for shaping the tympanic chamber. Use bone powder to reduce the mastoid cavity and reconstruct the posterior wall of the external auditory canal.
f. Remove part of the cartilage from the auricular cavity and reshape the cavity using skin scissors.
g. Fill the external auditory canal with a gelatin sponge, apply gauze for compression, suture the incision, and apply a pressure bandage.
Postoperative Treatment and Follow-up
Postoperatively, all patients were administered intravenous antibiotics; however, no painkillers were prescribed. Antibiotic gauze used during surgery was replaced at the time of discharge. This gauze was removed during a follow-up visit at the outpatient clinic 1 week after surgery. Follow-up continued for 1 to 2 years. Most gelatin sponges and secretions were typically absorbed within 2 weeks; any remaining material was removed via otoscopy. The healing of the tympanic membrane was monitored at 1, 3, 6, and 12 months post-surgery. Audiological examinations were conducted 3 months after surgery. In addition, a temporal bone CT and otoscopy were performed 1 year post-surgery to assess the recovery process.
Relevant Indicators
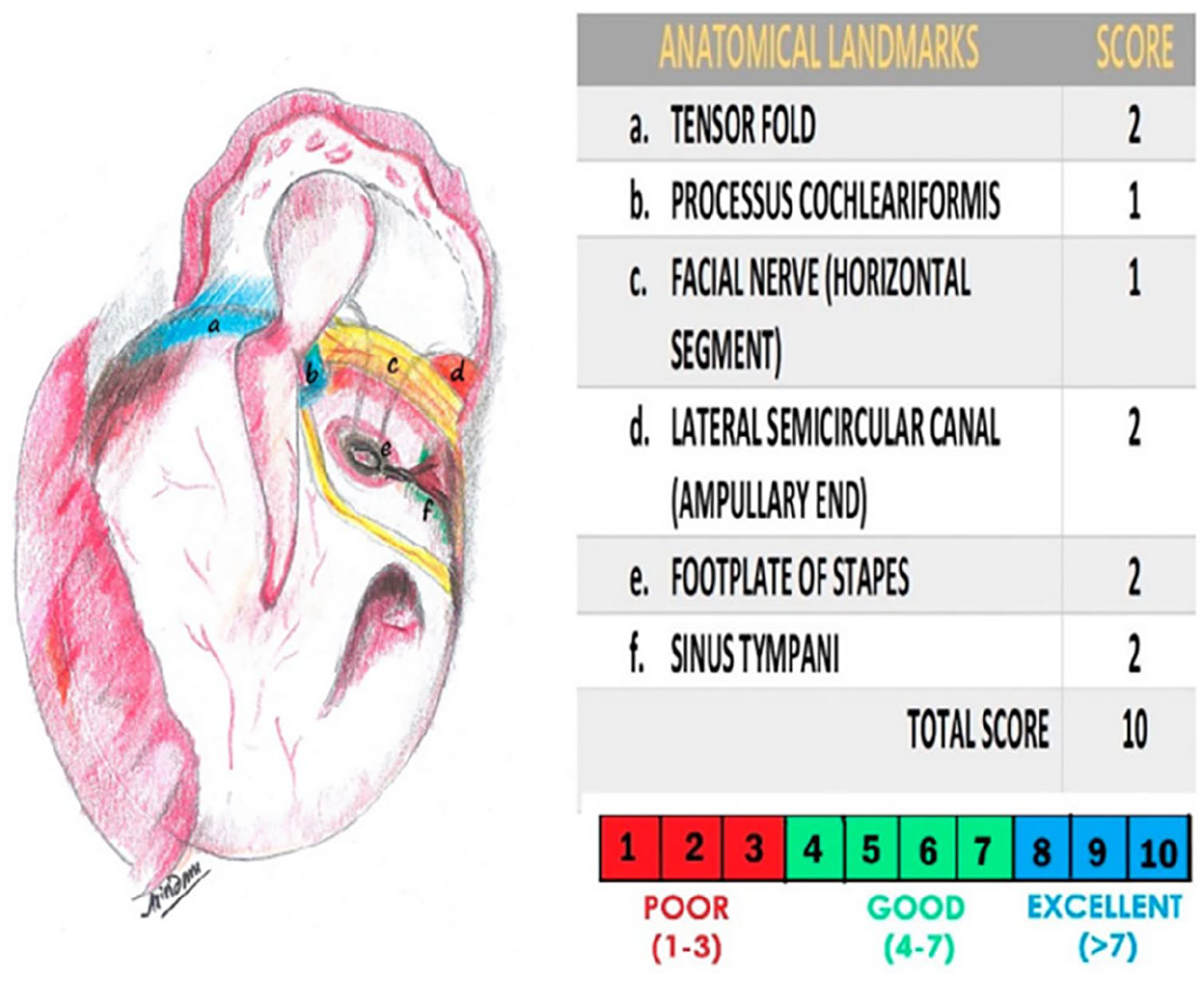
According to the EAONO/JOS, 7 the attic cholesteatoma was classified as follows: cholesteatoma localized in the attic (stage I), a retraction pocket with epithelial self-cleaning function (stage Ia), a retraction pocket with persistent accumulation of keratin-debris (stage Ib), cholesteatoma involving 2 or more sites (stage II), cholesteatoma with intratemporal complications and/or pathologic conditions (stage III), and cholesteatoma with intracranial complications (stage IV). The Middle Ear Structural Visibility Index (MESVI) was used to assess the degree of surgical exposure of certain key structures during the complete resection of cholesteatoma of the upper tympanic ventricle (Figure 2). The higher the MESVI, the higher the degree of surgical exposure. 8
Middle Ear Structural Visibility Index.
Observation Indexes
Our observational indices encompass (1) patients’ basic conditions; (2) intraoperative conditions, which include the MESVI for visual field exposure, intraoperative bleeding, operation time, and complications; (3) postoperative conditions, such as the use of the Visual Analog Scale (VAS) to assess pain intensity 24 hours after surgery, occurrences of facial paralysis, vertigo, nausea, vomiting, tinnitus, cerebrospinal fluid fistulae, and painkiller usage; and (4) postoperative follow-up, which records the perforation healing rate of the tympanic membrane at 1 month, hearing improvement outcomes in both groups (defined as effective when hearing speech frequency improves by more than 15 dB, bone-air conduction gap is less than 15 dB, or the average air conduction hearing threshold reaches 30 dB), and otoscopy results indicating the recurrence of the upper tympanic chamber invagination pocket and cholesteatoma residuals. The surgical procedure is shown in Figure 3.
