
Abstract
Objectives
To investigate the effects of titanium partial ossicular replacement prosthesis (PORP) and conchal cartilage for ossiculoplasty on hearing results in single-stage canal wall down (CWD) mastoidectomy surgery with type II tympanoplasty in patients with cholesteatoma.
Methods
The patients were performed surgeries for the first time by a senior otosurgeon from 2009 to 2022 and were performed CWD mastoidectomy with type II tympanoplasty in one stage were enrolled. Patients who could not be followed up were excluded. Titanium PORP or conchal cartilage was used for ossiculoplasty. When the stapes head was intact, a cartilage 1.2–1.5 mm thick was attached directly to the stapes; when the head of the stapes was eroded, a 1 mm high PORP and cartilage of .2–.5 mm thick were placed on the stapes simultaneously.
Results
148 patients were included in the study in total. The titanium PORP and conchal cartilage groups showed no statistically significant differences at 500, 1000, 2000, and 4000 Hz considering the number of decibels of closure of the air-bone gap (ABG) (P > .05) and pure-tone average ABG (PTA-ABG) (P > .05). Meanwhile, the closure of PTA-ABG between the 2 groups showed no statistically significant differences in the overall distribution (P > .05).
Conclusions
For patients with cholesteatoma and mobile stapes who underwent CWD mastoidectomy with type II tympanoplasty in one stage, either PORP or conchal cartilage is a satisfactory material for ossiculoplasty.
Introduction
The ultimate goal of cholesteatoma surgery is to eradicate the lesion, resulting in a dry and self-cleaning intraoperative cavity while improving or preserving auditory function. 1 Two main techniques in the treatment of cholesteatoma are canal wall up (CWU) and canal wall down (CWD) mastoidectomy. 2 The conventional view is that CWD mastoidectomy is the gold standard for obtaining a safe and dry cavity in cholesteatoma. 2 The purpose of ossiculoplasty is to restore the continuity of the ossicular chain and improve the sound conduction and impedance matching system with the integrated tympanic membrane. 3 Construction materials for ossiculoplasty can be categorized as allograft, homograft, and autograft materials, including partial ossicular replacement prostheses (PORP), total ossicular replacement prostheses (TORP), bone cement, hydroxyapatite, autologous bone interposition, and auricular cartilage.3–5 It has been reported that the state of the ossicular chain influences hearing outcomes the most.6,7
In this study, all patients were diagnosed with cholesteatoma and underwent CWD mastoidectomy with type II tympanoplasty in one stage; meanwhile, the ossicular chain was detected as mobile stapes with the presence of the suprastructure of the stapes. Titanium PORP or conchal cartilage was used for ossiculoplasty. Hearing results obtained after ossiculoplasty were compared between the titanium PORP group and auricular cartilage group. Previous studies have compared different reconstruction materials for ossiculoplasty in recent years, but rare study shows the results of one otosurgeon. For making the comparison more rigorous, we presented the outcomes by the same surgeon in this study.
Patients and Methods
Patients
A retrospective analysis was performed in patients with middle ear cholesteatoma in the department of otorhinolaryngology head and neck surgery in Xijing Hospital from 2009 to 2022, who underwent CWD mastoidectomy with type II tympanoplasty simultaneously using PORP (Spiggle, Germany) or auricle cartilage to reconstruct the ossicular chain. All included patients were primary cases, revision cases, and cases that could not be followed-up were excluded. Surgeries were performed by an experienced senior otosurgeon independently. All patients received pure tone audiometry, acoustic conductance, auditory brainstem evoked potentials, fiber otoendoscope, and temporal bone-thin layer computerized tomography (CT) before the operation. Written informed consent was obtained from all patients.
Surgical Technique
All patients received general anesthesia. When the anesthesia was successful, a retroauricular approach was performed, both transcortical and transmittal were advisable for gradual saucerization and deepening of the cavity. Bony overhangs were removed from the edges to obtain a round-shaped cavity. All air cells posterior to the mastoid segment of the facial nerve and the sigmoid sinus were removed and exteriorized. The sinodural angle was sufficiently removed and the facial ridge was evenly lowered by drilling the posterior canal wall. Finally, the shape of the cavity was saucerized with rounded external edges and no bony overhang in the cavity.
