
Abstract
Intrathyroidal parathyroid carcinoma is an extremely rare cause of primary hyperparathyroidism. We reported a 51-year old woman who presented symptoms of hypercalcemia. 99mTc sestamibi single-photon emission computed tomography/computed tomography (CT) revealed a large hypermetabolic nodule in the left thyroid lobe suggestive of hyperfunctioning parathyroid tissue. 11C-methionine positron emission tomography/computed tomography (PET/CT) and 18F-fluorocholine PET/CT confirmed the nodule in the left thyroid lobe and also revealed a hypermetabolic activity on the posterior surface of the lower left pole. The patient underwent a total thyroidectomy and parathyroidectomy, and a diagnosis of bifocal intrathyroidal parathyroid carcinoma was confirmed. We present the first reported case of bifocal intrathyroidal carcinoma and discuss the discordant imaging results.
Introduction
Parathyroid carcinoma (PC) is a rare endocrine tumor. It represents 0,5-5% of primary hyperparathyroidism (PHPT) cases. 1 Preoperative localization sensitivity and accuracy of PC is challenging and results vary in literature. We reported a case of a bifocal intrathyroidal PC with discordant imaging results. This is the first case described in literature.
Case Report
A 51-year old woman consulted at the emergency ward for palpitation and lipothymia having appeared 2 weeks before. The patient also reported polyuria and polydipsia. A blood sample highlighted severe hypercalcemia: 4.66 mmol/L (reference range: 2.15-2.50 mmol/L), high-serum parathyroid hormone (PTH) level: >1600 ng/L (reference value < 49.00 ng/L), and hypokalemia: 2.5 mmol/L (reference range: 3.5-4.5 mmol/L). Renal and liver functions were normal. The clinical examination was normal. Considering the severe hypercalcemia associated with an abnormally high level of PTH, a PC was suspected. The patient was hospitalized to balance the electrolyte disorder and start the PHPT assessment.
Neck ultrasound highlighted a multinodular goitre with a large nodular formation of 28.4 × 20.9 × 49.5 mm3 suggestive of a parathyroid adenoma in the lower left thyroid lobe and a mixed solid cystic nodule of 23.3 × 17.2 × 15 mm3 in the upper right thyroid lobe.