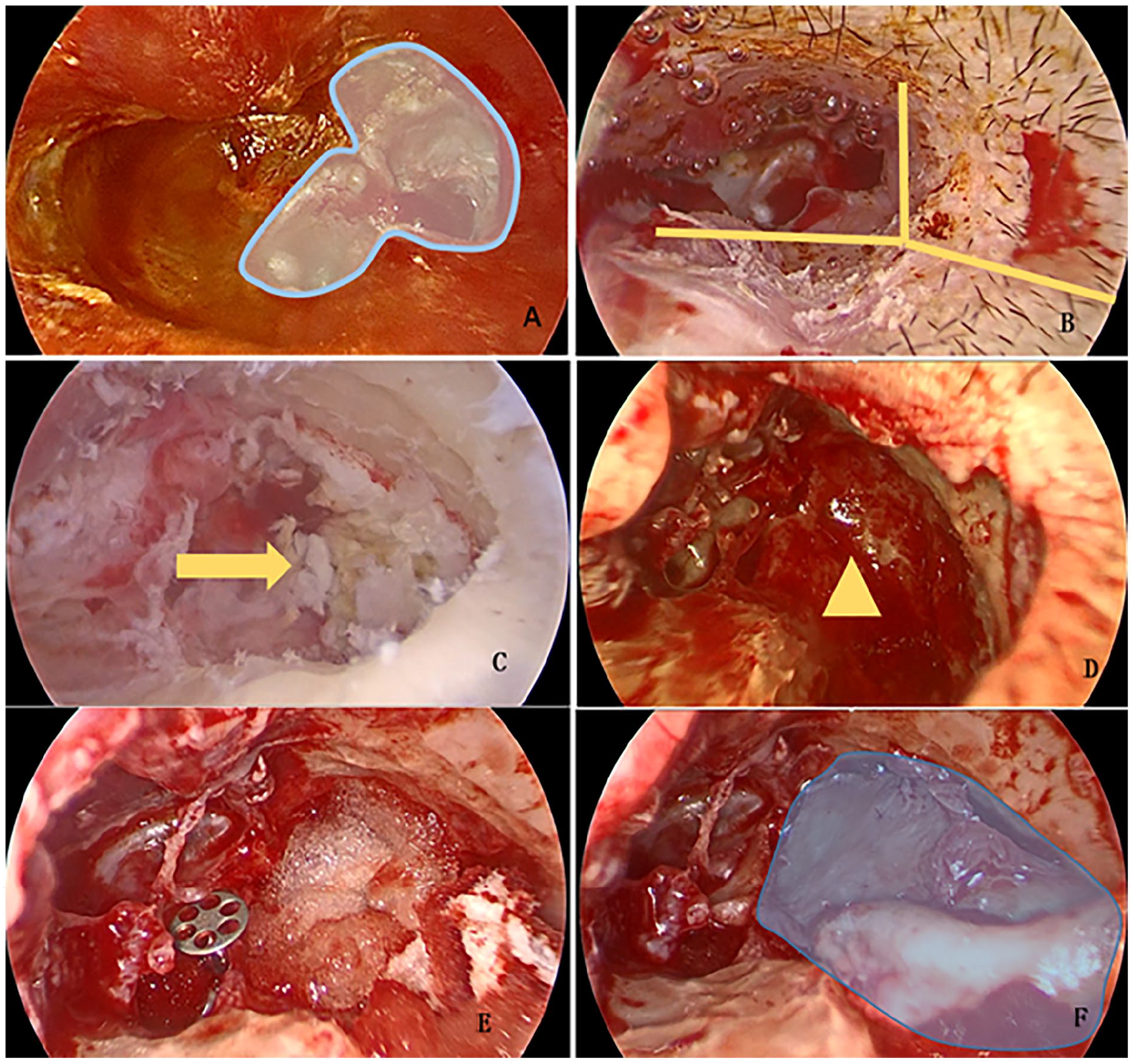
Otoscopic surgical photographs of a patient: (A) Preoperative cholesteatoma of the upper tympanic chamber; (B) “Y” incision to expose the posterior-superior wall of the external auditory canal; (C) Tracing the extent of the cholesteatoma along the cholesteatomatous epithelium under continuous irrigation (yellow arrow point); (D) Removal of the cholesteatoma from the upper tympanic chamber and of the tympanic antrum (yellow triangle); (E) Place the PROP; (F) Reconstruction of the posterior external auditory canal using otoconchal cartilage for the upper wall of the external auditory canal.
Statistical Methods
SPSS statistical software was used to analyze the data. Measurement information was expressed as mean ± standard deviation (x ± s), and a t-test was used for comparison between groups. Count information was expressed as the number of cases (n) and percentage (%), and the chi-square test was used for comparison between groups. P < .05 means that the difference is statistically significant.
Results
Following approval from the Ethics Committee of SuBei People’s Hospital, 79 patients with a total of 80 affected ears were enrolled consecutively and assigned random numbers upon admission. Subsequently, they were randomly divided into 2 groups: the experimental group and the control group. Prior to their participation, all patients were informed about alternative surgical modalities and provided informed consent.
Characteristics of Surgical Patients
A total of 80 affected ears from 79 patients diagnosed with chronic otitis media underwent surgical intervention. Notably, one patient’s left ear was assigned to the experimental group, while their right ear was allocated to the control group. Among these cases, 38 underwent surgery with otoscopy, while 42 received microscope-assisted procedures. The patient cohort comprised 34 males and 46 females, with ages ranging from 21 to 72 years. The mean ages for the experimental and control groups were 46.70 ± 9.86 and 48.53 ± 11.63 years, there was no significant difference in the ages of the 2 groups of patients, respectively. The most prevalent sites of cholesteatoma were the posterior superior tympanic chamber (75 cases, 94%), anterior superior tympanic chamber (42 cases, 53%), posterior middle tympanic chamber (25 cases, 31%), and the tympanic antrum (23 cases, 28.7%), in descending order of frequency. All patients underwent intraoperative auditory chain reconstruction. Further details regarding preoperative conditions are presented in Table 1. Previously operated is to have 1 ear operated on before and to have the other ear operated on this time.
