
Abstract
Introduction
The journey of myringoplasty started with Berthold in 1878 1 and Ely in 1880 2 when they published their surgical techniques using skin graft from the forearm to repair tympanic membrane perforation. Another major step was in 1952 when Wullstein and Zöllner presented the basics of tympanoplasty technique and described tympanoplasty classification of their own. 3 Their technique was an overlay tympanoplasty with full- or split-thickness or pedicle skin grafts obtained from forearm or canal skin. 4 Later in 1960, Shea presented a vein graft and an underlay technique for tympanoplasty that was followed by Storrs describing the temporalis fascia underlay technique. 5 A few years later in 1963, Goodhill et al published their article in which they used tragal perichondrium as a graft. 6 In 2002, Kartush et al described over-underlay tympanoplasty where the graft is placed over the malleus and under the annulus which is still widely used today for all kinds of grafts. 7
Since its first description in 1963, cartilage tympanoplasty has evolved in various ways by different surgeons. At first, the tragal perichondrium was used alone, and then septal and costal cartilage was used as graft and ossicular reconstruction material. The cartilage palisade technique was developed afterward. Using cartilage-perichondrial grafts or island grafts became popular over time as described in miscellaneous shapes. The most popular one used today is developed by Glascock et al and Damhoffer et al where the perichondrium is reflected from the tragal cartilage from 1 side like a book cover and then the attached cartilage is trimmed in a circular way with a strip removed to fit the malleus.8-11
The objective of this study is to compare graft success and hearing outcome between traditional tragal island cartilage tympanoplasty (TICT) and conchal cartilage-reinforced temporalis fascia graft tympanoplasty (CCRTT). In our technique, a piece of conchal cartilage is placed anteriorly and laterally over the temporalis fascia graft, in between the graft and anterior annulus to eliminate the gap between the graft and annulus to stabilize the temporalis fascia, which is hard to position in total and subtotal perforations, thus preventing medialization of the temporalis graft.
Materials and Methods
In this retrospective study, records of patients who underwent tympanic membrane reconstruction were reviewed from 2018 to 2023. Patients older than 12 years of age, having subtotal (>70% of the eardrum) or total (>90% of the eardrum) tympanic membrane perforation with a dry ear of 3 months, regardless of their ossicular chain status, were included in the study. Patients with cholesteatoma, sensory neuronal hearing loss, or with less than a 6-month follow-up were excluded from the study. The patients underwent computed tomography (CT) of the temporal bone (axial and coronal views) preoperatively, pure tone audiometry, and acoustic immittance tests were performed preoperatively and postoperatively. This study was approved by the ethics committee of our institution.
Fifty type 1 tympanoplasties (22 males, 28 females) performed in 44 patients (19 males, 25 females) were included in this study. Four of the patients had bilateral tympanoplasties and 2 of them had revision surgeries, 1 from each group. Tragal cartilage island graft was obtained in 27 (54%) and temporalis fascia reinforced by conchal cartilage was used in 23 (46%) tympanoplasties as grafting material.
All myringoplasties were performed microscopically under general anesthesia by the same surgeon. The external auditory canal and the retroauricular sulcus were infiltrated with 2% lidocaine with 0.125 epinephrine (Jetocain amp, Adeka, Turkey) (Figure 1A). First, the margin of the tympanic membrane perforation was circumferentially denuded and freshened microscopically. For the fascia group, after postauricular incision, approximately 2 × 2 cm of areolar tissue overlying the temporalis fascia is harvested for grafting, a 15 mm circular piece of conchal cartilage with its pericondrium obtained from the posterior aspect of the cymba concha. The mastoid cortex periosteum is cut in a T-shape, and the periosteum is raised off the mastoid bone. After the vascular strip incision, the strip is elevated and suspended out of the ear canal using a self-retaining retractor. The tympanomeatal flap is elevated, the annulus is identified, and the middle ear is entered via the rivinius notch. If necessary, the epithelium of the malleus handle and the tympanic membrane remnants involved with tympanosclerosis are removed. After exploring the middle ear, ossicular bones are checked. The middle ear space is packed with Gelfoam® and temporalis fascia grafting was made by over-underlay technique (Figure 1B) and a piece of conchal cartilage was placed over the fascia and under the annulus for supporting anterior part of the perforation and reducing the gap in between the anterior annulus and the graft (Figure1C and D).
