
Abstract
Introduction
Vocal fold leukoplakia (VFL) is a white, plaque, or patch-like lesion that appears on the vocal folds and cannot be diagnosed as any other disorder. 1 Although the prevalence was 10.2 for men, 2.1 for women per 100,000 persons and significantly associated with smoking and voice abuse, 2 VFL remains anxious for patients and ENT surgeons due to a 16% to 22.7% recurrence rate3,4 and 6% to 7% chance of malignant transformation. 5 The pathology of VFL includes hyperkeratosis or parakeratosis with non-, mild, moderate, and severe dysplasia. 6 As the efficiency of conservative treatment and rates of carcinogenesis vary with the degree of pathology, 7 pathology is then further grouped as low-risk and high-risk leukoplakia. 8 Therefore, it is vital to effectively predict the pathological degree of VFL before surgery and select appropriate treatments.
Outpatient laryngoscopy is a non-invasive and effective examination for the diagnosis and evaluation of VFL. Our previous work focused on the morphology of VFL in white light image (WLI) and suggested a 3-types classification, which included flat and smooth, elevated and smooth, and rough types. 9 Laryngoscopic scoring system was another valuable practice that described and classified VFL morphology in 6 detailed features. 10 Videostroboscopy and laryngeal dynamics analysis have also been elucidated to have a positive role in diagnosing VFL.11,12
Narrow-band imaging (NBI) was first introduced by Muto et al 13 and Yoshida et al 14 to evaluate the upper aerodigestive tract pathologies in 2004. With the specific visualization of superficial mucosal vessels by filtered blue and green light, NBI had obvious advantages in observing lesions and peripheral vascular proliferation, intrapapillary capillary loops (IPCLs) in detail. In 2011, Ni et al 15 described laryngeal cancer and precancerous lesions according to the distribution characteristics of IPCLs and proposed a 5-type classification method. In 2019, the specific 6-type classification was updated for VFL, which provided a reference for the relationship between the distribution of IPCLs and the degree of pathology. 16 However, Lin et al 17 selected 112 patients to verify the 5-type NBI classification and found high sensitivity in benign and malignant lesions, which was only 41.67% in precancerous lesions. IPCLs were indeed absent in some lesions in type II, but some thicker plaque might cover the lesion mucosa and block IPCLs, as named “umbrella effect,” leading to false negative of NBI. In order to explore the influence of the umbrella effect in the 6-type classification for VFL, we retrospectively analyzed the patients’ preoperative laryngoscopy images and their pathology, looking forward to making improvements by WLI morphological classifications to release this situation.
Material and Methods
The research was submitted and approved by the ethics committee of the Eye, Ear, Nose, and Throat Hospital of Fudan University, Shanghai, China. All patients were informed in detail and signed consent forms to allow access to their clinic and ward information.
Patients
From January 2020 to June 2022, a total of 59 patients diagnosed with VFL were included in the study. Inclusion criteria were listed as follows: (1) VFL was diagnosed by preoperative WLI, NBI laryngoscopy, and confirmed by postoperative pathology; (2) IPCLs were not observed under NBI, and VFL was classified as type II in the 2019 Ni classification; (3) Outpatient visits, surgical treatment, and postoperative follow-up were all completed by the same team of ENT surgeons. Exclusion criteria were the same as in previous studies, 18 patients with fever and coughing-related pseudomembrane, hormone-derived fungal mass, tuberculosis, or other nonkeratinized lesions were not involved in this research.
The basic characteristics of patients, including age, gender, smoking, and alcohol consumption, were collected from the inpatient medical record system for baseline comparison. Smoking more than 20 cigarettes or consuming 80 mg of alcohol per day and abstinence for less than 1 year were considered as current alcohol and tobacco consumers.
The preoperative laryngoscopy examination was completed with flexible endoscopy. The WLI and NBI was performed with a light source and central video system (CV-190, Olympus Medical Systems Corp, Tokyo, Japan) as previous research described. 19
Presurgical Evaluation of VFL in WLI and NBI
The morphological classification and laryngoscopic scoring system of VFL patients were completed by 2 independent observers, and if their opinions were unanimous, a third senior surgeon would judge.