Characteristics of Surgical Patients.
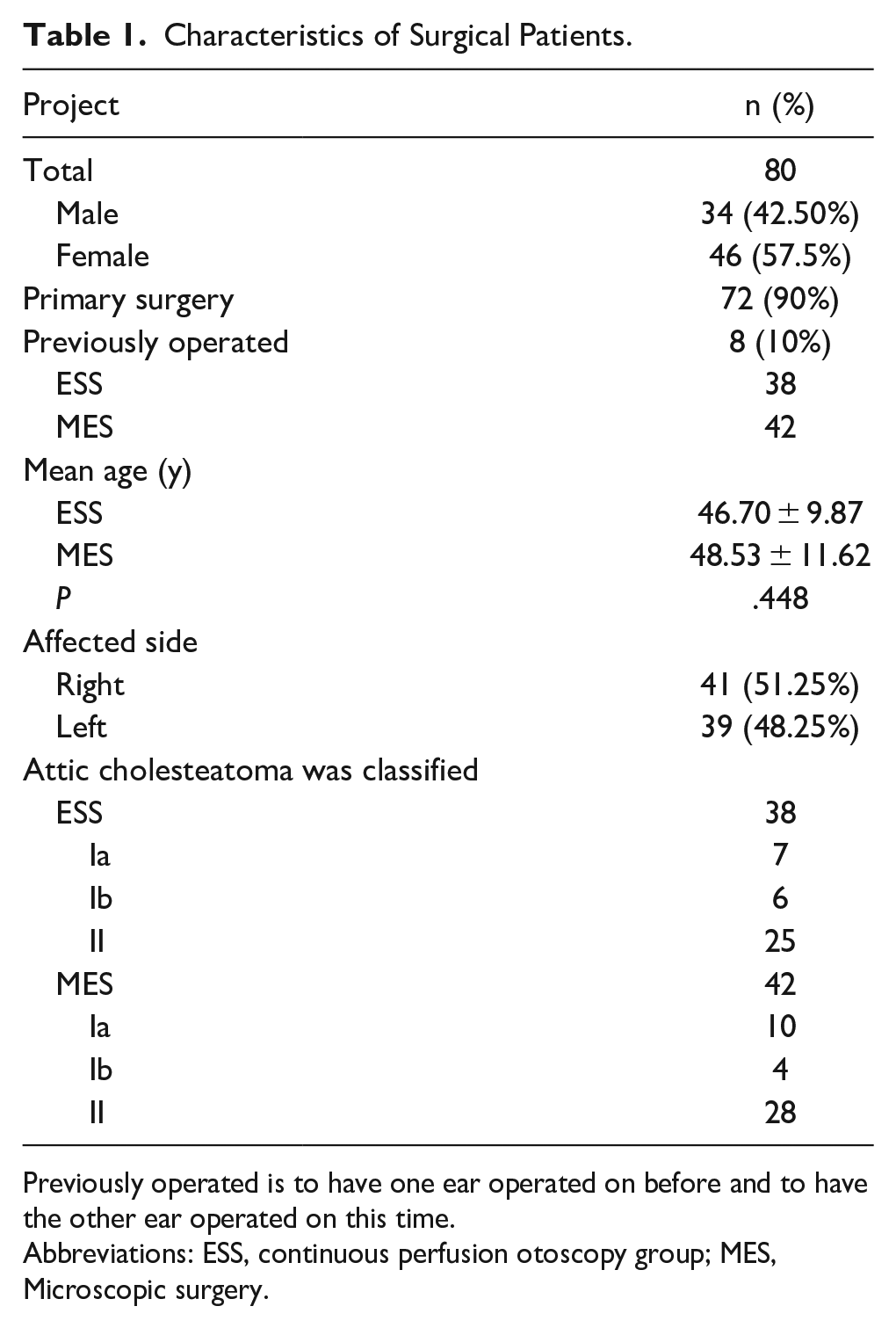
Previously operated is to have one ear operated on before and to have the other ear operated on this time.
Abbreviations: ESS, continuous perfusion otoscopy group; MES, Microscopic surgery.
Preoperative CT Statistics
Preoperative CT scans revealed jugular bulb elevation in 9 cases, with 5 cases found in the microscope group and 4 cases in the otoscopy group. Furthermore, low meningeal position was observed in 6 cases, with 2 cases identified in the otoscopy group and 4 cases in the microscope group. In addition, one case of external semicircular canal abnormality was preoperatively detected in the otoscopy group and confirmed during surgery. However, these observed differences did not reach statistical significance.
Intraoperative Statistics
Intraoperative visual field exposure MESVI index
The median MESVI was 8 (range: 6–10) in the experimental group, while it was 5 (range: 4-8) in the control group. Interestingly, the experimental group required significantly less bone grinding compared to the control group. This can be attributed to the endoscopic approach, which eliminated the need for mastoid abrading and avoided abrasion of the facial nerve crest. The endoscopic technique also provided superior magnification compared to the microscope, and the use of angled lenses (30° and 45°) further enhanced visualization (Figure 4).