8
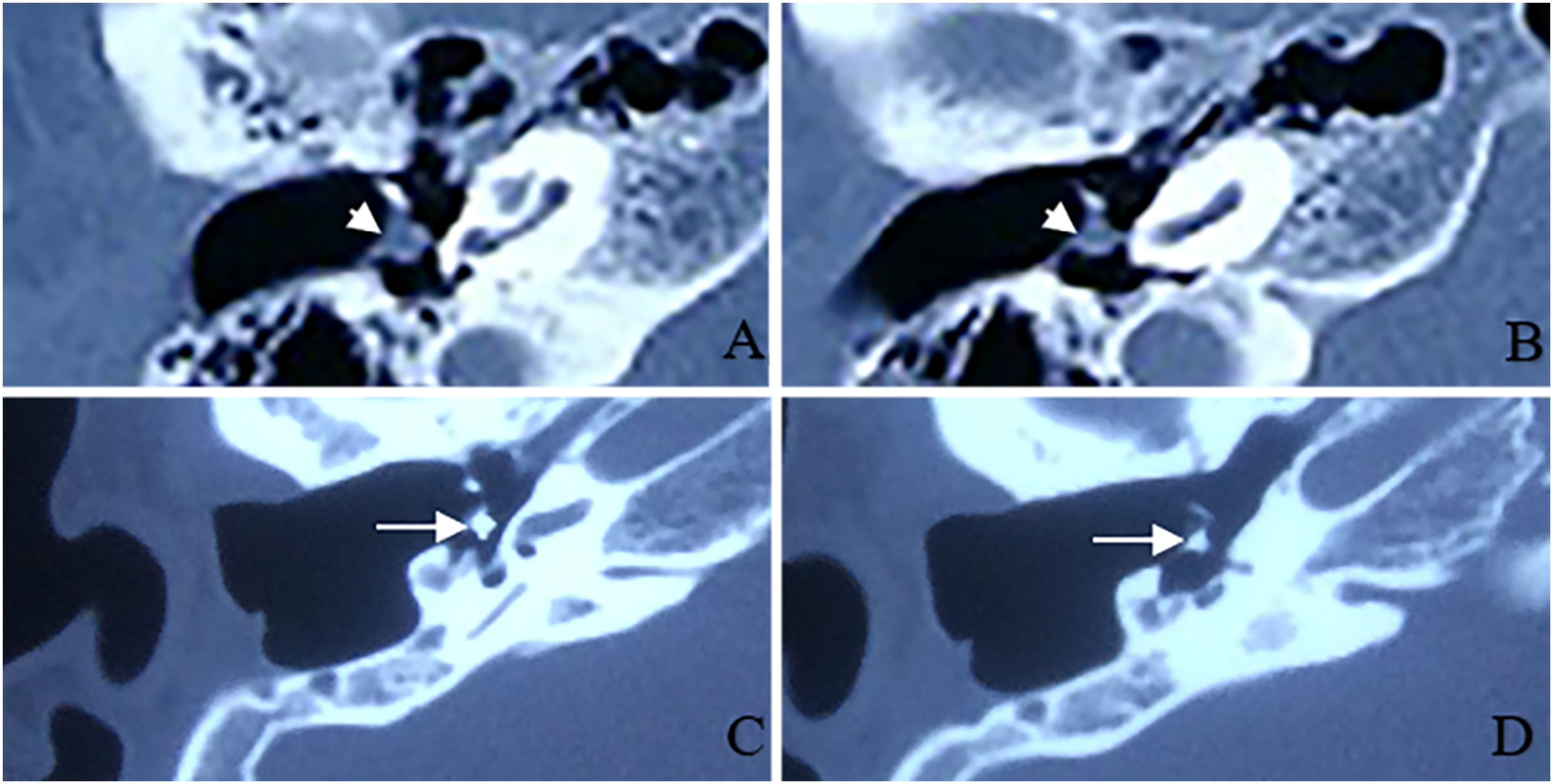
The conchal cartilage graft or PORP was used for ossiculoplasty, cartilage was harvested in the auricular concha. The thickness of the cartilage was measured by palpation and visual inspection and sculpted into an appropriate sheet with a scalpel. When the head of the stapes was intact, the cartilage with a thickness of 1.2–1.5 mm was preferred to heighten the stapes directly (Figure 1A), and when the head of the stapes was eroded, a PORP with a height of 1 mm was preferred and a thin cartilage disc of .2–.5 mm was added to it (Figure 1B). Figure 2 shows the temporal bone-thin layer CT scans of patients after the surgery. For patients with fistulas, a piece of temporal fascia was used to cover the fistula area. The bone pate, musculoskeletal flap, and cartilage were used for mastoid obligation and the temporal fascia underlay technique for myringoplasty. Conchoplasty was performed to enlarge the external acoustic meatus. The ear canal was obliterated with a gelatin sponge with antibiotics and was debrided after one month for the first time. Schematic of type II tympanoplasty with the CWD technique. Figure 1A shows that a thick conchal cartilage disc was interposed between the fascia graft and the stapes when the stapes head was intact. Figure 1B presents that a thin disc of conchal cartilage and PORP were interposed between the fascia graft and the stapes when the head of the stapes was eroded. TM: tympanic membrane; CWD: canal wall down, PORP: partial ossicular replacement prostheses. Temporal bone-thin layer CT scans after the surgery. Figure 2A–B show the CT