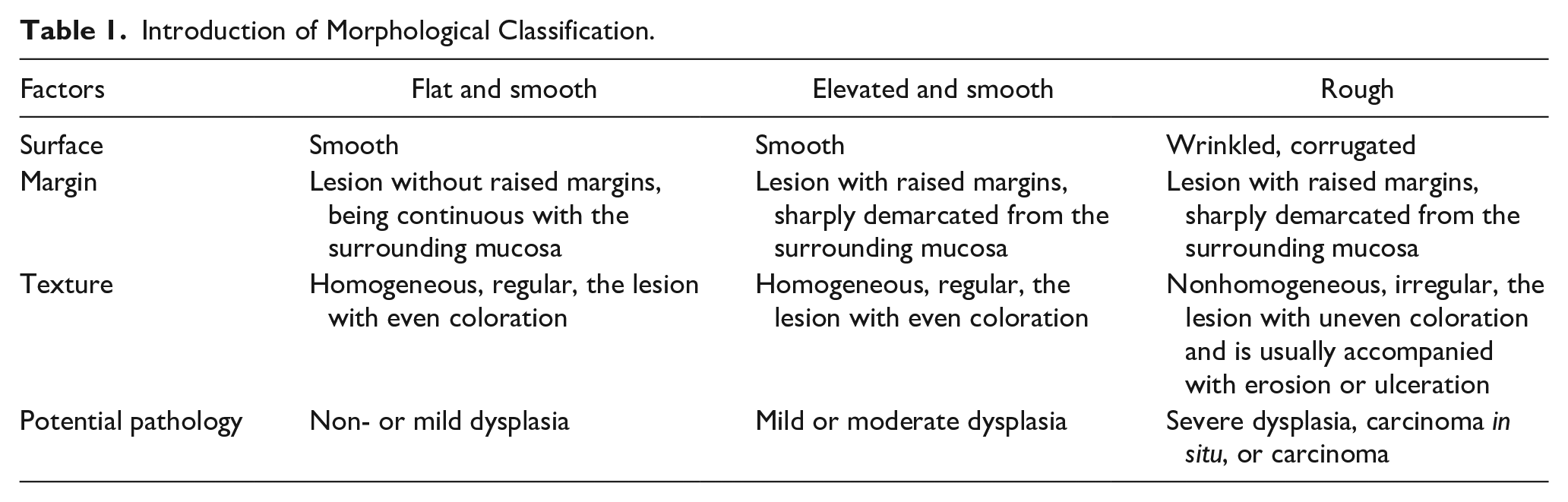
The morphological classification is listed in Table 1 as follows. 9 Three typical morphological types of VFL are shown in Figure 1. Due to the small number of flat and smooth cases in this research, it was combined with the elevated and smooth type and called the smooth leukoplakia in the statistical process.
Introduction of Morphological Classification.
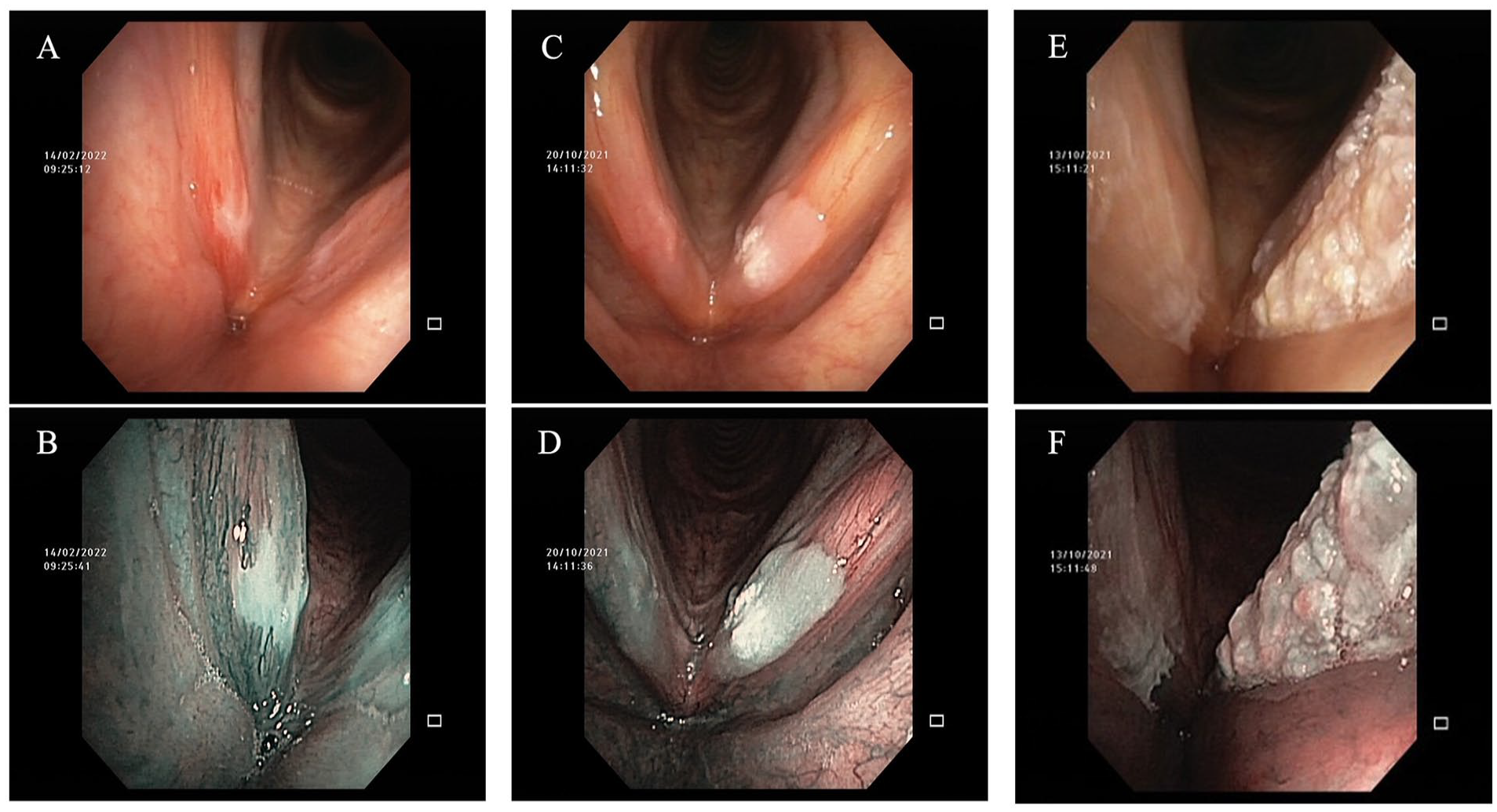