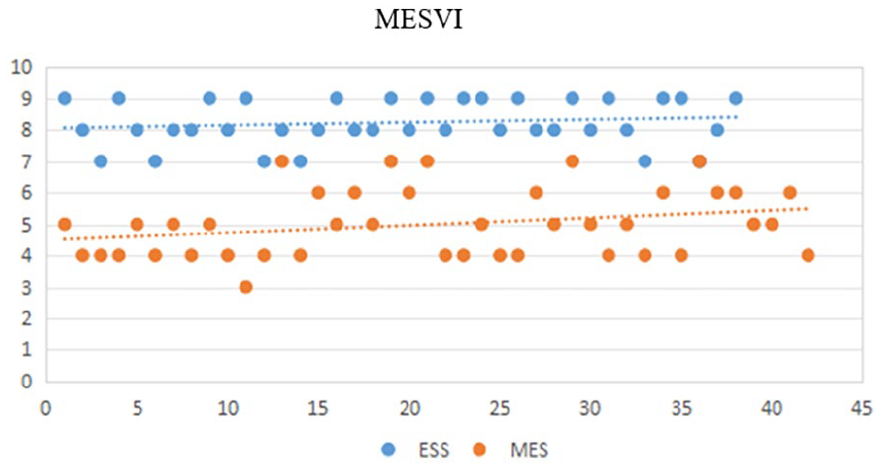
Middle ear MESVI score
Intraoperative complications
Throughout the surgical procedures, no cases of cerebrospinal fluid leakage were observed in patients undergoing endoscopic procedures. However, in the microscopic group, 1 patient experienced cerebrospinal fluid leakage in the ear, which was successfully repaired without any subsequent abnormalities. Nerve damage to the tympanic cord occurred in 4 patients in the endoscopic group and 3 patients in the microscopic group during surgery. In addition, vertigo was reported in 1 patient in the endoscopic group and 3 patients in the microscopic group. Postoperatively, 4 patients in the endoscopic group and 3 patients in the microscopic group developed hyposmia. Conversely, tinnitus occurred in 3 patients in the endoscopic group and 4 patients in the microscopic group. Furthermore, transient facial nerve paralysis was observed in 1 patient from each group (Figure 5).
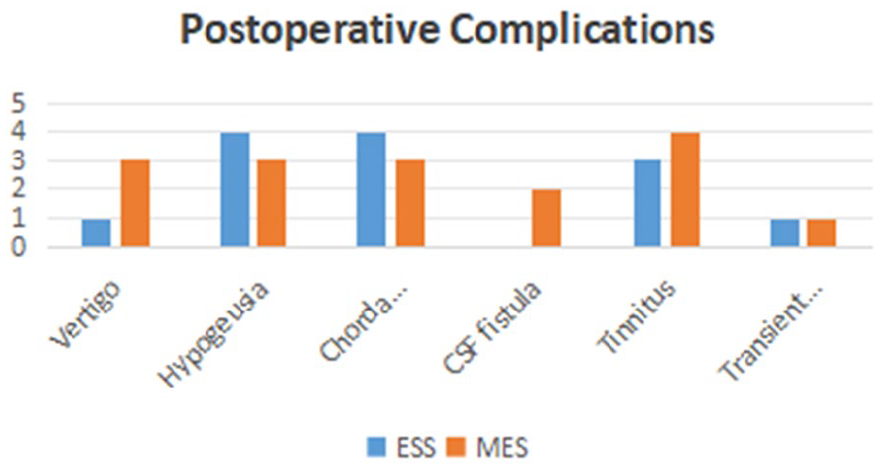
Intraoperative complications.
Surgical time, intraoperative situation
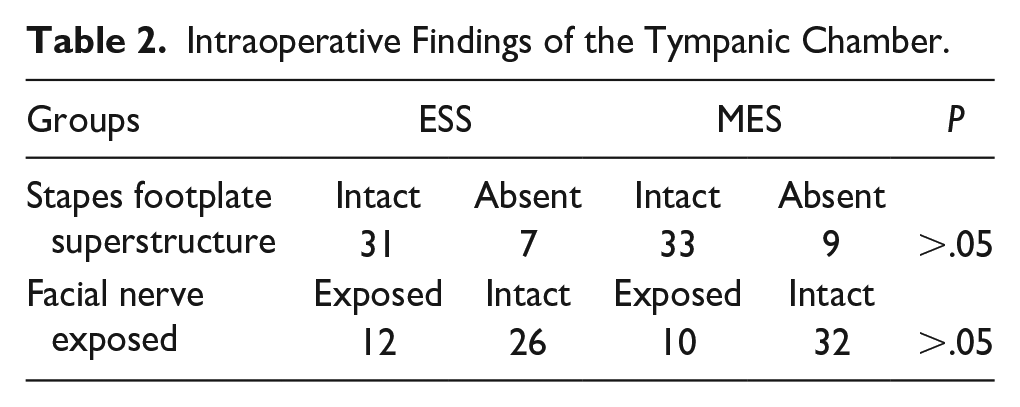
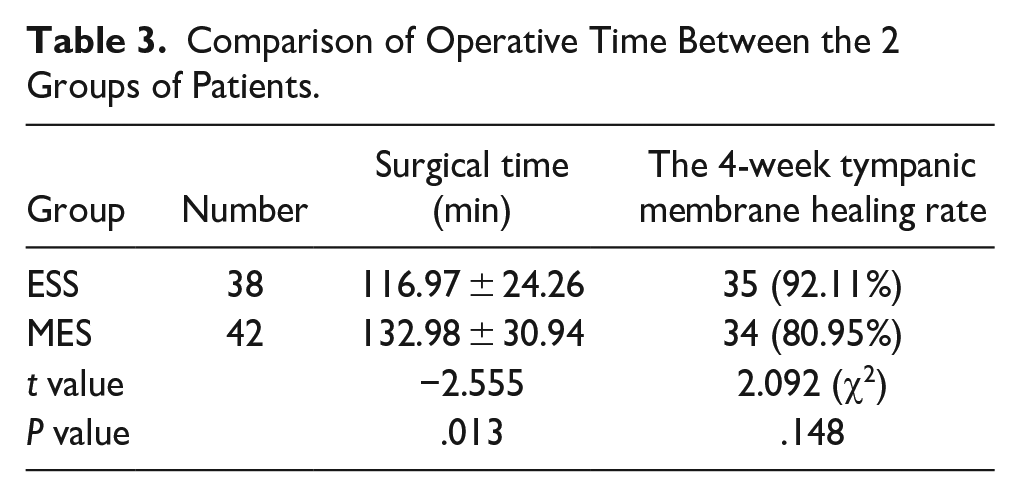
Intraoperative findings revealed that within the otoscopic group, 31 patients had intact structures on the stapes footplate, while 7 patients experienced destruction of these structures. By contrast, the microscopic group had 33 patients with intact structures and 9 with destruction on the stapes footplate. The facial nerve was exposed in 12 cases in the otoscopic group and 10 cases in the microscopic group; the remaining patients in both groups had intact facial nerves, with 26 in the otoscopic group not showing exposure (refer to Table 2). In addition, 1 patient in the microscopic group showed destruction of the external semicircular canal, which was successfully covered with fascia and healed well postoperatively. All patients underwent artificial auditory bone implantation during surgery to prevent the recurrence of cholesteatoma. The mean operative times were 116.97 ± 3.94 minutes for the endoscope group and 132.98 ± 30.57 minutes for the microscope group, showing statistically significant differences (P < .05, Table 3).