scans of a thick conchal cartilage disc that was interposed between the fascia graft and the stapes at 4 months after surgery. Figure 2C–D present the CT scans of a PORP with a thin disc of conchal cartilage interposed between the fascia graft and the stape at 4 years after surgery. White arrowhead: a thick conchal cartilage disc; White arrow: a titanium PORP with a thin disc of conchal cartilage; PORP: partial ossicular replacement prostheses; CT: computerized tomography.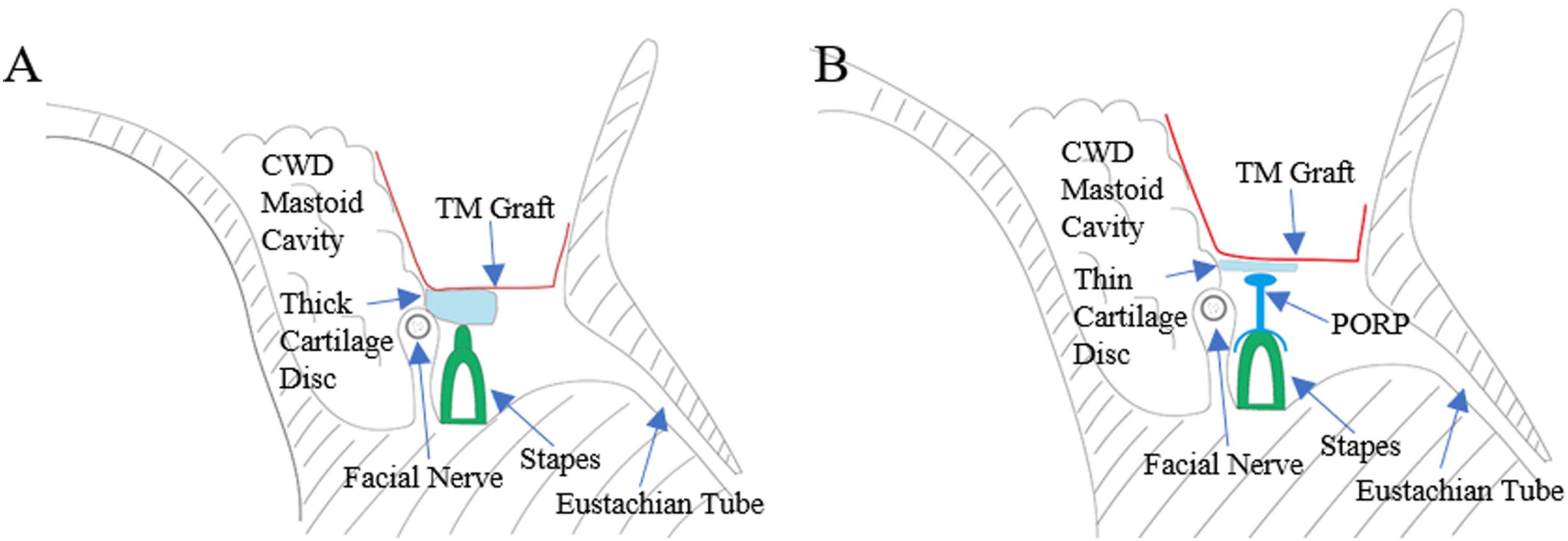
Hearing Tests
Pure tone audiometry was used for hearing tests, and thresholds were recorded at frequencies of 500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz.6,9 The preoperative and postoperative difference of ABG was calculated and the closure of ABG was compared. The number of decibels of ABG closure was determined as the preoperative ABG minus the postoperative ABG. 8 The audiological data used in this article are the preoperative hearing thresholds and the most recent postoperative hearing thresholds.
Statistical Analysis
All data are shown as mean ± SD (standard deviation) or quartiles. Continuous variables between 2 groups were compared with 2 independent sample t-tests, and paired samples were tested by the paired t-test. Mann-Whitney U tests were performed for independent nonparametric samples, respectively. Categorical variables were determined using the Chi-square test. SPSS 17.0 software was used to calculate the statistical results. Statistical significance was defined as P < .05.
Results
Demographic and Clinical Characteristics
Demographic and Clinical Data of the Patients.
