
Abstract
Introduction
Albrecht von Haller, a Swiss anatomist, first described Haller cells in 1765 and subsequently named after him. Infraorbital ethmoid air cells (Haller cells) have been defined as an anterior or posterior ethmoidal air cell that develops into the orbital floor, where it can narrow the adjacent maxillary sinus ostium or infundibulum. 1 It may be defined as any ethmoidal cell which pneumatizes inferior to the orbital floor and lateral to a line parallel with the lamina papyracea.1,2 There are a lot of synonyms for these specific cells, they were called in the past either orbit-related ethmoidal air cells or maxilla-related ethmoidal air cells because they are related to the anatomical position of either the orbit or maxillary sinus. Therefore, it was named as maxilla-ethmoidal or orbito-ethmoidal air cells. The name infraorbital ethmoidal air cell (IOEAc) is proposed to describe the site and origin. IOEAc may be different in size, number, and shape. Haller cells are defined as air cells situated beneath the ethmoid bulla along the roof of the maxillary sinus and the most inferior portion of the lamina papyracea, including air cells located within the ethmoid infundibulum. 3
An awareness of the anatomical variations of the IOEAc is important for clinical practice, together with its relationship to associated rhinosinusitis. In addition, it can be solitary involved in inflammation and subsequently affects surrounding structures including the orbit. It has implications for preoperative planning and is important in selecting the most appropriate approach during endoscopic sinus surgery to reach lesions in the maxillary sinus safely without orbital penetration. Such anatomical variation influences a variety of intraoperative factors which determine patient’s outcome and increases the risk of misinterpretation and surgical error. Despite this, there is a lack of consensus in the literature on a system that comprehensively documents and classifies such variations. 4 Detection of IOEAc may also forewarn the surgeons prior to endonasal procedures, thus preventing any untoward intraoperative complications. Therefore, this study aimed to identify and categorize the anatomical variations of the IOEAc to produce a new and comprehensive classification system.
Materials and Methods
This study was an observational cross-sectional study that included computed tomography (CT) scans of the nose and paranasal sinuses of 1365 patients retrieved from the recording systems of Otorhinolaryngology and Diagnostic Radiology departments. All these patients who had these scans presented with chronic or recurrent headache with or without nasal obstruction. The study was carried out after the approval of the institutional review board. Patients younger than 18 years, suspected trauma or malignancy, or with known surgical intervention in the midface region were excluded. CT scans with partially reconstructed images and artifacts that compromised the diagnostic quality of the scans were also excluded. A set of 105 scans were excluded from the study because it did not meet the inclusion criteria.
The remaining 1260 scans included in the study were done using a multidetecting computed tomography scanner (Somatom-Siemens, Berlin, Germany), using a dedicated paranasal sinuses protocol. The scans were evaluated for the presence and extension of IOEAc in relation to the infundibulum and inferior orbital wall. The bilaterality, shape of IOEAc (ovoid, oblong, or rounded) according to its dimensions, and their numbers (single or multiple) were recorded. The size and the 2 maximum perpendicular dimensions in the coronal view of IOEAc were calculated. Ventilation of the IOEAcl were recorded from the infundibulum, bulla ethmoidalis, or the maxillary sinus, and the relationship of the IOEAc to the maxillary ostium and bulla ethmoidalis, if applicable.
Each scan was analyzed twice, once by the senior otorhinolayngologist and another by the senior radiologist involved in the study (both with more than 20 years of experience). Assessors were blinded to the cases. The scans were reviewed electronically on the picture archiving and communication system. Images consisted of standard axial, coronal, and sagittal images on CT. The interobserver agreement between the 2 observers was measured using a Cohans kappa that with its result ranged from 0 to 1.
The primary outcome of the study was the proposal of a new classification system for IOEAc according to the number of these cells and/or the extent of these cells involving either uncinated process superiorly or infraorbital nerve inferiorly. The secondary outcome of the study was the correlation between different parameters of IOEAc, such as number, dimensions, and shape, on the one hand, and this classification system on the other hand.
The study data were collected and analyzed using a version 26 statistical package for social sciences software (SPSS; IBM Corp., Armonk, NY, USA). Quantitative variables were expressed as numbers and percentages. Qualitative variables were expressed as mean and standard deviation. F-test (ANOVA test) was used for normally distributed quantitative variables, to compare between more than 2 groups. Chi-square test (X2) was used for categorical variables, to compare between different groups. A P value less than .05 was considered statistically significant. While the P value less than .001 was considered highly significant. All authors accept data sharing according to Wiley’s data sharing policy.
Results
In this study, the included 1260 included scans showed that 173 patients (13.7%) patients had IOEAc. Bilateral IOEAs were observed in 99 patients (57.2%), while 50 patients (28.9%) had unilateral right air cells and 24 patients (13.9%) had unilateral left air cells. According to the relation of the IOEAc to the inferior orbital wall and the maxillary infundibulum, a classification with 5 types was proposed as demonstrated in (Figures 1-3).