Intraoperative Findings of the Tympanic Chamber.
Comparison of Operative Time Between the 2 Groups of Patients.
Postoperative Situation
In the postoperative phase, 17 patients from the microscopic surgery group required oral or intravenous pain medication, compared to only 2 patients in the otolaryngoscope group, demonstrating a statistically significant difference (P < .05). Pain intensity for the 2 groups was recorded using a VAS for 24 hours after surgery. The results indicated that all patients in the otolaryngoscope group reported minimal or no pain and did not require analgesic medication (Figure 6). By contrast, 40.48% of patients in the microscopic surgery group needed oral or intravenous pain medication. Notably, some patients in this group even opted out of head wrapping due to discomfort. The mean pain score was significantly lower in the otolaryngoscope group at 2.39, compared to 5.29 in the microscopic surgery group (P < .05).
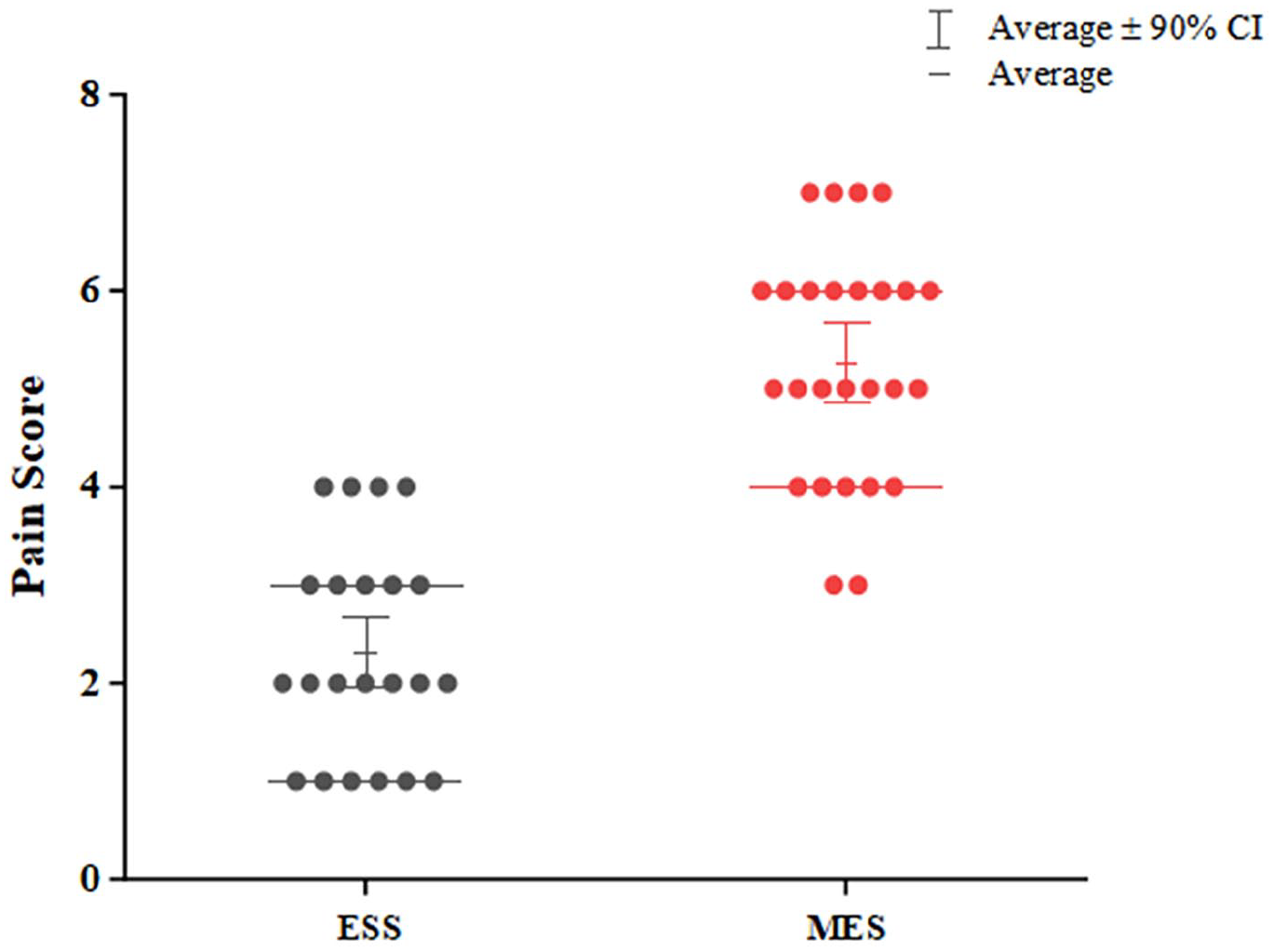
Postoperative patient pain score.
Postoperative Complications
Postoperative vertigo was reported in 1 patient in the endoscopy group and 3 patients in the microscope group; however, all affected patients improved and were discharged within 1 week after the operation. Regarding taste abnormalities, 4 patients from the endoscopy group and 3 from the microscope group experienced postoperative changes in taste. In addition, facial paralysis occurred in 1 patient from the endoscopy group on the seventh day post-operation and 1 patient from the microscope group within 24 hours post-operation. Both patients fully recovered following hormone therapy and nutritive nerve treatment, with no lasting sequelae.
Record of Postoperative Follow-up
One week post-surgery, secretions will be suctioned and the use of ear drops will continue. By the second week, the tympanic membrane is observed for healing; well-healed membranes may lead to discontinuation of ear drops, whereas infections will require fluid therapy. A follow-up re-examination is scheduled for the fourth week, which includes an otoscopy to assess the healing of perforations, check for recurrence of invagination in the upper tympanic chamber, and evaluate any residual cholesteatoma. In addition, audiometry will be conducted to observe postoperative hearing improvements. The assessment criteria for effective hearing improvement include an increase in speech frequency of more than 15 dB, a bone-air conduction gap of less than 15dB, or an average air conduction hearing threshold reaching 30 dB.