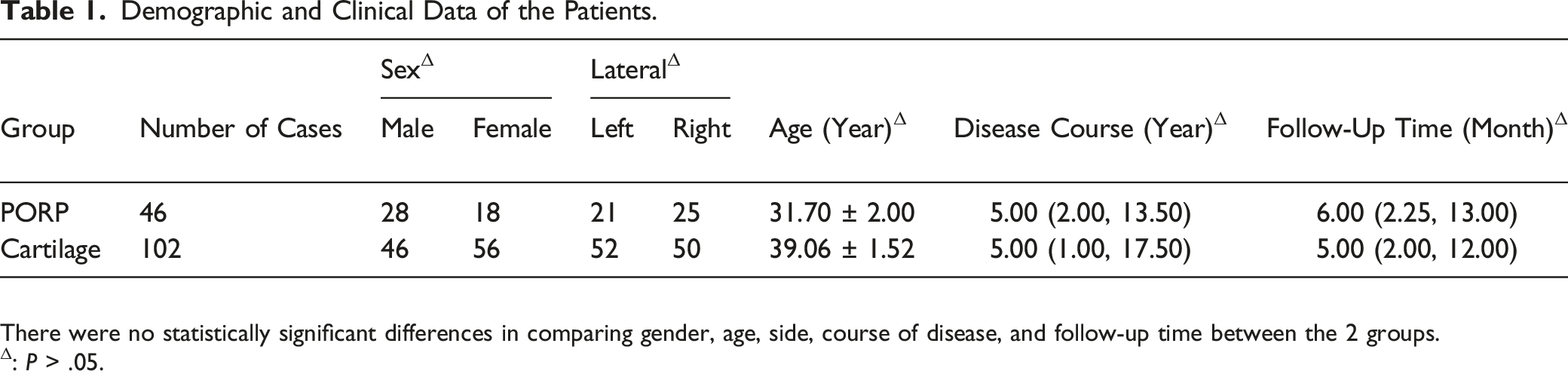
There were no statistically significant differences in comparing gender, age, side, course of disease, and follow-up time between the 2 groups.
Δ: P > .05.
Preoperative and Postoperative ABG
Comparison of ABG between PORP and Cartilage Groups.
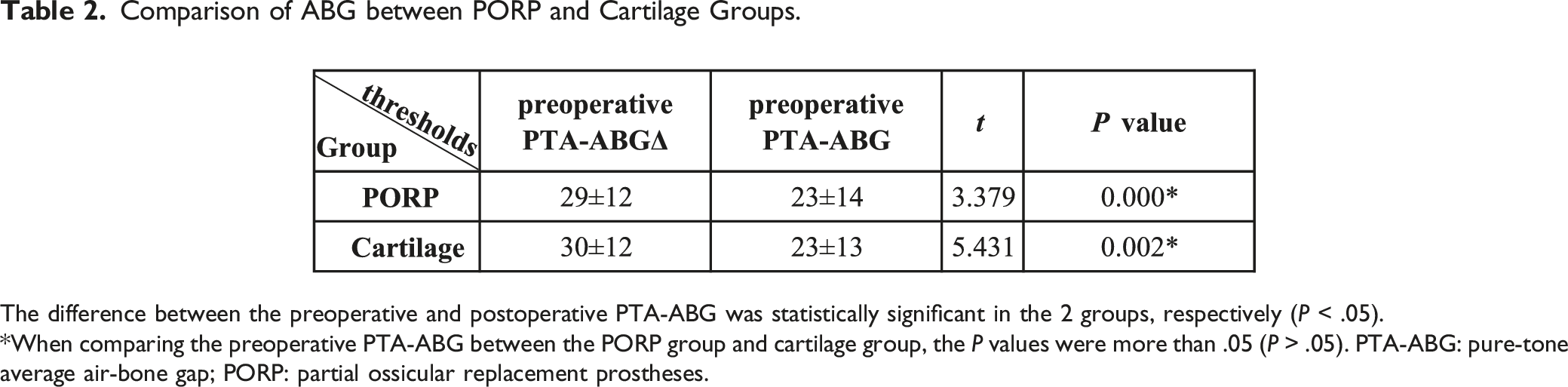
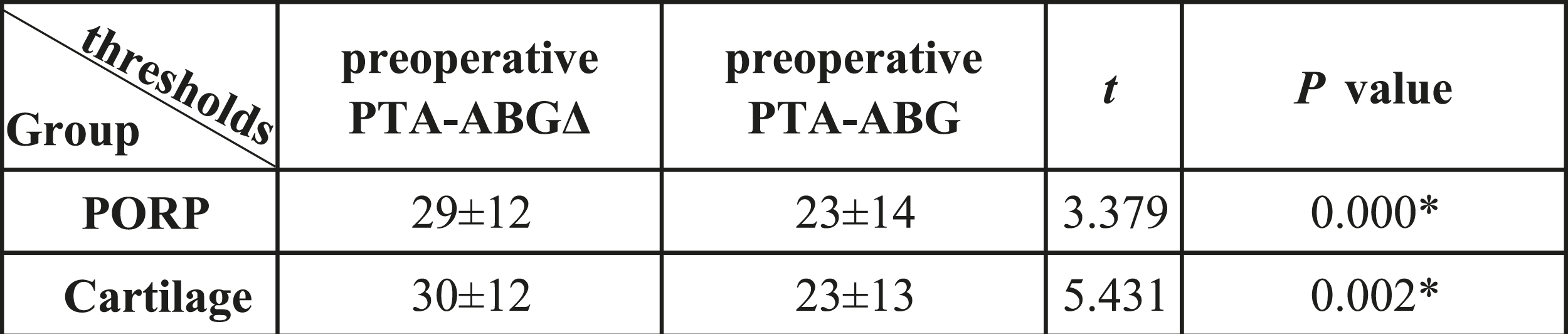
The difference between the preoperative and postoperative PTA-ABG was statistically significant in the 2 groups, respectively (P < .05).