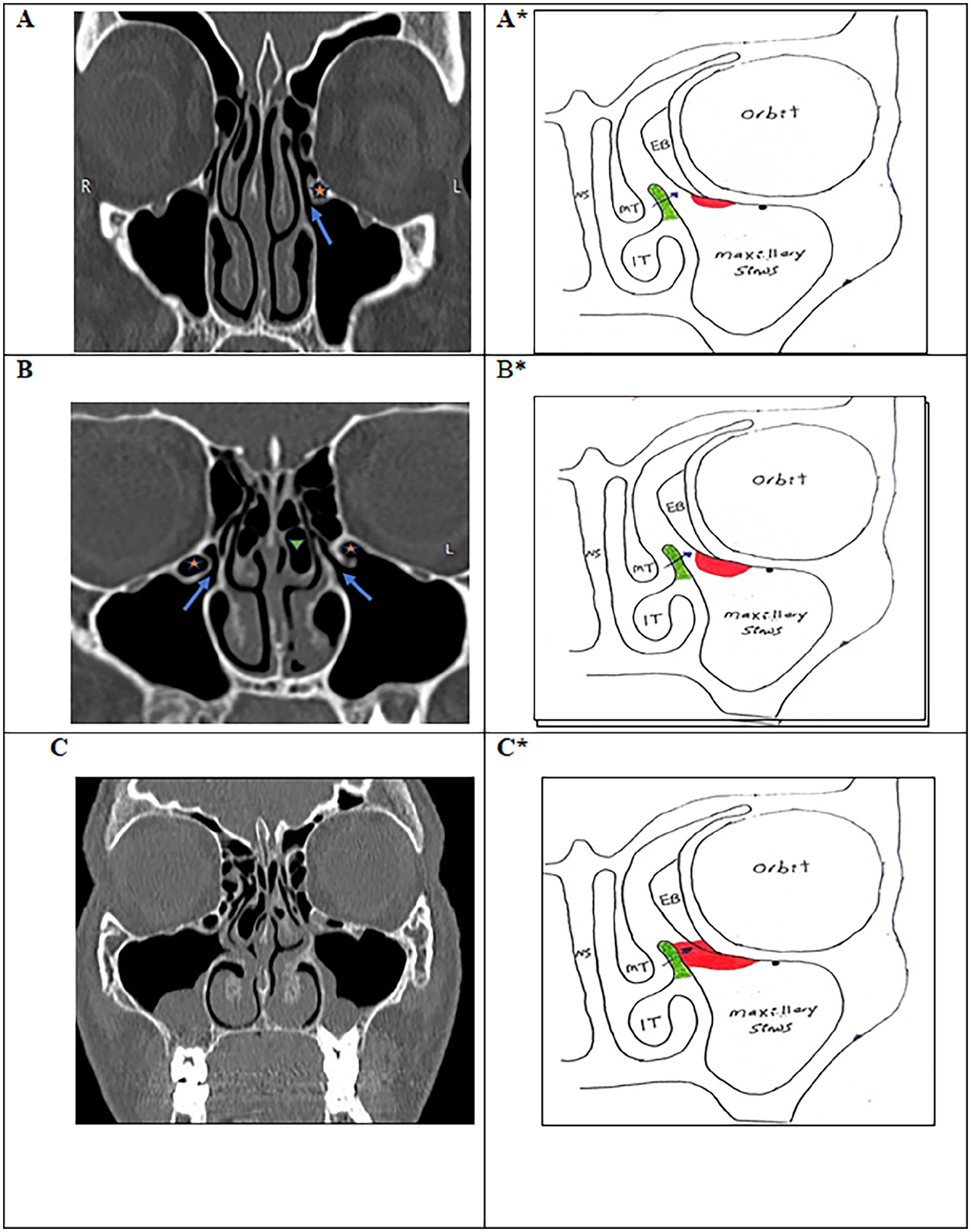
Type I IOEAc (localized infundibulo-orbitoethmoidal air cells): (A, B, C) CT and (A*, B*, C*) drawing of the nose and paranasal sinuses showing: A, A*: Type Ia: small air cell not reaching to the uncinate process (less than 1/2 the distance between the uncinate process and infero medial wall of the orbit) (Arrow: Infundibulum, Asterisk: IOEAc). B and B*: Type Ib: large not impacted to the uncinate process (more than 1/2 the distance between the uncinate process and infero medial wall of the orbit) (Arrow: Infundibulum, Asterisk: IOEAc). C and C* Type Ic: IOEAc impacted to the uncinate process. IOEAc, infraorbital ethmoidal air cells; CT, computed tomography.