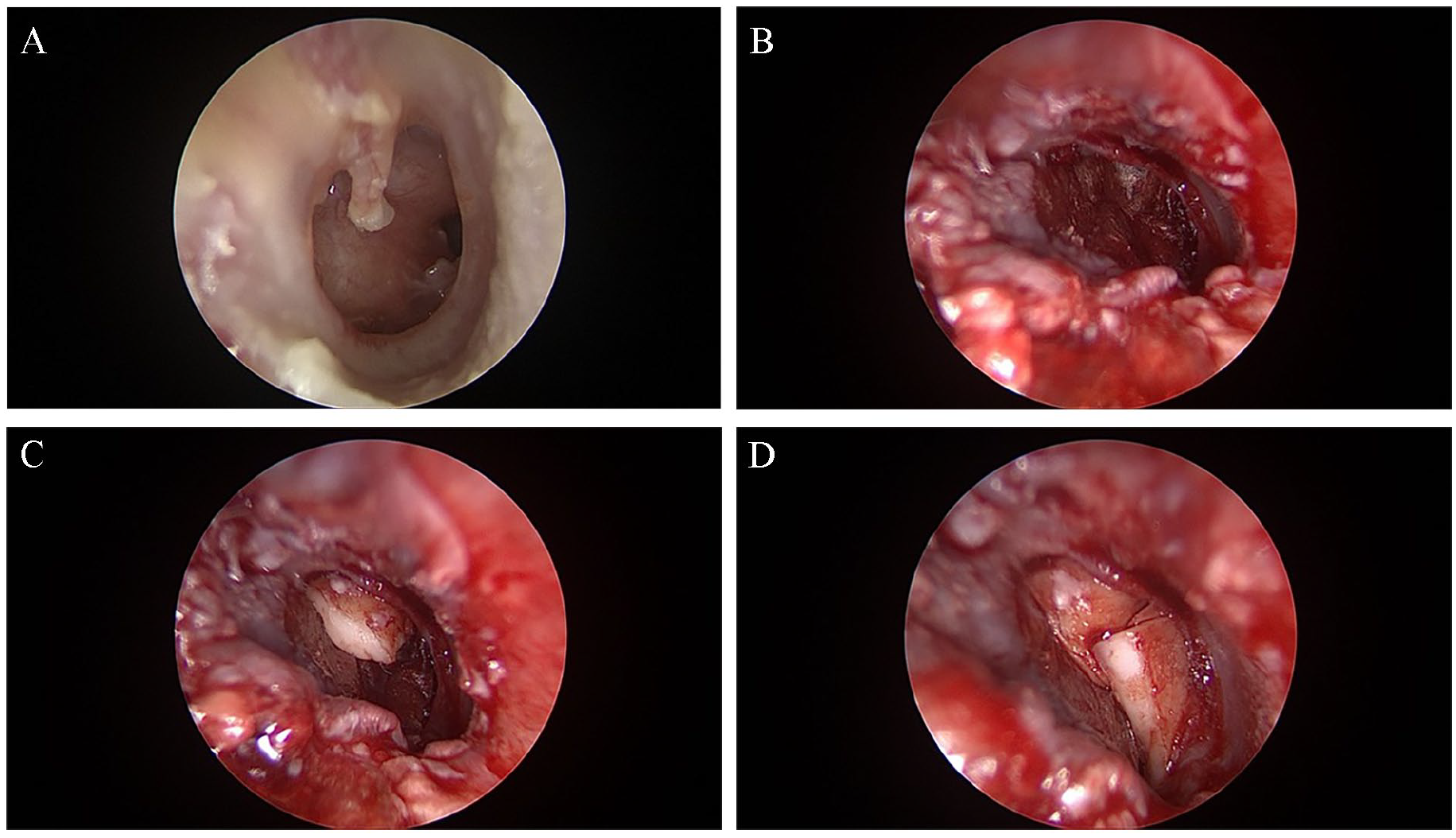
Conchal cartilage-reinforced temporalis fascia graft tympanoplasty procedure. (A) Preoperative total perforation. (B) The temporalis fascia is introduced to the middle ear in an over-underlay method. (C) First conchal cartilage piece is secured over the temporal fascia under the anterior annulus. (D) A second piece of conchal cartilage is secured over the fascia under the anterior annulus to diminish the gap in between thus securing the temporalis fascia.