*When comparing the preoperative PTA-ABG between the PORP group and cartilage group, the P values were more than .05 (P > .05). PTA-ABG: pure-tone average air-bone gap; PORP: partial ossicular replacement prostheses.
ABG Closure
Comparison of ABG Closure between PORP and Cartilage Groups.
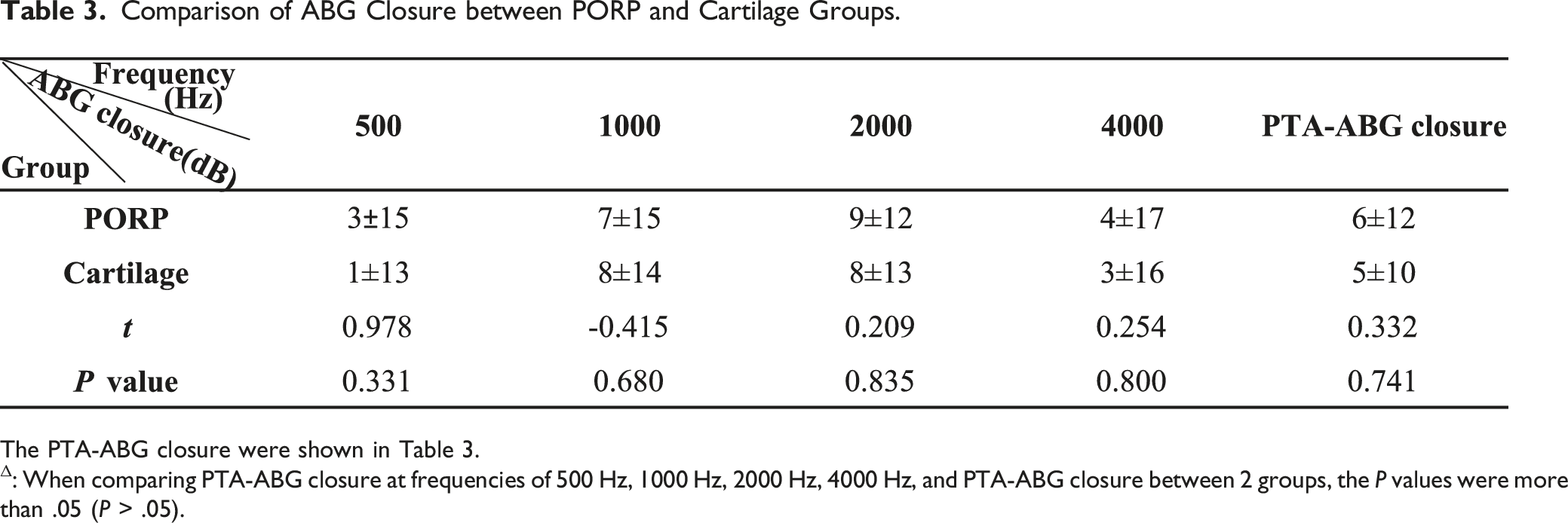
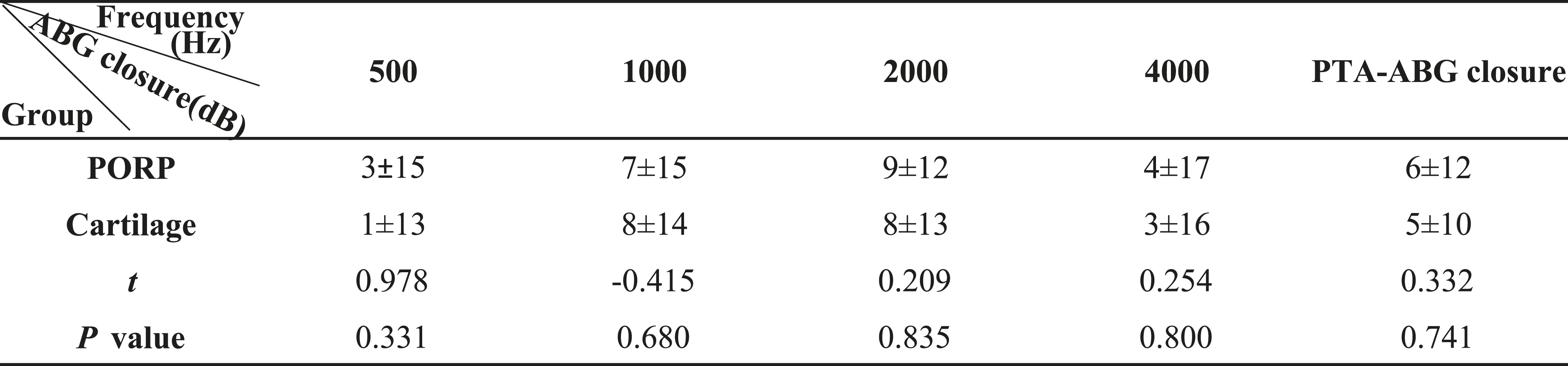
The PTA-ABG closure were shown in Table 3.