A cervicofacial computed tomography (CT) confirmed the presence of a multinodular goitre in the left lobe and also revealed a nodule of 13 × 10 × 10 mm3 below the left thyroid lobe, compatible with a parathyroid adenoma. A complementary 99mTc sestamibi single-photon emission computed tomography (SPECT) highlighted a large slowdown MIBI washout zone in the left thyroid lobe and a more discreet hypermetabolic heterogenic nodule in the right inferior thyroid lobe (Figure 1).
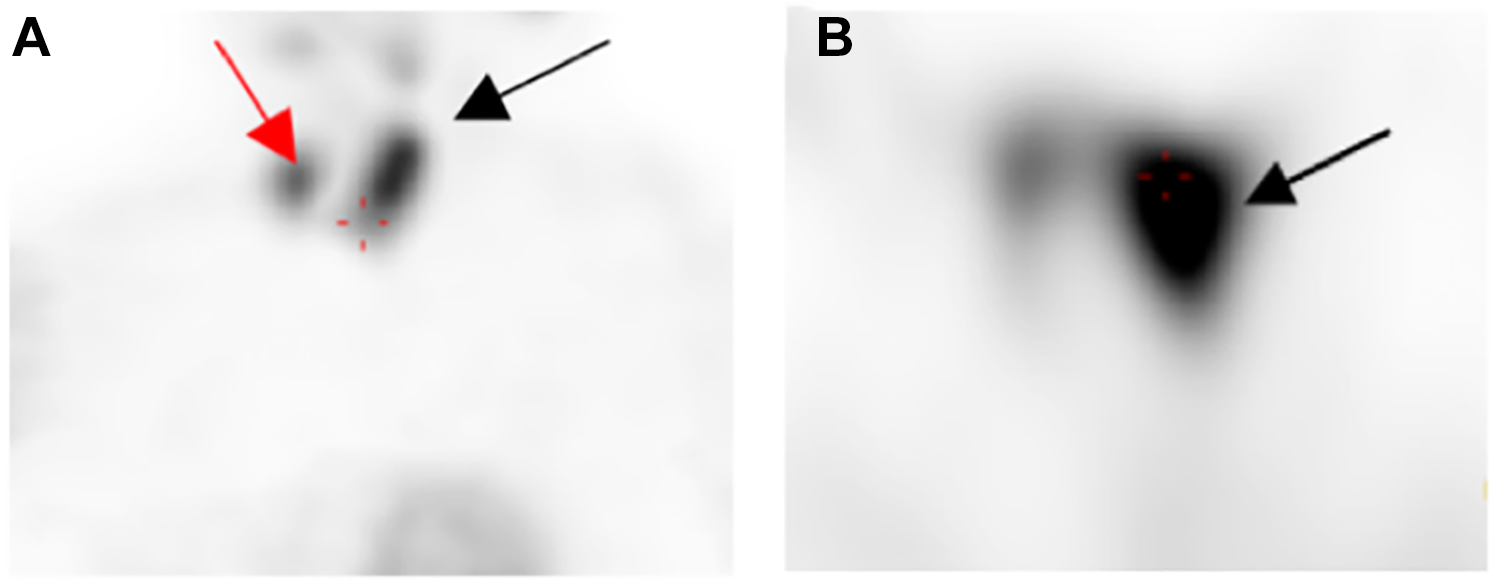
99mTc sestamibi single-photon emission computed tomography (SPECT). A, Coronal plan: a large slowdown MIBI washout zone in the left thyroid lobe (black arrow) and a more discreet nodular zone in the inferior right pole of thyroid (red arrow). B, Axial plan: large nodule in the left thyroid lobe (black arrow).
The imaging assessment was supplemented by positron emission tomography (PET) using 2 radiotracers: methionine (11C-methionine PET/CT) and fluorocholine (18F-fluorocholine PET/CT). These confirmed the large hypermetabolic nodule in the left thyroid lobe and revealed a hypermetabolic activity on the posterior surface of the lower left pole (Figure 2).
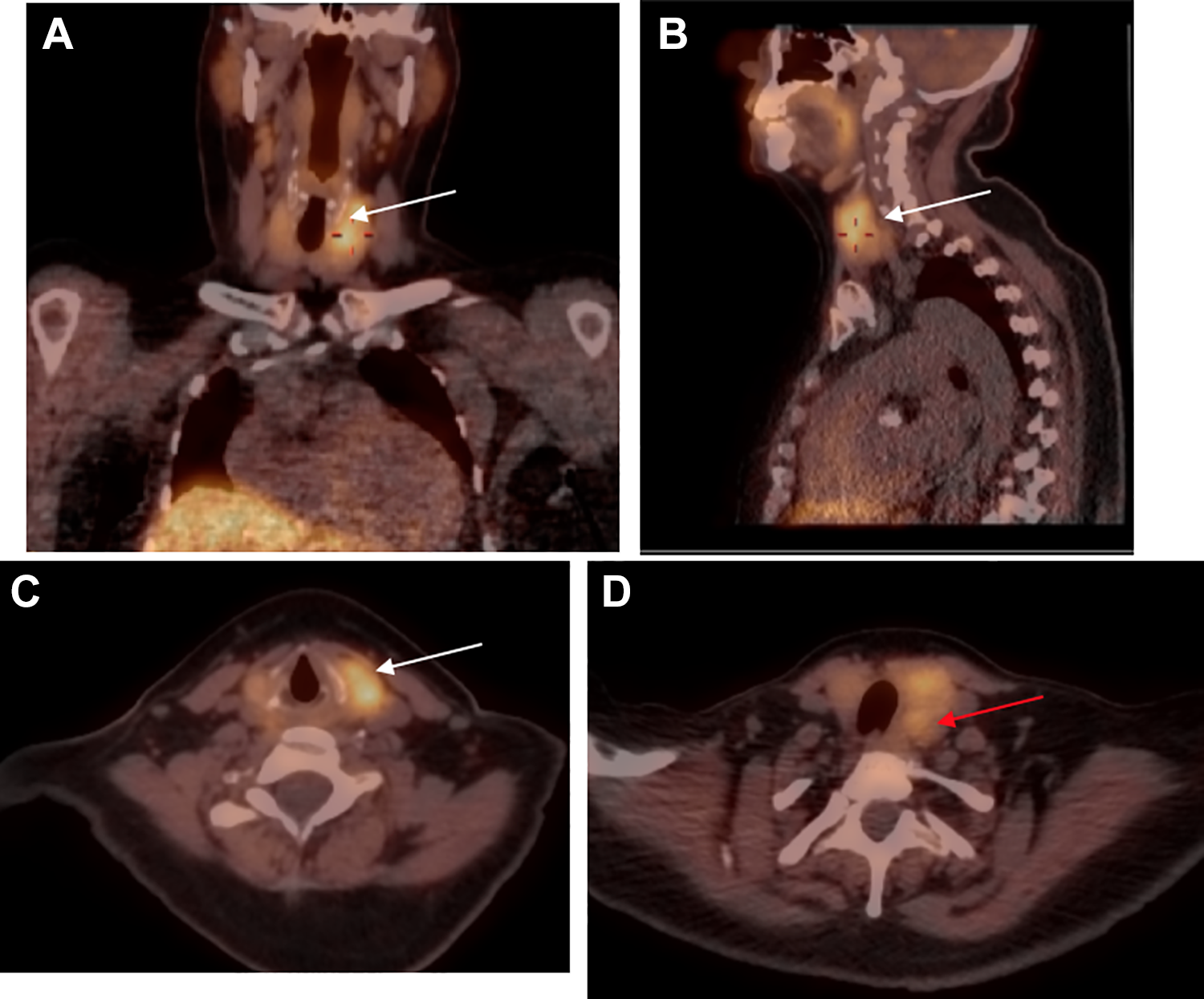
11C-methionine PET/CT: Hypermetabolic activity in the upper pole of the left thyroid lobe (white arrow) and oval uptake lesion in the posterior part of the lower pole of the left lobe (red arrow). A, Coronal plan; (B) sagittal plan; (C-D) axial plan. Similar results with 18F-fluorocholine PET/CT. PET/CT indicates positron emission tomography/computed tomography
A thyroid–parathyroid “en-bloc” resection was performed. The pathological analysis revealed a bifocal intrathyroidal PC: a nodule of 35 × 20 × 20 mm3 with capsular breach in the upper left thyroid and the other one of 8 mm on the posterior surface of the lower thyroid lobe. These 2 nodules corresponded to lesions found by PET CT.
Due to positive resection margins, an increasing level of postoperative calcium and a high-recurrence rate, a follow-up by 18F-fluorocholine PET/CT was recommended. However, the patient did not attend the follow-up. To our knowledge, this is the first reported case of bifocal intrathyroidal PC.