For tragal island cartilage graft group, a skin incision was made on the medial aspect of the tragus, and the whole medial and lateral cutaneous surface of the tragus (leaving perichondrium attached to the cartilage) is elevated. An incision was made in depth of the tragal cartilage, leaving a 1 to 2 mm strip in depth. The medial aspect of the perichondrium is elevated over the tragal cartilage as the tragal cartilage is still attached to the lateral perichondrium. An island graft is then created according to the size of the perforation by removing the excess cartilage with a Rosen circular cutting knife or a size 11 scalpel blade. In the end, the mesotympanium is packed with Gelfoam®, the graft was placed in an over-underlay fashion, with the perichondrium on top.
The preoperative and one-year postoperative pure tone air and bone conduction thresholds of the patients were recorded at octave intervals from 0.25 to 8 kHz. The pure tone average (PTA) was calculated as an average of 0.5, 1, 2 kHz. The PTA of bone conduction was subtracted from the PTA of air conduction to determine the air-bone gap (ABG).
Data were analyzed with IBM SPSS V23. The Shapiro-Wilk test was used to examine the conformity of the data to normal distribution. The Independent Samples T Test was used in paired group comparisons of parameters that were normally distributed. Mann-Whitney U Test was used in paired group comparisons of parameters that were not normally distributed. Fisher’s Exact Test and Yates Correction were used to examine the relationship between categorical data. Results were presented as mean ± standard deviation, median (minimum-maximum) for quantitative data, and frequency (percentage) for categorical data. The significance level was taken as P < .050.
Results
The mean age for all 50 patients was 31.46 ± 13.9 (min. 12 years, max. 67 years), mean age for male patients was 30.32 ± 14.8, and for female patients was 32.36 ± 13.4, there was no statistically important difference between 2 genders considering the age of the patients (P > .05).
Type 1 tympanoplasty was performed in all patients and bone-cement was used in 7 patients (4 in CCRTT, 3 in TICT group) for incudostapedial re-bridging. Demographics, duration, graft success rate, and hearing gain considering pure tone audiometry and ABG are listed in Table 1.
Demographics, Duration, Graft Success Rate, Hearing Gain of TICT and CCRTT Group.
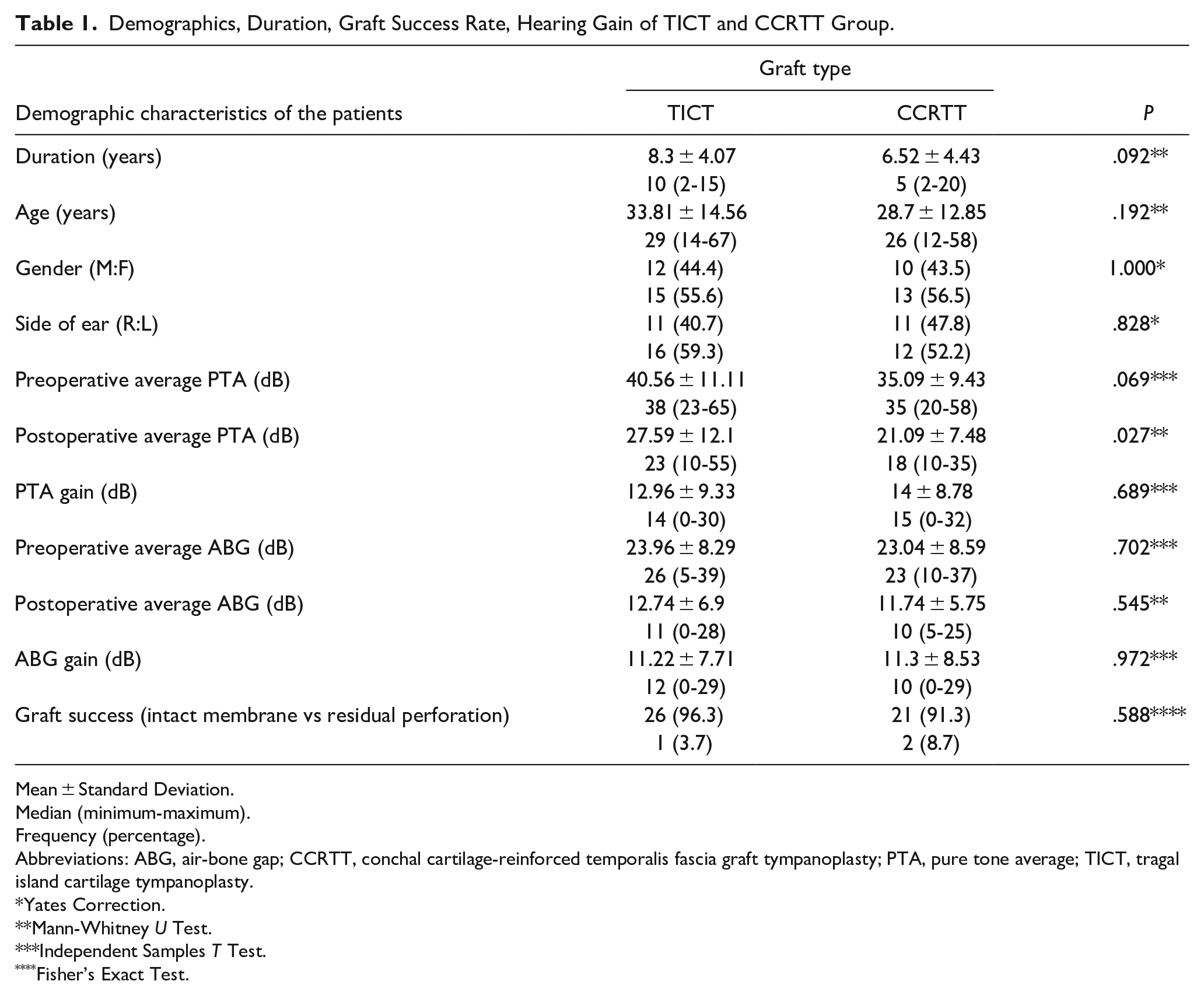
Mean ± Standard Deviation.
Median (minimum-maximum).
Frequency (percentage).