Morphological classification of vocal fold leukoplakia. Flat and smooth leukoplakia in white light (A) and NBI (B); Elevated and smooth leukoplakia in white light (C) and NBI (D); Rough leukoplakia in white light (E) and NBI (F). NBI, narrow-band imaging.
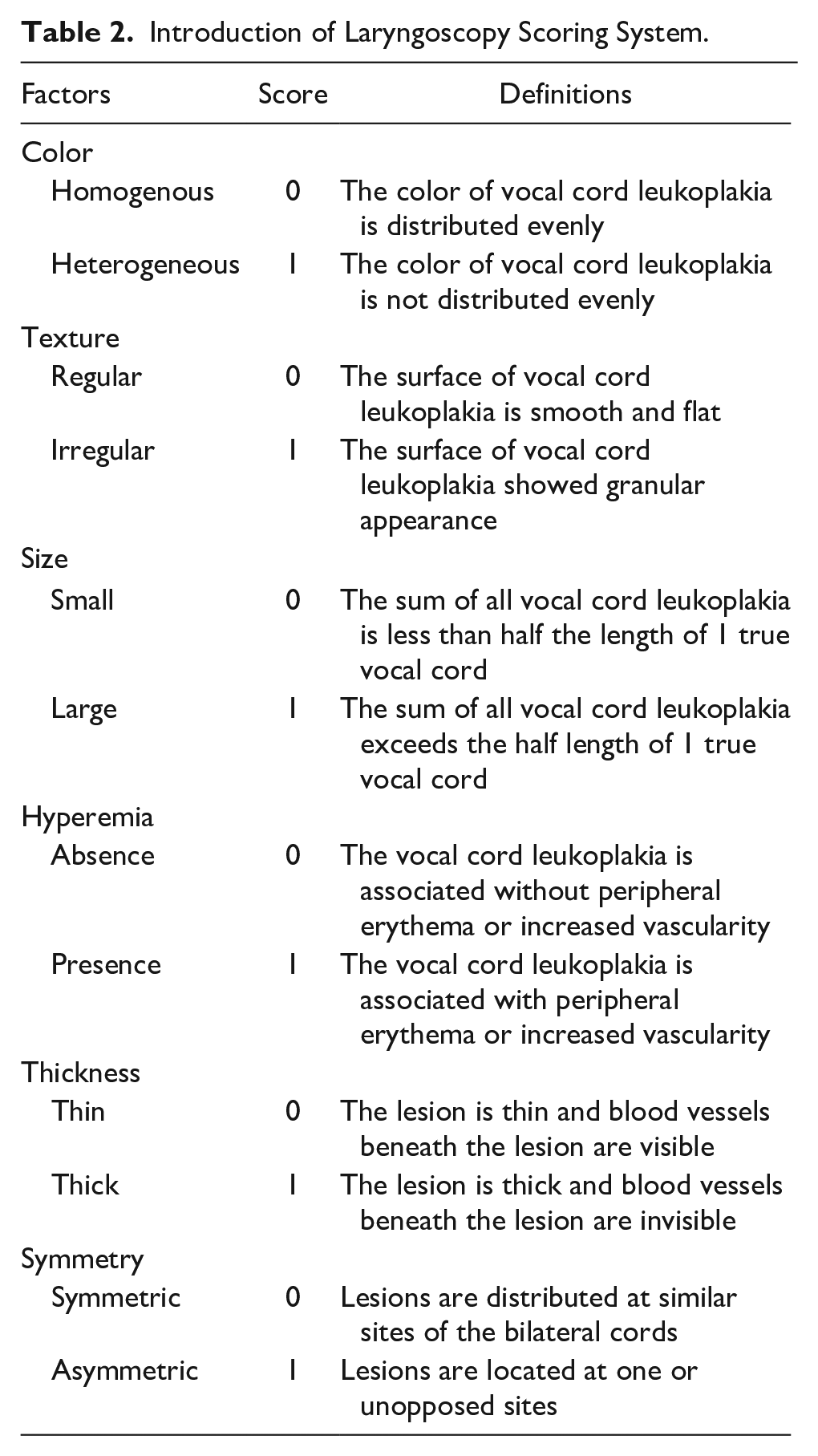
The details of laryngoscopic scoring system 10 are as follows in Table 2 and typical VFL with low/high scoring is shown in Figure 2.