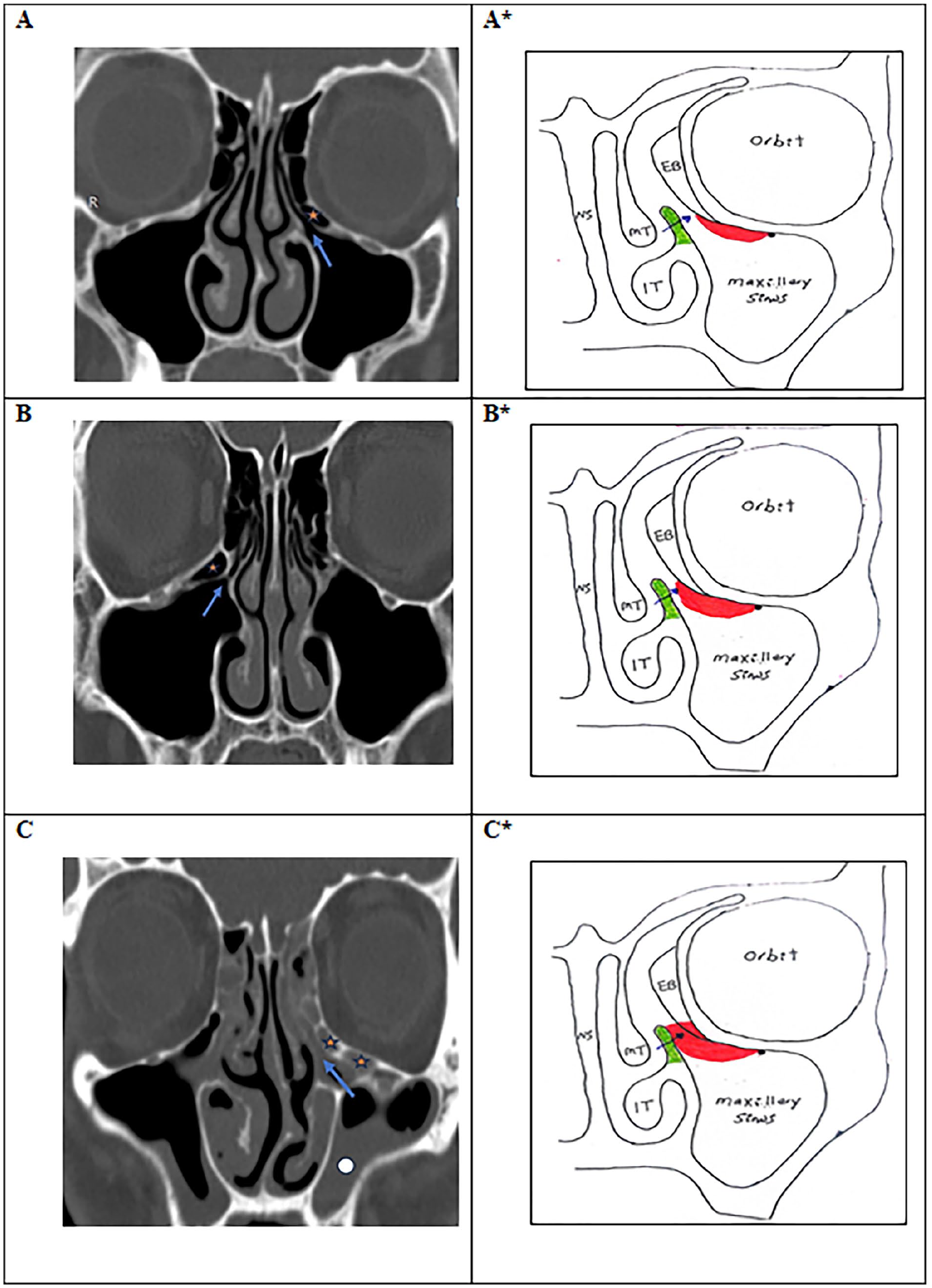
Type II IOEAc (Expanded infundibular orbitoethmoidal air cells): (A, B, C) CT and (A*, B*, C*) drawing of the nose and paranasal sinuses showing: A, A*: Type IIa: small not reaching to the uncinate process (less than 1/2 the distance between the uncinate process and infero medial wall of the orbit (Arrow: Infundibulum, Asterisk: IOEAc). B& B*. Type IIb: large not impacted to the uncinate process (more than 1/2 the distance between the uncinate process and infero medial wall of the orbit. Rt IIb IOEAc (single) (Arrow: Infundibulum, Asterisk: IOEAc). C &C*: Type IIc: Large impacted air cell to the uncinate process with associated maxillary sinusitis (Arrow: Infundibulum, Asterisk: IOEAc). IOEAc, infraorbital ethmoidal air cells; CT, computed tomography.