Abbreviations: ABG, air-bone gap; CCRTT, conchal cartilage-reinforced temporalis fascia graft tympanoplasty; PTA, pure tone average; TICT, tragal island cartilage tympanoplasty.
Yates Correction.
Mann-Whitney U Test.
Independent Samples T Test.
Fisher’s Exact Test.
The graft success rate was 96.3% in TICT group and 91.3% in CCRTT group and there was no statistical difference between the 2 groups. There was 1 (3.7%) reperforation in the TICT group and 2 (8.7%) reperforations in the CCRTT group. The difference between the groups considering reperforation was not statistically significant. Considering postoperative hearing gain, PTA gain was 12.9 ± 9 dB for the TICT group and 14 ± 8.8 dB for CCRTT group, and postoperative ABG gain was 11.2 ± 7.7 dB in TCIT group and 11.3 ± 8.5 dB in CCRTT group and again, there was no statistical difference between these 2 study groups for these 2 parameters (Table 1)
Discussion
Anterior reinforcement techniques for preventing medialization of the graft by reducing the gap between the anterior annulus and the graft have been popular for the last 10 years. Various techniques and materials have been used for reinforcement.
In the study of Lou et al, subtotal perforation patients (perforation of more than 50% and less than 75%) operated by endoscopic cartilage reinforcement underlay technique or the traditional cartilage underlay technique, and the results were compared accordingly. In this study, perichondrium was freed from the tragal cartilage in both groups, and in the lateral reinforcement group, first cartilage then perichondrium was placed endoscopically trans-perforation to close the subtotal perforation, and an additional cartilage graft was positioned between the annulus and the perichondrium to minimize the gap in between. However, in the regular group, tympanomeatal flap was elevated and first the cartilage and then the perichondrium were introduced via trans-tympanomeatal flap to close the perforation. In this study, they ascertained that graft success rate and postoperative ABG were the same in both groups however, operation time was significantly shorter in the trans-perforation group. 12 In this study, patients who had more than 70% perforation were included and all patients were operated microscopically in an over-underlay technique. To overcome the bulkiness of the temporalis fascia after introducing it into the middle ear space, conchal cartilage pieces were meticulously placed anteriorly in between the annulus and the fascia both to reduce the gap and stabilize the fascia.