Δ: When comparing PTA-ABG closure at frequencies of 500 Hz, 1000 Hz, 2000 Hz, 4000 Hz, and PTA-ABG closure between 2 groups, the P values were more than .05 (P > .05).
Distribution of PTA-ABG Closure.
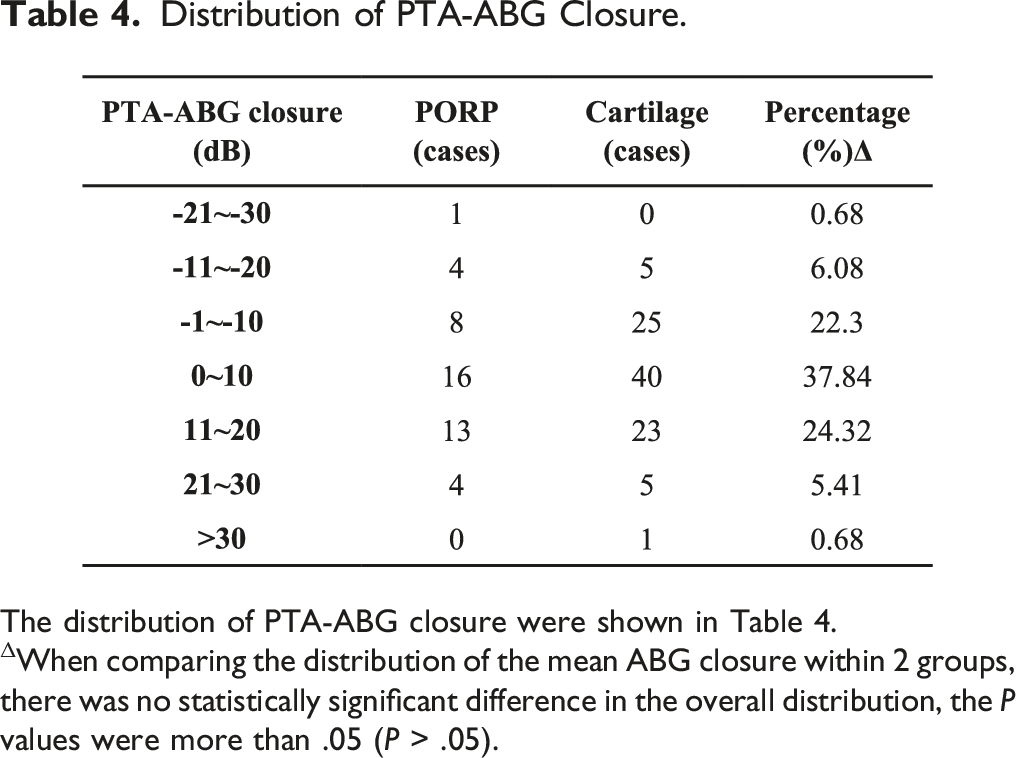
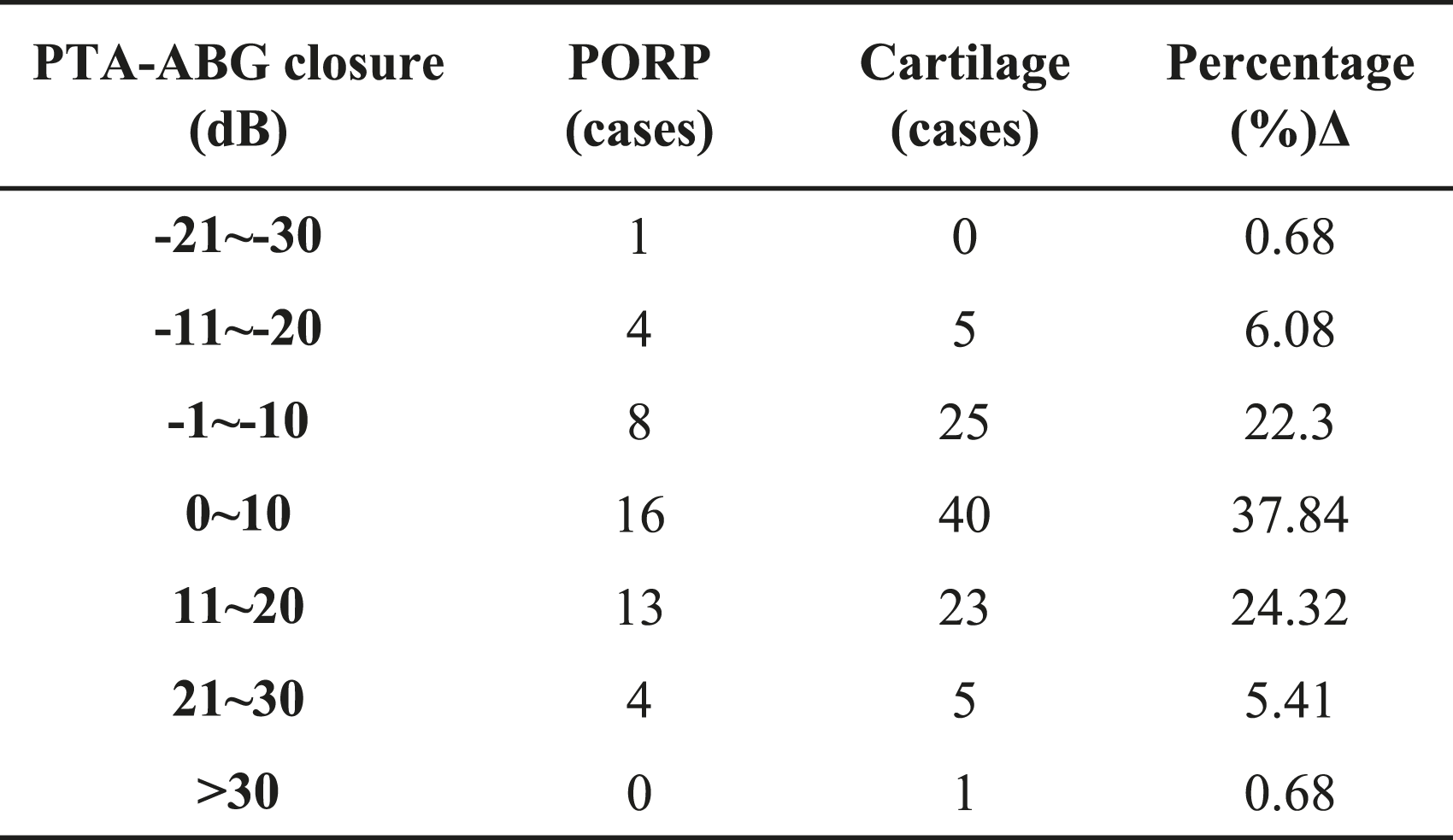
The distribution of PTA-ABG closure were shown in Table 4.
ΔWhen comparing the distribution of the mean ABG closure within 2 groups, there was no statistically significant difference in the overall distribution, the P values were more than .05 (P > .05).
Discussion
Cholesteatoma is one of the most severe and common diseases in the ear. It is a cystic lesion formed from a stratified keratinizing squamous epithelium, and is commonly characterized as “skin in the wrong place,”10–12 which can cause otorrhea, hearing loss, and severe intra- or extra-cranial complications. 13 Ossicular erosion and bone erosion are generally observed under the epithelium. 14 The disease can be classified as congenital or acquired disease. 2 Since there is no non-surgical treatment for cholesteatoma, 15 CWU and CWD mastoidectomy are the primary techniques to eradicate cholesteatoma. Since CWU mastoidectomy has a higher percentage of recurrence, 2 some surgeons mainly apply CWD techniques in cholesteatoma to achieve a well-functioning CWD cavity with minimal hearing loss and quality of life and to avoid the second operation. 8 The main disadvantage of CWD mastoidectomy is that externalization of the mastoid creates a cavity, which accumulates debris and usually requires continuous debridement. Protruding edges, high facial ridges, or prominent mastoids can hinder the self-cleansing of cerumen and cavity debris. 8
Hearing rehabilitation should lead to a stable, predictable, symmetric, and as close to the average hearing threshold as possible. Previous studies have shown that CWD mastoidectomy with ossiculoplasty in one stage can simultaneously reduce the difference of ABG in the affected ears, identifying the need to reconstruct the ossicular chain.16–18 Complications associated with ossiculoplasty include displacement of the prosthesis, the need for subsequent surgery, the insertion of a secondary ventilation tube, the formation of extensive scar tissue, and recurrence of perforation. 19 Our study showed that 2 patients had perforations of the tympanic membrane, one in the PORP group got reperforation at 4 years post-surgery; the other in the cartilage group got reperforation at 2 months post-surgery. The hearing results may vary widely due to different factors of the surgeon. 20 Previous studies have shown that ossicular chain factors have the most significant influence on postoperative hearing.7,20,21 In this study, the status of the ossicular chain was the mobile stapes floor and the existence of the superstructure of the stapes. On this basis, ossicular chain reconstruction and CWD tympanoplasty were performed independently by an experienced otosurgeon in microscopic surgery. Rare studies had conducted and compared the results of the same surgeon. Therefore, the preoperative and postoperative hearing comparison had more clinical value in this study by excluding the different factors of the surgeon.