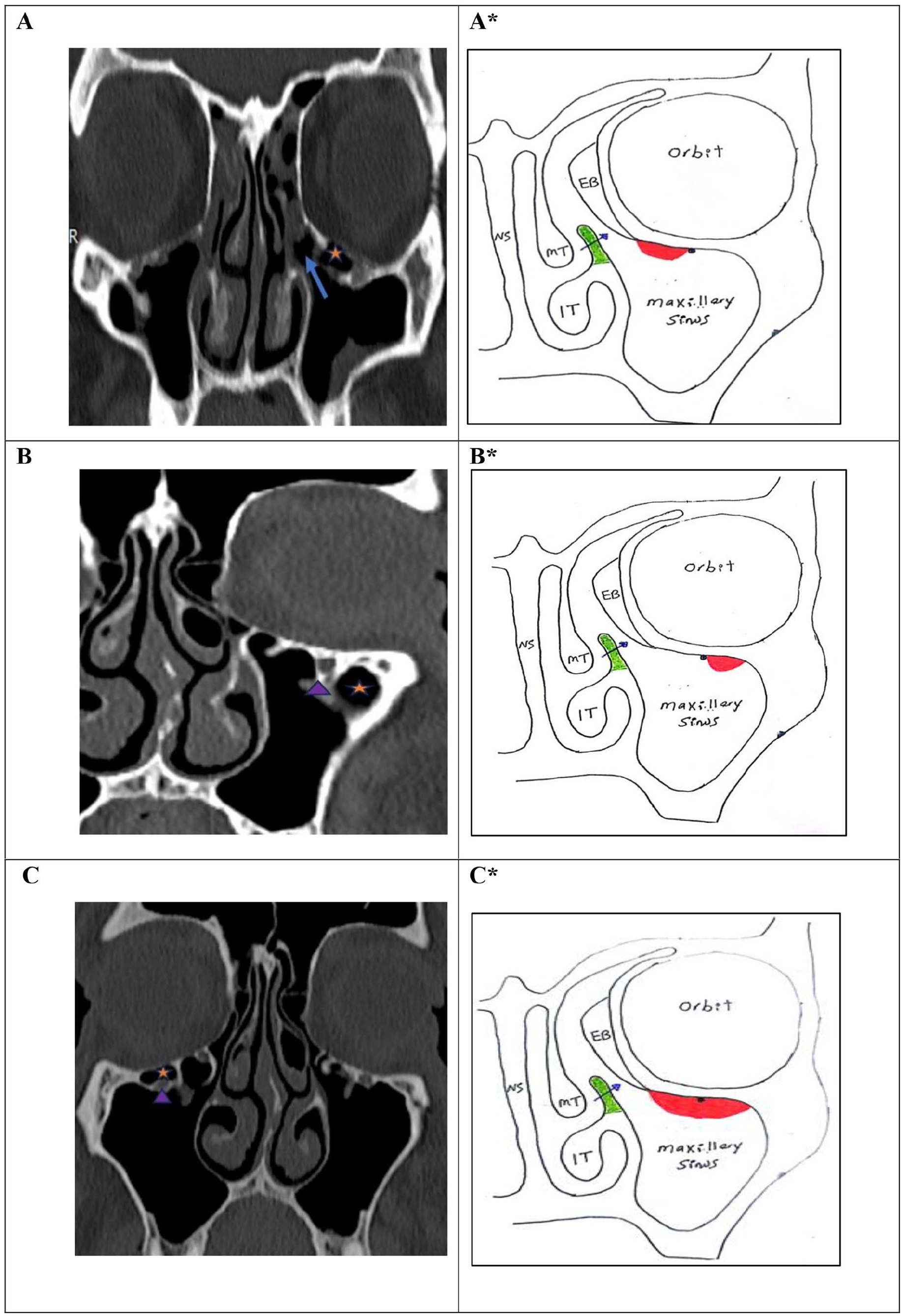
IOEAc (A, B, C) CT and (A*, B*, C*) drawing of the nose and paranasal sinuses showing: A, A*: Type III: noninfundibular orbitoethmoidal air cells lie at the inferior orbital lateral to the infundibulam and medial to the inferior orbital canal (Arrow: Infundibulum, Asterisk: IOEAc). B, B*: Type IV: noninfundibular orbitoethmoidal air cells lie lateral to the inferior orbital canal (Arrow head: Infraorbital canal, Asterisk: IOEAc). C, C*: Type V: noninfundibular orbitoethmoidal air cells lie lateral to the infundibulum and involve the whole floor of the orbit, medial and lateral to infraorbital canal (Arrow head: Infraorbital canal, Asterisk: IOEAc). IOEAc, infraorbital ethmoidal air cells; CT, computed tomography.