In another study by Kolethekkat et al, temporalis fascia tympanoplasty (TFT) patients were compared to cartilage rim augmented TFT. Conchal cartilage mini strips are located under the annulus circumferentially under the temporalis fascia. In their study, they found that cartilage rim augmentation increased graft success rate and decreased postoperative ABG significantly. 13
Wang et al used an anteriorly localized additional perichondrium patch over cartilage-perichondrium graft to boost graft success rate for large, marginal, or anterior perforations and achieved a high success rate. 14
In their study Shakya et al, used double- or single-layer perichondrium for reinforcement of tragal cartilage tympanoplasty for anterior perforations and found no statistical difference between 2 groups considering graft uptake and hearing improvement. 15
Casas et al used L-shaped tragal cartilage as anterior reinforcement for repair of the total and subtotal perforations where a perichondrium graft was placed over the L-shaped cartilage under the annulus. 16 In this study, conchal cartilage pieces were used for anterior reinforcement and placed over the temporalis fascia under the anterior annulus.
In the study of Tek et al, cartilage from symba concha is used for anterior reinforcement of the temporalis fascia by placing the cartilage under the annulus, and then, temporalis fascia is allocated under the annulus over the reinforcement. They also found statistically significant graft uptake difference between temporalis fascia patients with and without anterior reinforcement and patients with reinforcement had higher graft succession. 17
Various studies compared TFT with different types of cartilage tympanoplasties. In the study of Arora et al, the cartilage palisade technique was compared with TFT, and regarding graft uptake and hearing improvement, no statistical difference was found between the 2 groups. 18 Ashgari et al compared TFT with sliced cartilage tympanoplasty, where they named TFT as “bucket handle” tympanoplasty where the implanted fascia was secured under the anterior flap. In their study, no statistically significant results were found regarding hearing improvement and tympanic membrane closure. 19 In the study of Ciger et al TFT was compared to a conchal cartilage graft, shaped as a wheel and perichondrium, but although there was no difference regarding hearing, a statistically significant difference was assessed regarding graft success. 20 Jain et al analyzed the difference between TFT and tragal cartilage island graft and found that although no difference in hearing improvement was assessed between the 2 groups, statistical differences were apparent regarding graft success. For the TFT group, graft uptake was 82.9% and for the cartilage group, it was 97.1%. 21 In the study of Nithya et al where diced cartilage was used as a cartilage graft, graft uptake was 83% for TFT and 93% for the cartilage group. 22 This was 95% for the cartilage island graft group and 86.1% for the TFT in the study of Kalcioglu et al and 92% for the cartilage-perichondrium composite graft and 85% for TFT in the study of Sapci et al.23,24
Table 2 summarizes the results of the various studies comparing TFT and different types of cartilage tympanoplasties. As one can infer from the table, cartilage tympanoplasty is much more successful in study groups with larger perforations. This study demonstrated that reinforcing anterior annulus with conchal cartilage, improved the graft uptake success in TFT which is a disadvantage in large perforations.
List of Studies Comparing TFT with Different Types of Cartilage Tympanoplasties.