Since the incudostapedial joint is a non-weight bearing, 22 the reconstructive materials should be flexible enough. Luca compared titanium and hydroxyapatite ossiculoplasty in CWD mastoidectomy and showed that titanium was a satisfactory material for ossicular reconstruction and is equal to hydroxyapatite. 1 Gautam demonstrated that cartilage-based ossiculoplasty was an effective way to improve hearing. 23 Anindita showed a marked improvement after CWD mastoidectomy with ossiculoplasty in a prospective study. 24 Burton proved that patients who underwent tympanoplasty with stapes columella grafting in CWD mastoidectomy yield marginal hearing benefits. In this tympanoplasty technique, cartilage or other tissue was placed directly onto the head of the stapes. 25 Although no material has been demonstrated to generate better hearing results than others, the search for a perfect material to maintain ossicular continuity is evolutionary. 3
When the stapes head was intact, either a PORP or cartilage would be suitable for ossiculoplasty in CWD mastoidectomy with type II tympanoplasty. Based on our experience, both PORPs and cartilage are suitable for the amplification effect of the ossicle, this study showed comparable hearing results between PORPs and cartilage. We preferred to choose cartilage when the stapes head was intact for the following reasons: (1) cartilage is cost-effective for it is free, while a PORP costs more when obtaining a comparable hearing improvement; (2) autologous cartilage has better biocompatibility, while PORPs have the risk of extrusion; 19 and (3) for patients who might need a high-field MRI test in the future, the patients with PORPs might be anxious about the risk for undergoing a high-field MRI test. Some patients refused to use PORPs and informed refusal was documented before the operation. When the stapes head was eroded, a PORP was preferred to heighten the ossicle, preventing cartilage from adhesion to promontory and impairment of hearing level. Figure 2 shows the temporal bone-thin layer CT scans of patients after the surgery, which revealed the position of the thick disc of cartilage (Figure 2A-B) and a PORP with a thin disc of cartilage (Figure 2C-D) in the reconstructed ossicular chain.
The study showed a recidivism rate of 2.7% (4/148), which corresponded to the reported recidivism rate of the CWD technique (0–13.2%). 2 From the surgeon's point of view, CWD mastoidectomy is more friendly for novice otosurgeons, with better visual field exposure, more conducive to the thorough eradication of lesions to reduce the risk of recurrence. CWU mastoidectomy is more suitable for experienced ear surgeons due to poor visual field exposure and a higher risk of residual cholesteatoma and recurrence rate (16.7–61%). 2 Although hearing improvement is the secondary goal for cholesteatoma surgery, patients desire an improved hearing result, not only eradicating the disease for a dry and self-cleansing ear, thus, making our work more challenging. For this reason, the study searching for a perfect material for the maintenance of ossicular continuity is entirely meaningful to obtaining satisfactory hearing results.
It is positively necessary to perform an ossiculoplasty after CWD mastoidectomy, nearly 70% of the patients achieve closure of the PTA-ABG in the study. For patients with cholesteatoma and flexible stapes with suprastructure of the stapes who underwent CWD mastoidectomy with tympanoplasty at one stage, the closure of PTA-ABG showed no statistically significant difference between the PORP and cartilage groups, therefore either is a satisfactory material for ossiculoplasty after performing CWD mastoidectomy, the surgeon can choose one according to the need of the patients, the status of stapes heads, or whether a PORP is acceptable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the National Natural Science Foundation of China, grant number 82171161 (Recipient: ZDJ), 82103627 (Recipient: QWZ). They all authored or reviewed drafts of the paper and the Natural Science Foundation of Shaanxi, grant number 2020JZ32 (Recipient: Juan Qu)
Ethical Approval
This study was approved by the Ethics Committee of the Xijing Hospital (Reference number to the ethical application: KY2022082), and the written approval was waived.
Data Availability
The datasets used or analyzed during the current study are available from the corresponding author on a reasonable request.