There was no significant relationship between IOEAc classification and their number, IOEAc being single in 153 cases (88.4%, P = .326) (Table 1). With respect to the size of IOEAc, the vertical and horizontal dimensions that were significantly increased among patients with Type V classification than other types of IOEAc (P < .0001) (Table 2).
Relation Between Classification of IOEAc and Frequency Number (N = 173).
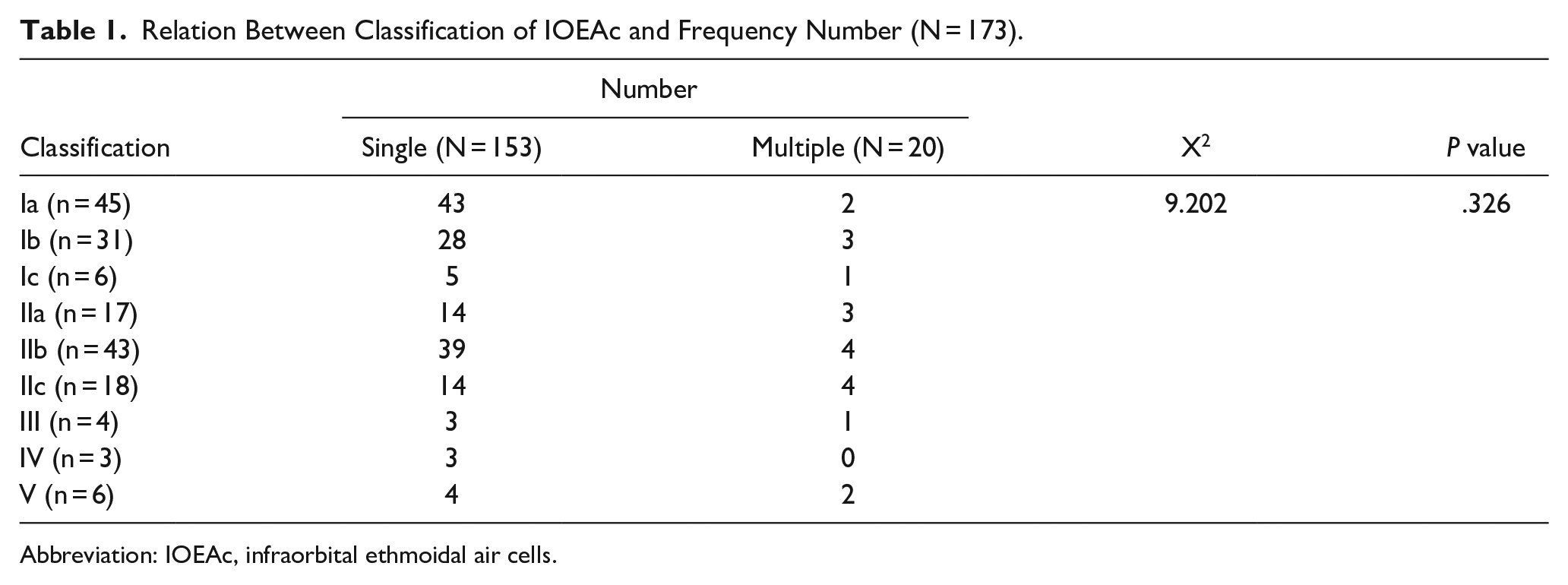
Abbreviation: IOEAc, infraorbital ethmoidal air cells.
Relation Between Classification of IOEAc and Dimension 1 (N = 173).