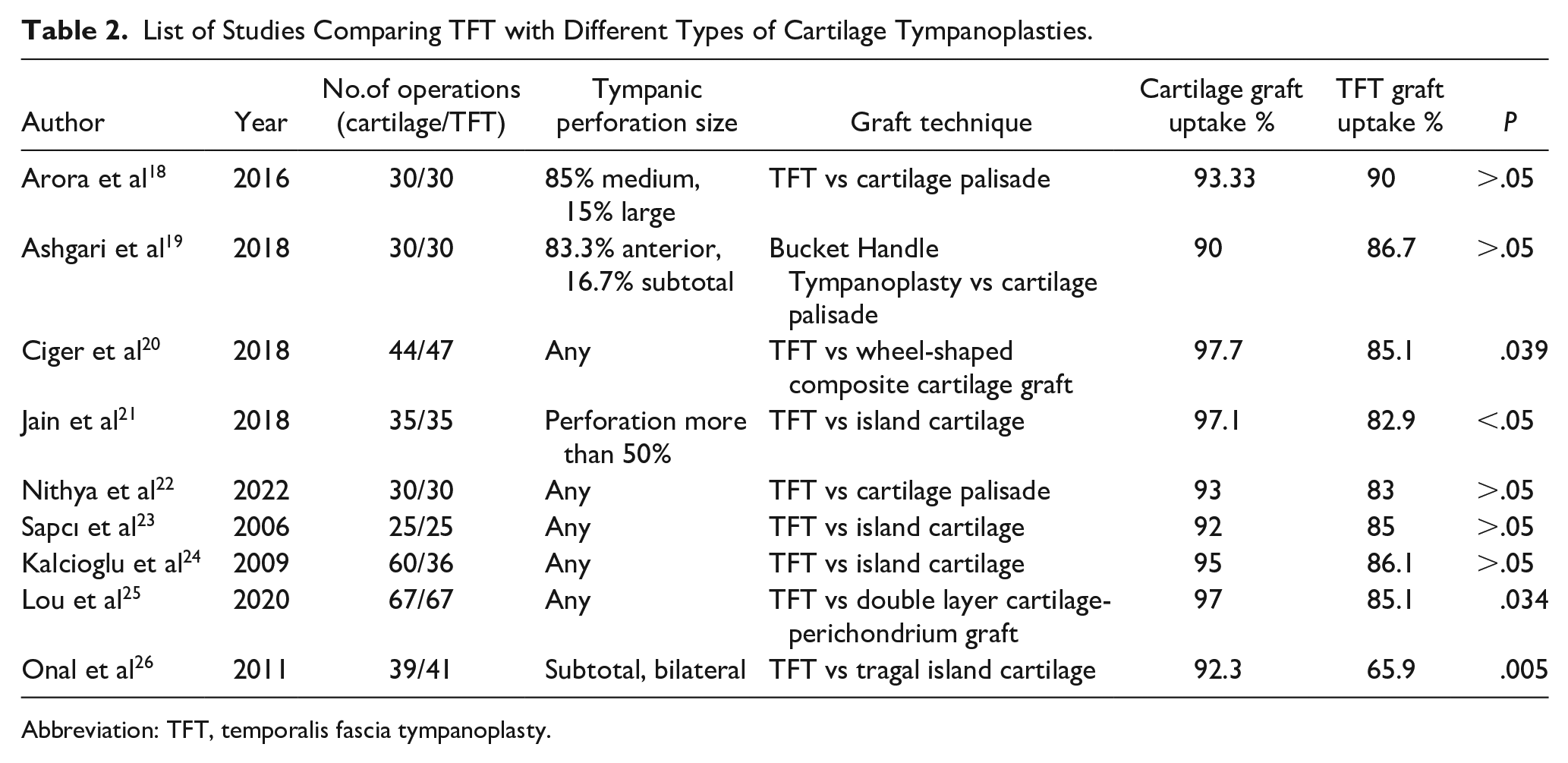
Abbreviation: TFT, temporalis fascia tympanoplasty.
Conclusion
Since the introduction of cartilage tympanoplasty, different methods have been used by various surgeons to optimize the tympanoplasty results. Cartilage harvest from conchal or tragal cartilage and combining temporal fascia and/or perichondrium have been evaluated for better surgical results. This study compared the results of the 2 tympanoplasty grafting techniques for subtotal and total tympanic membrane perforations. The popularity of temporalis fascia grafting has decreased as endoscopic operations became popular in ENT due to the bulkiness of the temporalis fascia as it becomes swollen after being introduced to the middle ear resulting in poor stability and medialization of the graft. Cartilage or perichondrium graft tympanoplasty gained popularity as the graft does not get swollen and is easy to manipulate after being placed in an over-underlay manner. Therefore, various techniques have been developed by various surgeons to overcome the disadvantages of TFT by placing the additional cartilage under the temporalis fascia to reduce the gap in between the anterior annulus and the graft. However, in these techniques it is hard to manipulate the cartilage under the fascia, which is usually displaced through the eustachian tube, causing medialization of the fascia. So, in this new technique, the additional cartilage or cartilages were placed over the fascia under the anterior annulus to stabilize the graft for especially subtotal and total perforations. The graft success and hearing improvement results were similar to the tragal cartilage island grafting technique. Our study group has a limited number of patients, as it consists of patients having only total and subtotal tympanic membrane perforations. More research is needed to compare these 2 tympanoplasty techniques with different sizes of tympanic membrane perforations.
Footnotes
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.