Introduction of Laryngoscopy Scoring System.
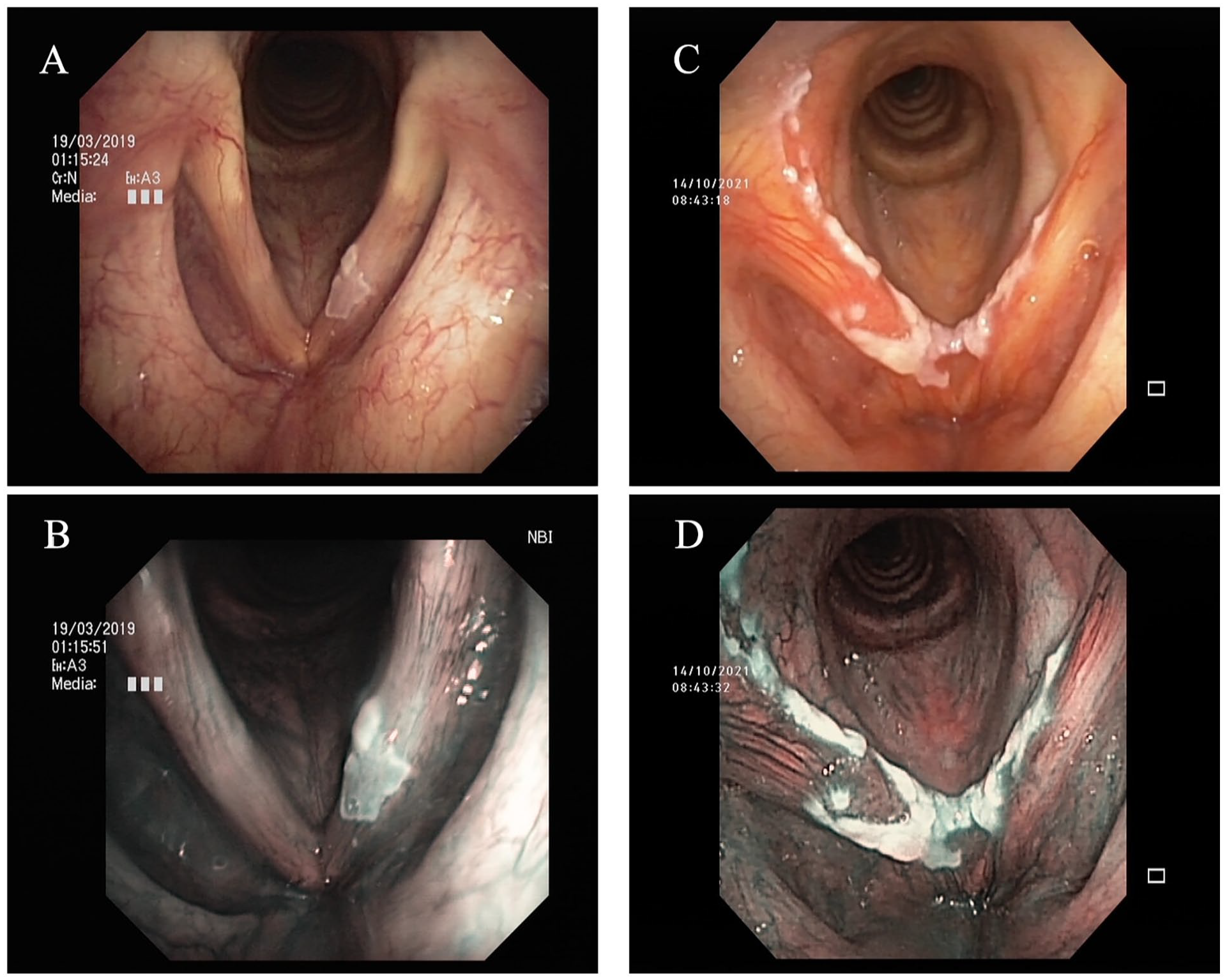
Laryngoscopy characteristics of vocal fold leukoplakia with type II in 2019 Ni IPCLs classification. (A, B) A case of leukoplakia with homogenous color, regular texture, small size, absence of hyperemia, thin thickness, asymmetric lesion, absence of edema in white light, and NBI. (C, D) A case of leukoplakia with nonhomogeneous color, irregular texture, large size, exist of hyperemia, thick thickness, symmetric lesion, exist of edema in white light, and NBI. IPCLs, intrapapillary capillary loops; NBI, narrow-band imaging.