Tympanic membrane healing of patients in the endothelial microscopy group and the microscopy group
At 4 weeks postoperatively, 3 patients in the ESS group experienced non-healing of the tympanic membrane, while the MES group had 8 such cases. However, patients in the endothelial group exhibited a higher healing rate, with this difference being statistically significant. Following targeted management, 1 patient from the ESS group and 4 from the MES group required a second operation for repair of the tympanic membrane. After these interventions, all patients experienced successful healing.
Mean hearing recovery level and hearing improvement of patients in the MES group and the ESS group
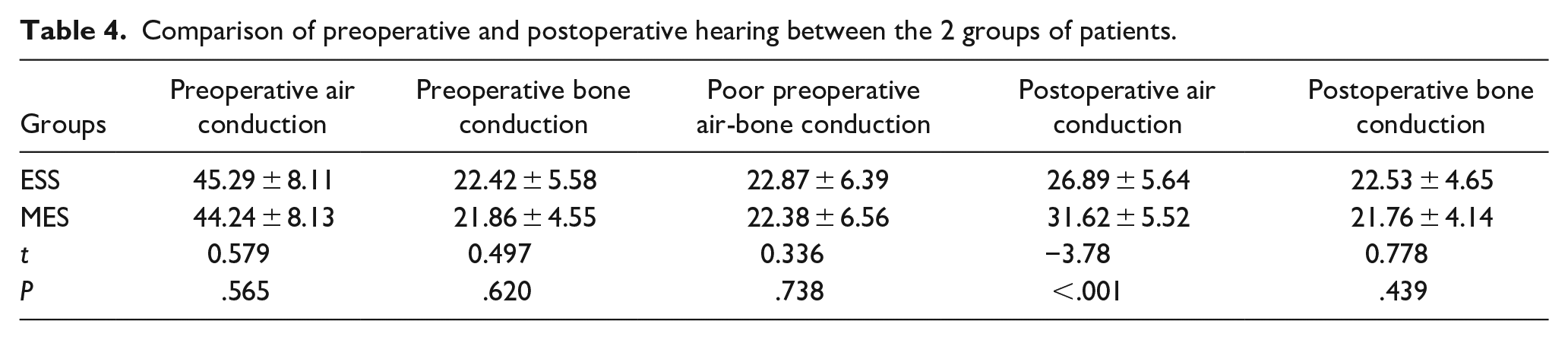
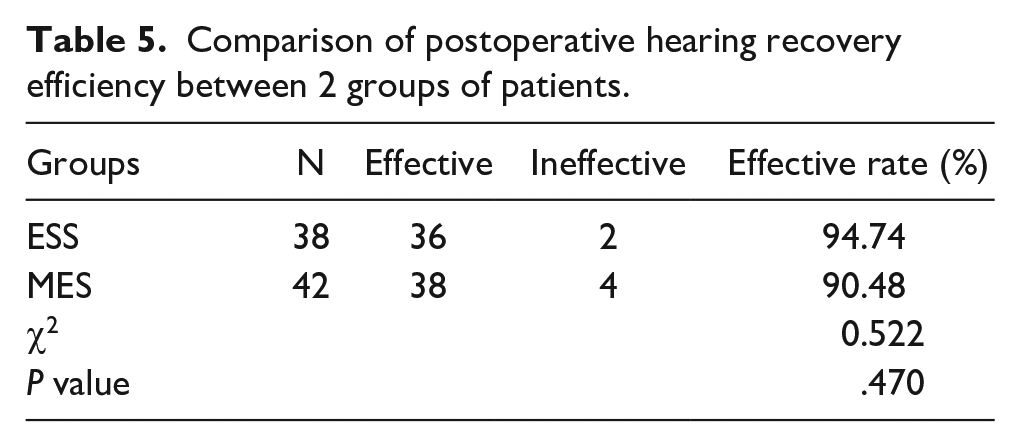
Preoperative hearing assessments between the ESS and MES groups, including measures of air conduction, bone conduction, and air-bone conduction differences, showed no significant differences (P > 0.05). In the MES group, the minimum and maximum values of postoperative air-bone conductance were 1, 24, and the median value was 10; in the ESS group, the minimum and maximum values of postoperative air-bone conductance were 1, 19, and the median value was 4. The nonparametric test showed that the postoperative hearing effect of ESS patients was better than that of MES patients, and the difference was statistically significant (P < 0.001). Postoperatively, the endoscope group demonstrated significantly greater improvement in air conduction compared to the microscope group (Table 4). Furthermore, the postoperative air-bone conduction gap in the endoscope group was smaller, indicating a statistically significant and superior therapeutic effect in terms of hearing restoration (P < 0.05). The chi-square test revealed a significant difference in hearing improvement between the ESS and MES groups (P < 0.001), highlighting the efficacy of the endoscopic approach in enhancing postoperative hearing recovery (Table 5).
Comparison of preoperative and postoperative hearing between the 2 groups of patients.
Comparison of postoperative hearing recovery efficiency between 2 groups of patients.
Recurrence of cholesteatoma
In the ESS group, 2 patients exhibited cholesteatoma recurrence, with 1 case observed in the upper tympanic fossa and the other in the medial part of the bone crest of the posterior wall of the upper tympanic fossa. Conversely, within the MES group, 5 patients experienced cholesteatoma recurrence, distributed as follows: 2 in the facial nerve fossa, 1 in the otosalpinx, and 2 in the upper tympanic fossa. The recurrence rates of cholesteatoma were 5.26% (n = 2) in the ESS group and 11.9% (n = 5) in the MES group, indicating a statistically significant difference between the 2 groups.