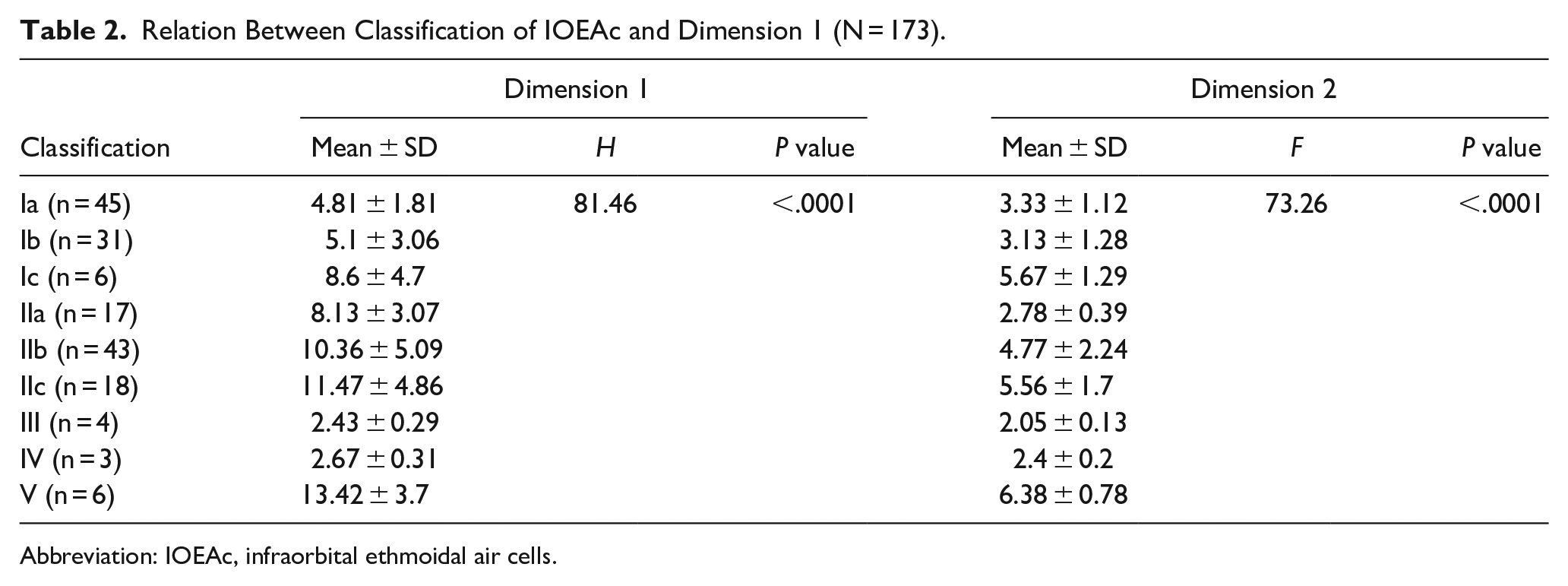
Abbreviation: IOEAc, infraorbital ethmoidal air cells.
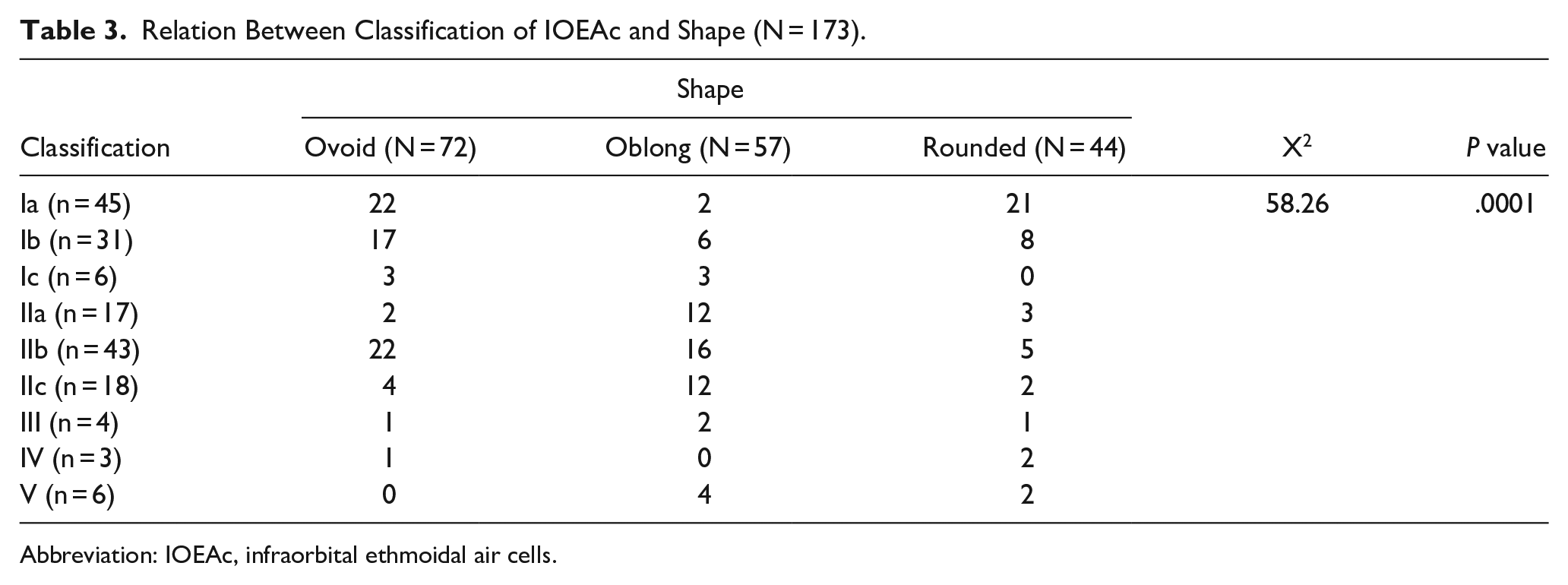
There were 3 common shapes (ovoid, oblong, and rounded); ovoid shape was the most common among patients with classification Ia, Ib, and IIb, also, oblong shape was the most common among patients with classification IIc, IIa, and V. However, rounded shape was the most common among patients with classification Ic, III, and IV. There was a significant difference between the different classifications and the shape pf IOEAc (P = .0001) (Table 3).