The type II of 2019 Ni classification in NBI was described as VFL which contained thicker white plaque on the vocal cord and neither IPCLs nor obliquely running vessels or branching vessels can be found, other 5 types were defined the same as original research. 16
Treatments
For patients with flat and smooth, elevated and smooth VFL, it was recommended to first treat the cause of the disease such as voice rest, smoking cessation, and acid suppression therapy. Surgical resections were employed for patients whose VFL presented type II in NBI with rough morphology, no releasement with conservative treatments, or those with carcinophobia and strongly demanded surgeries for flat and smooth, elevated and smooth leukoplakia.
Surgery was performed under general anesthesia and a self-retaining laryngoscope. When the glottis was fully exposed under the binocular microscope (ZEISS S88, Carl Zeiss Co., Tuttlingen, Germany), lesions were resected with 1mm margins for flat and smooth type and 2 to 3 mm margins for rough type and mucosal dissection using carbon dioxide laser (Lumenis 40 C, Yokneam 20692, Israel). The patients were discharged on the second postoperative day and underwent regular follow-up at 1 week, 1 month, 3 months, and 1 year after discharge.
Pathology Diagnoses
All postoperative pathology of VFLs was completed by the pathology department of our hospital and reviewed by senior pathologists. Reports described VFL pathology according to the 2005 WHO standard as hyperkeratosis or parakeratosis with non-, mild, moderate, severe dysplasia, carcinoma, 6 which were further regrouped as low-risk (non-, mild, moderate dysplasia) and high-risk VFL (severe dysplasia) according to research proposal of Ni 2019 classification. 16
Correlation of WLI and NBI Classification With Pathology
In morphological classification, smooth type referred to VFL with non-, mild, and moderate dysplasia; rough type contained severe dysplasia and carcinoma. There was no certain correspondence between the laryngoscopic scoring system and pathology. In the 2019 Ni classification, type II was defined as “benign leukoplakia” which contained non-, mild, moderate dysplasia. A definitional contradiction arose about the grouping of moderate dysplasia between 2019 Ni research and 2017 WHO Blue Book; 20 in this research, the former remained the main reference, and moderate dysplasia was grouped with non-, mild dysplasia as low-risk VFL.
Statistical Analysis
SPSS version 22.0 software (IBM Corporation, Chicago, IL, USA) was employed to complete the statistical calculations in this research. The comparison of age was completed with one-way ANOVA, other comparisons, including the baseline data, and morphology correspondence with pathology, were accomplished with R*C Chi-square test. Two-sided P values <.05 were viewed as statistically significance.
Results
The pathologies of type II VFL in this research contained 1 case of leukoplakia with non-dysplasia, 12 cases with mild dysplasia, 15 of moderate dysplasia, 8 of severe dysplasia, 23 of carcinoma according to the 2005 WHO standard, which were further regrouped as 28 cases of low-risk and 31 cases of high-risk VFL. The baseline analysis between low- and high-risk groups found no statistical difference in age (61.8 vs 65.5, P = .095), and gender (1 female in each group, P = .414). The percentages of current smokers (51.5% vs 17.9%, P < .001) and alcohol consumers (21.2% vs 3.6%, P < .001) in the high-risk group were significantly higher than that in the low-risk group.