Comparative analysis of patients’ postoperative vestibular reactions
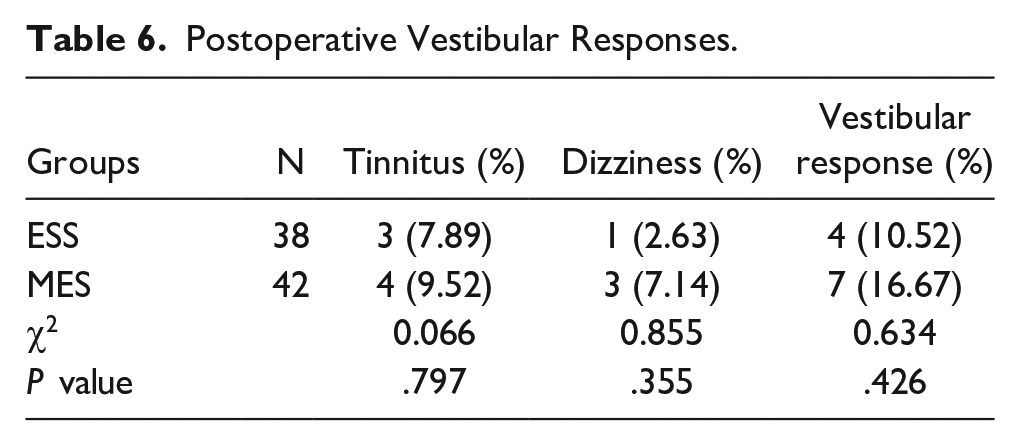
In the ESS group, 3 patients reported experiencing tinnitus, while 1 patient reported symptoms of dizziness and nausea, resulting in an incidence rate of vestibular reactions of 10.52% (Table 6). Conversely, within the MES group, 4 patients reported tinnitus, and 3 patients reported symptoms of dizziness and nausea, resulting in an incidence rate of vestibular reactions of 16.67%. Statistical analysis indicated no significant difference in postoperative vestibular reactions between the 2 groups (P > .05).
Postoperative Vestibular Responses.
Discussion
Treatment of Attic Cholesteatoma
The management of cholesteatoma has been practiced for decades since its discovery. Attic cholesteatoma typically originates from the Prussak gap, extending through the upper tympanic chamber and tympanic antrum to the mastoid. 9 Despite the early utilization of otoscopy for ear examination and treatment, microscopy remains the conventional approach for managing cholesteatoma. While cholesteatoma confined within the tympanic antrum can be exposed and excised using an otoscope and curette, mastoidectomy is often necessary if it extends into the mastoid cavity or mastoid tip. 10 It is worth noting that most acquired cholesteatomas originate in the superior tympanic chamber or middle ear cavity. While microscopy can access these areas, it requires passage through the skin behind the ear, the mastoid bone, and the tympanic antrum, posing a risk of damage to vital structures such as the dura mater at the base of the skull, facial nerve, and semicircular canal. By contrast, endoscopy offers an alternative approach that allows for cholesteatoma removal through the external ear canal and mastoid process. Otoscopy via the external auditory pathway, unlike microscopy, avoids traversing the sigmoid sinus and positions the skull base at a more distant point. In addition, the facial nerve lies centrally in the field of view during otoscopy, minimizing the risk of damage to surrounding tissues. 11 Consequently, there is a growing trend among practitioners worldwide to explore endoscopic techniques for cholesteatoma removal within the middle ear, upper tympanic chamber, and even the antrum tympanicum and mastoid. Endoscopy offers the advantage of single-handed operation, simplifying surgical manipulation. Initially, endoscopes were primarily used for tympanoplasty or cholesteatoma removal in the tympanic cavity.8,12 However, advancements such as the introduction of perfusion systems have addressed concerns regarding bleeding and endoscope lens contamination during underwater bone grinding. Nonetheless, previous endoscopic approaches were limited to the upper tympanic cavity, tympanic chamber, and eustachian tube, with cholesteatoma removal in the mastoid process presenting greater difficulty. 13 To address this, our study adopts an otoscopic Y-shaped incision. The first incision, made internally in the ear canal near the cartilaginous and osseous junction from 3:00 to 12:00, allows access to the upper tympanic ventricle, posterior tympanic ventricle, and part of the tympanic antrum. The second incision is the tragus-front foot of the helix incision, the incision near the anterior wall of the first incision, which extends outward between the tragus and the front foot of the helix, providing access to the antrum tympanicum and part of the mastoid process. This approach effectively exposes the posterior superior wall of the external auditory canal, it is convenient for mastoid bone drilled and clear visualization of the upper tympanic chamber, antrum tympanicum, and mastoid cholesteatoma. While there was no significant difference between endoscopic and microscopic methods for reconstructing the auditory ossicle chain, a disparity exists in tympanic membrane reconstruction. Microscopic reconstruction of the posterior wall of the external auditory canal relies on powdered mastoid bone, while endoscopic reconstruction of the tympanic membrane relies on cartilage. Nevertheless, the comparative results indicate that the improvement in hearing achieved with otoscopy is superior to that achieved with microsurgery, this is consistent with the research results of Tang, Yiyang et al. 14 This may be related to the cartilage-cartilage membrane complex to replace the tympanic membrane in the ESS group.