Relation Between Classification of IOEAc and Shape (N = 173).
Abbreviation: IOEAc, infraorbital ethmoidal air cells.
Discussion
The new classification system we have proposed in Table 4 has several advantages. In addition to containing more distinct variations and types of variation, it demonstrates greater potential for the categorizations of IOEAc identified in future studies. The grouping of such cells can allow users to select a variation type and its relationship to the orbit and maxillary sinus, while subgroups allow physicians to methodically identify and categorize its relations to the maxillary infundibulum. Overall, the new classification system provides a more comprehensive summary of the anatomical variations of IOEAc in humans, increasing the simplicity, flexibility, and efficiency of categorization and improving the precision of the IOEAc ontology.
Classification of IOEAc.
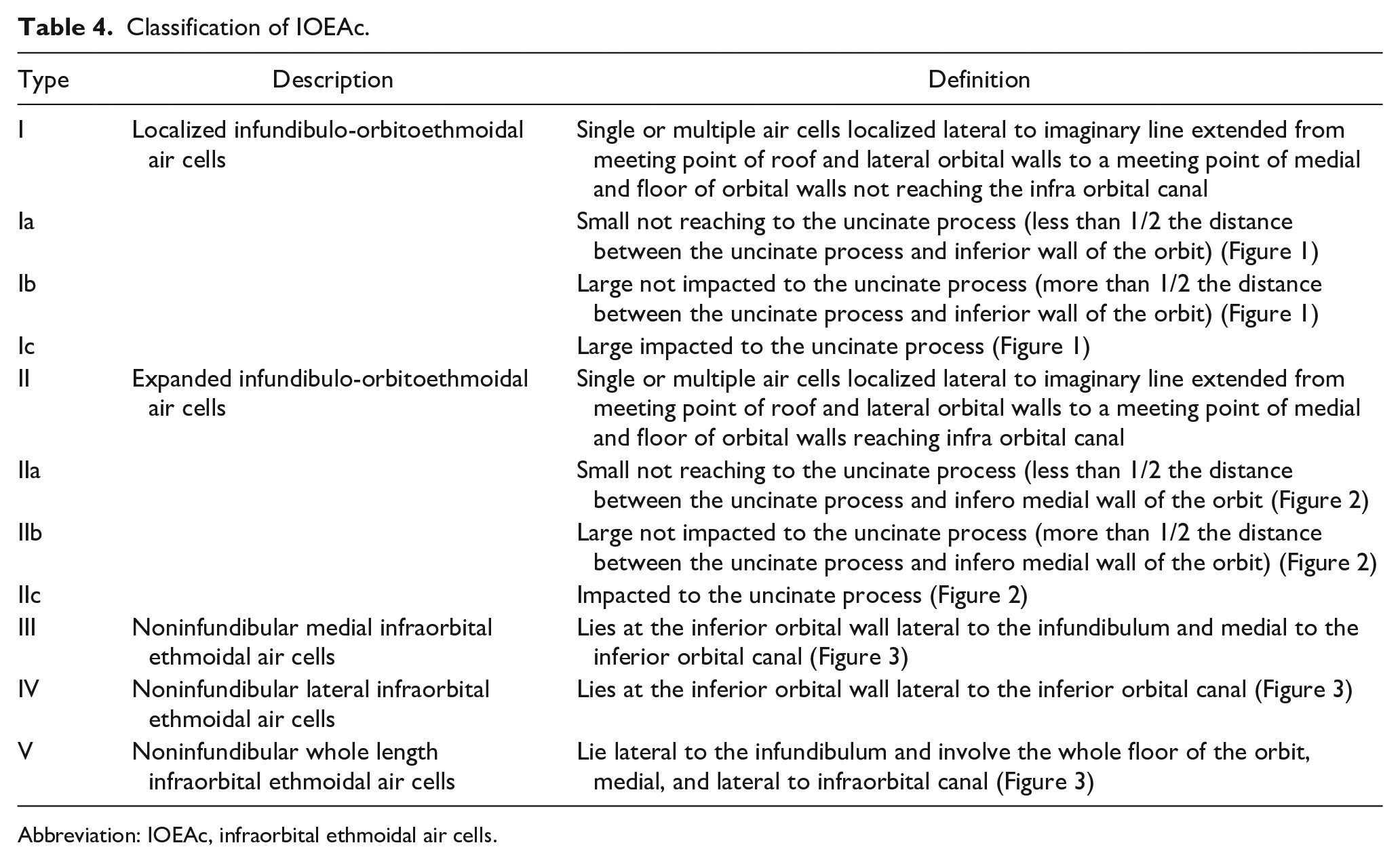
Abbreviation: IOEAc, infraorbital ethmoidal air cells.