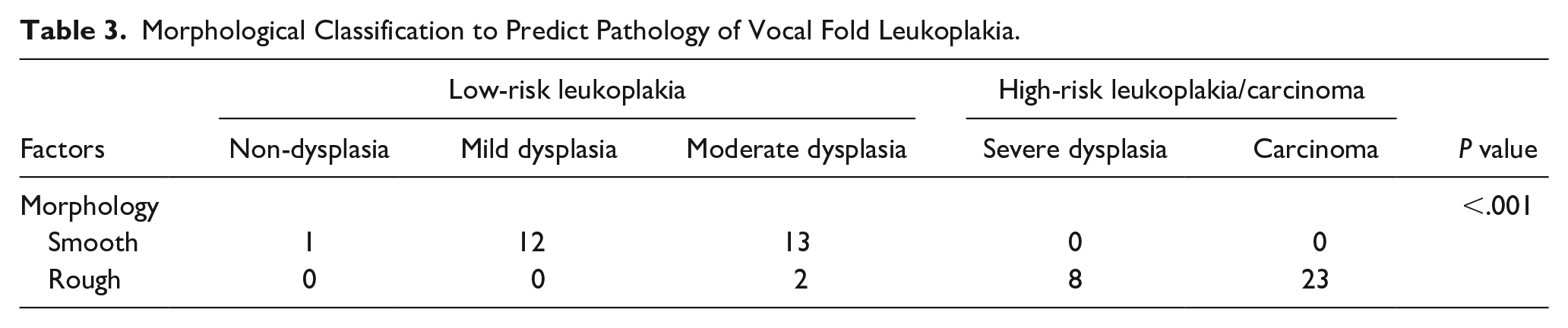
According to the morphological classification (as shown in Table 3), there was 1 case with non-dysplasia in smooth leukoplakia. Another 25 cases of smooth leukoplakia were also identified as mild dysplasia (12 cases) and moderate dysplasia (13 cases). The cases with rough morphology included 2 cases with moderate dysplasia, 8 cases with severe dysplasia, and 23 cases with carcinoma. With reference to the pathological classification criteria preset in this research, all cases with smooth morphologies correctly correspond to their expected pathological types. While 2 cases in rough leukoplakia came to be milder pathology as moderate dysplasia.
Morphological Classification to Predict Pathology of Vocal Fold Leukoplakia.
When laryngoscopic scoring system was applied to analyze type II VFL (as shown in Table 4), high-risk leukoplakia and carcinoma were more likely to have nonhomogeneous color (P = .024), irregular texture (P = .002), large size (P < .001), thickness (P < .001), which was proven by univariate analysis, while the hyperemia and symmetry situations were found without statistical difference. In multivariate analysis, only texture (P = .025), size (P = .002), and thickness (P = .016) remained significant differences between low-risk and high-risk leukoplakia/carcinoma.
Correlation of Laryngoscopy Scoring System of Vocal Fold Leukoplakia With Pathology.
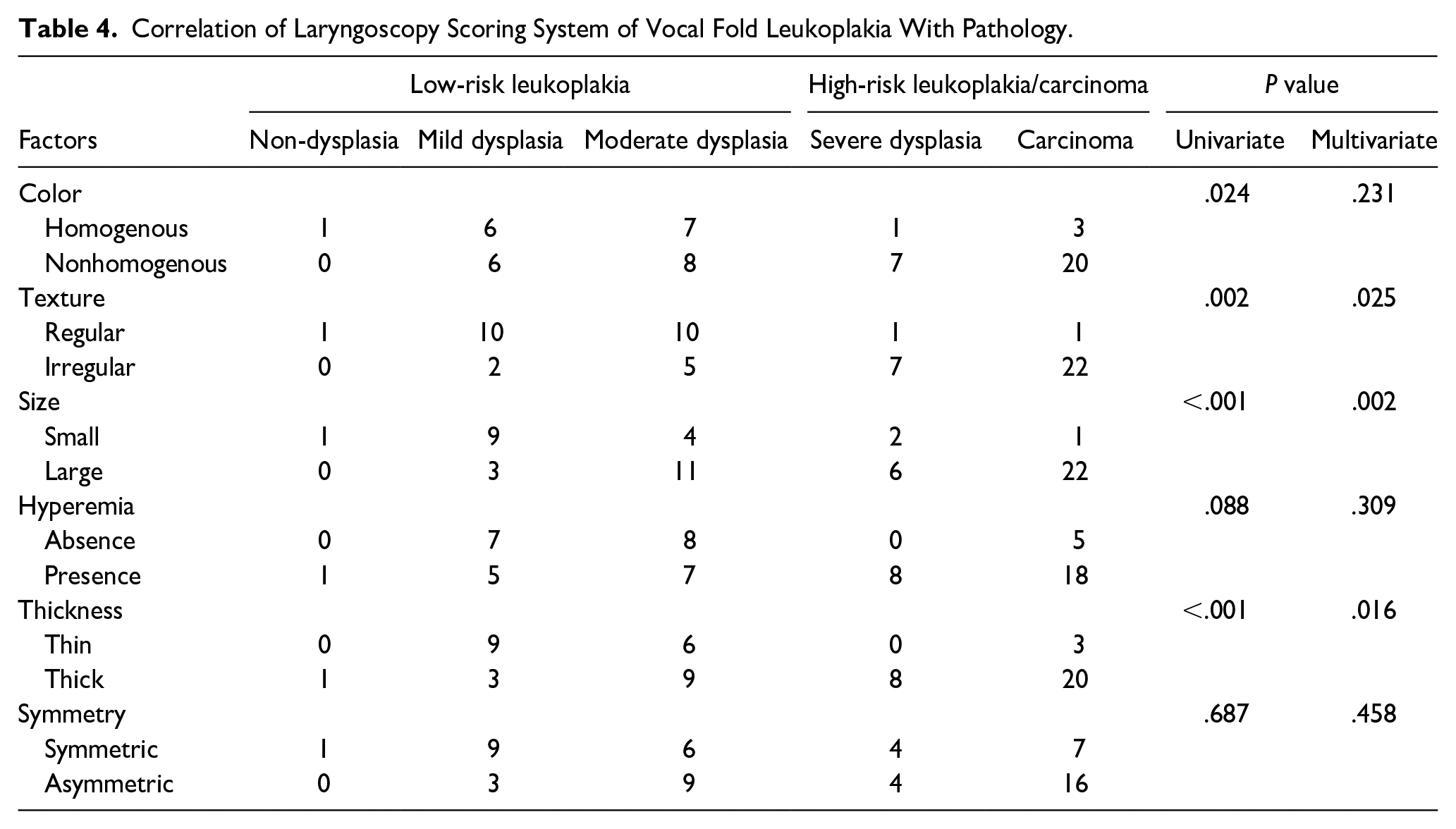
Of the 3 indicators, texture was the most accurate predictor of VFL pathology. There were 7/8 (87.5%) of severe dysplasia, 22/23 (95.7%) of carcinoma performed irregular texture, 1/1 (100.0%) of non-dysplasia, 10/12 (83.3%) of mild dysplasia, and 10/15 (66.7%) of moderate dysplasia showed regular texture. Size and thickness also had an accurate predictive ability for high-risk leukoplakia/carcinoma, but their ability to distinguish moderate dysplasia was not as good as texture. Only 4 cases (26.7%) of moderate dysplasia leukoplakia were less than 50% of the full length of the vocal cords, and the remaining 11 cases were more than half the length of the vocal cords. Thin thickness was observed in 6 of 15 (40.0%) moderate dysplasia lesions, other 9 cases (60.0%) showed thicker plaques.
Discussion
Among the non-invasive methods of preoperative prediction of VFL pathology, NBI presented unique advantages in comparison with other laryngoscopy examinations such as white light laryngoscopy and dynamic laryngoscopy. By filtering the red-light band to retain the blue and green-light bands, NBI could clearly display the running blood vessels in the mucosal layer and the superficial layer of the lamina propria, especially the perpendicular neovascularization to the mucosa, namely IPCLs. Previous studies generally believed that NBI had certain advantages over WLI in predicting laryngeal lesions, especially laryngeal precancerous lesions. 