Exposure of Surgical Field
Surgical failure commonly stems from postoperative infection, residual cholesteatoma, and cholesteatoma recurrence. 15 Among these factors, residual cholesteatoma is particularly significant, with key areas prone to residue including the tympanic orifice of the pharyngeal tube, the tympanic antrum, the stapes base plate, the facial nerve crypt, processus cochleariformis, and the juxtapapillary ridge of the external hemicircular canal. Adequate exposure to these anatomical regions is crucial during surgery. 16 The MESVI stands as the sole grading system for assessing exposure in middle ear surgery, utilizing a 10-point scale based on the visibility of specific key anatomical landmarks. Our study revealed that otoscopy achieved significantly higher MESVI scores compared to microscopy. This discrepancy can be attributed to otoscopy’s broader viewing angle, multiple endoscope angles, and greater magnification, facilitating flexible observation of the upper tympanic chamber, the Eustachian tube, the upper tympanic fossa, and even the space at the tip of the mastoid process. 17 Furthermore, otoscopy resulted in significantly less bone abrasion compared to microscopy, simplifying the removal of hidden cholesteatomas and reducing the risk of residual cholesteatoma, a potential cause of surgical failure. Conversely, microscopy requires more bone destruction to attain a larger viewing area, and the constant need to reposition the microscope during surgery prolongs the procedure, necessitating frequent refocusing and increasing surgical duration. 18
The Choice of Surgical Incision
The otoscopic system is frequently employed in treating middle ear cholesteatoma, with various incisions available for cholesteatoma management. These include the basic “C” incision, primarily utilized for tympanic surgery, which does not afford complete exposure to the upper tympanic chamber. 19 While suitable for tympanoplasty, excising upper tympanic chamber cholesteatoma, and reconstructing the auditory ossicle chain, it is insufficient for addressing cholesteatomas of the mastoid process, tympanic antrum, or mastoid process tip. To address this limitation, we devised a modified C-shaped incision near the upper wall of the external auditory canal. This incision extends from the ear canal’s incision point to the cartilage of the auricle’s scaphoid fossa and the anterior margin of the ear canal’s outer lip. By meticulously separating the skin of the external auditory canal and employing small retractors, complete exposure of the canal’s posterior wall is achieved, mitigating the risk of tympanic membrane flap interference during drill use. Subsequently, a parallel incision along the upper canal ridge provides full exposure of the surgical site, enabling visualization of cholesteatoma within the upper tympanic chamber, tympanic antrum, and mastoid process. Moreover, a Y-shaped incision can be utilized to create a canal tunnel to the mastoid process in the external auditory canal’s posterior wall using an abrasive drill. This approach facilitates cholesteatoma observation, allowing for precise determination of the extent of posterior canal wall resection based on cholesteatoma characteristics, thereby significantly reducing surgical duration. 20 In addition, endoscopic surgery minimally alters the external auditory canal’s structure, contrasting with the broader canal alteration seen in microscope-assisted procedures, aligning more closely with the natural physiological configuration of the external auditory canal.
Surgical Outcomes
During our study, we observed significant advantages of the ESS group over the MES group in terms of postoperative hearing status, tympanic membrane healing, and both intraoperative and postoperative delayed complication rates following ESS surgery. This suggests that the endoscopic one-handed manipulation in a 2-dimensional space does not significantly impact the 2-handed manipulation in a 3-dimensional space relative to microscopic manipulation. No notable difference was found in their vestibular response rates, indicating that continuous unidirectional perfusion of normothermic saline below body temperature did not elevate vestibular response incidence. 8 Moreover, the ESS group demonstrated superiority in shortening operation time, reducing bleeding, and minimizing postoperative dry ear duration. Due to reduced bone removal, there was no need for deliberate bone powder collection for posterior external auditory canal wall reconstruction. Continuous endoscopic irrigation effectively flushed bone powder and blood from the operative area while maintaining lens clarity, facilitating the removal of minute cholesteatomas. The lower cholesteatoma residual and recurrence rates in the otoscopy group were attributed partly to the rinsing effect of continuous irrigation, which could dislodge some cholesteatomas, and partly to the higher visual field score. Although Tseng et al. concluded no statistically significant difference in the hearing improvement and graft success rates between endoscopy and microscopy groups through META analysis, 21 our findings suggested better hearing improvement in the ESS group, which may require validation with a larger sample size.
Surgical Complications
Postoperative complications encompass those occurring during and after surgery. Intraoperative complications include facial nerve injury, tympanic cord nerve injury, hemorrhage, cerebrospinal fluid leakage, cholesteatoma residue, and outer semicircular canal injury. 22 Immediate postoperative complications comprise pain, tinnitus, vestibular reactions (vertigo, nausea, and vomiting), transient facial paralysis, and delayed facial paralysis. Long-term complications include cholesteatoma recurrence and unhealed tympanic membrane perforation, with cartilage displacement. In our study, intraoperative complications such as facial nerve injury, tympanic cord nerve injury, cerebrospinal fluid leakage, and cholesteatoma residue showed no significant difference between the 2 groups. However, patients in the ESS group experienced significantly less bleeding compared to the MES group. This reduction may be attributed partly to reduced bone abrasion in the otoscopic group and partly to the smaller surgical incision, as well as the vasoconstrictive effect of saline solution at a lower temperature than body temperature, contrary to the findings of Magliulo et al. 23 Postoperative pain scores were higher in the microscopic group than in the endoscopic group, with a statistically significant difference between the 2 surgical approaches, consistent with other studies. 24 Richard Salzman reported that among cholesteatoma patients, 88% of endoscopic patients and 43% of microscopic patients using the endaural approach, as well as 75% of microscopic patients using the retroauricular approach, required no postoperative painkillers on day 1. 25 This discrepancy may be attributed to smaller incisions and less bone removal in the endaural group, as well as the absence of postoperative compression bandages, reducing pain incidence. The best follow-up time for patients with cholesteatoma is 5 years or more, while our patient’s follow-up time is relatively short, only 2 years. However, based on our follow-up results, we believe that endoscopic ear surgery has advantages over microscopic surgery. We will continue to strengthen follow-up and observe the recurrence of cholesteatoma.
The use of otoscopic surgery for the treatment of cholesteatoma originating from an invaginated pocket in the upper tympanic chamber, combined with continuous perfusion, addresses several challenges. It allows for one-handed operation and minimizes the risk of lens contamination by blood while also improving cholesteatoma removal, visualization of the middle ear, and hearing outcomes. In addition, it leads to a higher rate of tympanic membrane healing, requires less bone removal, and reduces postoperative pain. These advantages make endoscopic ear surgery particularly beneficial for skilled practitioners.
Supplemental Material
sj-doc-1-ear-10.1177_01455613241306964 – Supplemental material for Comparison of the Efficacy of Endoscopic Continuous Perfusion Combined With Y-Shaped Incision and Microscopic Retroauricular Incision in the Treatment of Attic Cholesteatoma: A Randomized Prospective Study
Supplemental material, sj-doc-1-ear-10.1177_01455613241306964 for Comparison of the Efficacy of Endoscopic Continuous Perfusion Combined With Y-Shaped Incision and Microscopic Retroauricular Incision in the Treatment of Attic Cholesteatoma: A Randomized Prospective Study by Qi Yan, Ying Wang, Li Xu, Baoxu Liu, Haiyong Sun, Bin Zhu and Bing Guan in Ear, Nose & Throat Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.