The prevalence of IOEAc in this study was (13.7%). Several studies identified a prevalence of IOEAc between 6% and 16%.5-19 On the contrary, other studies reported a higher prevalence of IOEAc ranging between 42.6% and 56.6%.20-23 In this study, most of the patients were males (62.3%). This matches the findings of other studies, which found that most of the identified gender was also male (52.89%-64.80%).10,18,24-26 On the other hand, Solanki et al 27 and Khojastepour et al 24 had most of their patients as female (54.2%, 70.6%, respectively). In this study and in other studies IOEAc were mostly bilateral (57.1%), which matches the findings of other studies that reported an incidence of bilaterality ranging between 50% and 71%.10,24,28-30 Unilocular forms were the most common in the present study (88.4%) matching other studies including. Chaudhari et al 10 ; reporting an incidence of 93.3%, and Kumar et al 31 reporting an incidence of 80.4%. This could be explained by the differences between studies related to genetic predisposition in different countries as these studies were presented in different nations.
The current study showed that with respect to morphology, the incidence of oval shape was 41.6%, making it the most common morphology of IOEAc. While, the incidence of oblong shape was 32.9%, and the incidence of rounded shape was 25.5%. The ovoid shape was the most common among patients with classification Ia, Ib, and IIb; also, oblong shape was the most common among patients with classification IIc, IIa, and V. However, the rounded shape was the most common among patients with classification Ic, III, and IV.
Our study was close to the studies obtained by Solanki et al 27 ; Raina et al 19 who found that the prevalence of oval shape was (47.4%, 50%, respectively). On the other hand, Manaj et al, 32 Chaudhari et al, 10 and Kamdi et al 26 found that prevalence of oval shape more than the present study (80%, 53%, and 51.85%, respectively). However, Kumar et al 31 reported a lower incidence of the oval shape than the current result (21.8%).
Furthermore, this study was in agreement with the studies obtained by Solanki et al 27 and Kumar et al 31 who found that the prevalence of round shape was (21.4%, 29.3%, respectively). On the contrary, Raina et al, 19 Chaudhari et al, 10 and Kamdi et al 26 found that the prevalence of round shape in their study was more than in our study (47.90%, 46.60%, 38.51%, respectively).
There was no definite classification detected previously for IOEAc. So that, this study contributes to introduction of a new classification system of IOEAc, which might be considered a significant advancement. This classification system contributes to the existing knowledge by providing a more refined and detailed categorization of these cells based on their morphology and location. This new classification could potentially offer a more accurate and clinically relevant way of describing and understanding IOEAc variations, which help medical professionals diagnose and manage related conditions.
IOEAc is one of anatomical variants that can affect the patency of the osteomeatal complex according to their type, size, and shape which further lead to blockage of many sinuses drainage pathway, which may result in inadequate sinus ventilation that may lead to vacuum or pressure headache. These types of headache are mostly presented at forehead followed by the periorbital area. This association of IOEAc in maxillary sinus pathology was also observed by authors in the past from 1991 to till date where different imaging modalities were used.21,26,33
This new classification should be studied by rhinologist, in our opinion, before the endoscopic sinus surgery to finalize the operation without any complications. This classification is very important as frontal cells classification to detect the extent of the problem and the percentage of any possible recurrence of the infection or sinonasal polyps.
There were many limitations of the study, such as this study has retrospective design and the potential for selection bias that was solved by fixation of the observer. More number of patients with more number of rhinogenic patients are needed for further studies to detect the exact manifestations attached to each type of these variants of IOEAc.
Conclusions
The authors in this study established a new classification of IOEAc that had a clinical value, describing its extension, site, and impact on the development of rhinosinusitis. The new classification consisted of 5 types: Type I, Type II, Type III, Type IV, and Type V. it allows the description and categorization of the recorded and unrecorded variants identified in past and future studies. It is applicable to current clinical practice.
Footnotes
Author Contributions
First author collected data from search engines and was responsible for the design and analyzing data and shared in writing the manuscript. First and fifth authors were major contributors in writing the manuscript. Then, all authors analyzed and interpreted the data regarding the diagnosis and management of the cases. All authors read and approved the final manuscript
Data Availability Statement
Accepted by all authors according to Wiley’s data sharing policy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
After obtaining approval from the local ethics committee, patients who agreed to participate gave their signed informed consent after explanation of the trial benefits and hazards. All procedures were carried out in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study received the approval of ethical committee of faculty Medicine, Menoufia University (No. 11/2019OBSGN27).
Level of Evidence
Level 2—Individual cross sectional study with consistently applied reference standard.