21 This advantage could not be fully exploited when it came to absence of IPCLs. 22 Considering that it was difficult for NBI to accurately predict the pathology in the VFL where IPCLs could not be observed, it was inevitable to employ other methods to assist in the prediction of these leukoplakia, and the morphological classification based on WLI or NBI had become the first choice, which achieved positive outcomes in distinguishing severe dysplasia, carcinoma in type II VFL.
As a specific classification method for the IPCL characteristics of VFL, Ni et al reported an application to 120 VFL patients and found that the classification method had an accuracy of 90.8%. 16 However, 17 cases in the study had pathological findings of chronic inflammation rather than epithelial proliferation/hyperkeratosis/dyskeratosis, the accuracy of NBI to distinguish leukoplakia from white plaques was 85.8%. Therefore, it should be emphasized that not all white lesions were leukoplakia, and non-keratinizing white lesions should still be excluded before diagnosis. In this research, there were 59 patients with no observable IPCLs and were classified as type II, in which the pathological types spanned a wide range from non-dysplasia to severe dysplasia, to invasive carcinoma. Despite Ni’s research, Huang et al 21 published a study contained 57 VFL patients, in which IPCLs was not observed in 33 cases. The pathologies of these patients included 4 cases with moderate dysplasia and 2 cases with severe dysplasia. Giulia et al 23 also found 5 moderate dysplasia and 2 severe dysplasia in 56 IPCLs-missing cases. The results of the above studies are roughly similar, the pathologies of 3.5% to 6.0% of VFL with absence of IPCLs under NBI were severe dysplasia and carcinoma.
Our study found that the type II VFL differed greatly in their pathological types, but the focus was mainly on high-risk leukoplakia, especially in invasive carcinoma (23/59). We believed that this was related to the stricter control of surgical indications in this medical unit, as patients were required to undergo 2 to 3 months of drug and sound rest therapy, and then the no relief part was performed with surgery. At the same time, because some patients in this study were patients who had undergone multiple surgical treatments in other hospitals and still had recurrence, their pathological types might have progressed. Therefore, the high-risk leukoplakia/invasive carcinoma pathologies of type II VFL patients were particularly prominent in this study.
In this study, both morphological classification and laryngoscopy scoring systems managed to distinguish most high-risk leukoplakia/invasive carcinoma from low-risk leukoplakia. The main difference between the 2 was the principle of classification, as morphological classification advocated classifying with the most accessible description, which was easy for laryngoscopists and clinicians to remember and apply, while laryngoscopy scoring system described the characteristics of VFL under white light as comprehensive and detailed as possible. This result underscored the role of macroscopic features of VFL, especially texture, size, and thickness, in predicting pathology. Referring to the classification characteristics of oral leukoplakia, the texture could not be ignored as a very important reference factor. 24 Fang et al 10 also supported the texture of VFL being an independent factor in predicting malignancy, but the original research did not come to the result that size might be another positive index in differentiating high-risk leukoplakia. While Lee et al 25 summarized the morphological features of 63 VFL patients and grouped them with postoperative pathology, the results found that extent of VFL resulted in statistically significant differences for both the recurrence and malignant transformation of VFL. As for thickness, the original intention of this research was to explore the pathological types of thicker leukoplakia. Several studies have also found that thicker leukoplakia can produce the umbrella effect of IPCLs, making pathological prediction of high-risk leukoplakia difficult.17,26
An inconclusive problem encountered in the previous research reference and method design of this research was the grouping problem of moderate dysplasia in the dichotomy of pathology, that was, whether it belongs to the low-risk group or the high-risk group. In 2019, when Ni et al released the 6-type NBI classification for VFL, moderate dysplasia was grouped with non- and mild dysplasia. This classification might refer to the guidelines for the diagnosis and treatment of laryngeal leukoplakia issued by China in 2018, 8 in which mild to moderate dysplasia was grouped into one category from the perspective of the difficulty of distinguishing the shape and size of epithelial basal nuclei in pathological detection and the incidence of clinical malignant transformation. In the 2017 WHO Blue Book, moderate and severe dysplasia were classified as high-grade dysplasia, which was also the pathological classification method referred to in this study. The main basis for this classification is whether the atypical epithelial cells occupying at least lower epithelial half up to the whole epithelial thickness of VFL, and the malignant potential of laryngeal precursor lesions. The pathological classification was an important way to provide a reference for the clinical tendency of malignant transformation, the cancer probability of moderate dysplasia leukoplakia should be paid with more attention. Isenberg et al 5 reviewed 136 patients (208 biopsies) in their institution and found squamous cell carcinoma developed in 83 of 824 (10.1%) patients with mild-moderate dysplasia. Zhang et al published a retrospective study of 86 VFL patients, in which 5 of 25 (20%) patients with moderate dysplasia developed carcinoma, the moderate dysplasia had a similar progression rate to severe dysplasia (2/14, 15%). At present, researchers with larger sample sizes focused on moderate dysplasia still need to clarify whether its clinical characteristics are closer to mild or severe dysplasia, which might provide a basis for more reasonable pathological grouping. This research emphasized the role of diversified assessment methods in the prediction of VFL pathology through preoperative laryngoscopy-related examinations, we introduced morphological classification in VFL without IPCLs and obtained positive results. In the following research, we will try to integrate the 2 classification methods and give full play to their respective advantages to further improve the accuracy of pathological prediction. Also, full-trained artificial intelligence (AI) based on optimized classification was the future scope of preoperative laryngoscopy-related examinations. Currently, fully trained AI can achieve a judgment accuracy similar to that of ENT experts, 27 synchronizing the mature AI database to the outpatient laryngoscopy system during the examination process will play an important role in real-time pathological prediction of VFL.
There were still some shortcomings in this research to be improved. Firstly, the particularity of the patient structure in our hospital leads to more patients with severe disease, type II leukoplakia in NBI was not the most common type of VFL during our research, the sample size of this study could still be expanded to eliminate the potential bias and verify the predictive value of morphological typing for pathology in type II leukoplakia. Secondly, the classification of moderate dysplasia encountered in the methodological design of this study still needed to be resolved, as different classifications might have an impact on the results obtained.
Conclusion
In summary, the pathologies of VFL with type II in NBI classification were hard to be predicted. Morphological classification and laryngoscopy scoring system contributed to predict pathology in leukoplakia, lesions with irregular/rough texture were more likely to be high-risk pathology.
Footnotes
Data Availability Statement
The patient data used in this study came from the Eye, Ear, Nose, and Throat Hospital of Fudan University and was protected by the ethics committee. If relevant information is needed, please contact email
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the Science and Technology Commission of Shanghai Municipality of China (Grant 21Y11912000 and 22ZR1409800) and also supported by National Natural Science Foundation of China (Grant 82271149 and 82102863).
Disclaimers
The views expressed in the article were authors own opinions and not an official position of the institution or funder.