Discussions
Parathyroid carcinoma is a rare endocrine tumor accounting for 0.5% to 5% of PHPT. 1 Less than 1000 cases of PC have been reported in the literature 2 and only 20 cases with an intrathyroidal localization. 3 To the best of our knowledge, our patient is the first reported case of bifocal intrathyroidal PC.
The association of biological and imaging criteria can lead to suspect a PC (1), but the final diagnosis is based on histological analysis. Imaging methods of choice for locating parathyroid lesions preoperatively are neck ultrasound and 99mTc sestamibi. 4
In our case, 99mTc sestamibi SPECT CT showed one of the two localizations of PC in the left thyroid lobe. A 2005 meta-analysis estimated the sensitivity of dual phase 99mTc sestamibi at 86%. 5 Sensitivity seems to be lower in patients with concomitant multinodular goiter 6 or in case of multiple localization with a sensitivity of 88.9% for single adenoma and 29.9% for double localization. 7
For cases with equivocal imaging results, second-line imaging modalities can be used and showed promising results. In our case, patient performed PET CT with 2 different radiotracers (methionine and fluorocholine), and results were comparable with a sensitivity of 100%. Two recent studies revealed that 11C-methionine PET/CT or 18F-fluorocholine PET/CT can be useful as a second-line in patients with negative or discordant conventional imaging modalities.8,9
The gold standard treatment of PC is an “en-bloc” resection of the tumor associated with a homolateral thyroid loboistmectomy. 10 In our case, a total thyroidectomy was performed due to positive resection margins. Patient should be closely followed over time due to the high degree of persistent or recurrent disease (more than 50%). 2 Besides the monitoring of PTH and calcium levels, imaging has a major role in the postoperative follow-up and may help for detection and localization of persistent or recurrent PC. In a recent prospective study, 18F-fluorocholine PET/CT showed better results than 99mTc-sestamibi SPECT/CT in the detection and localization of small size parathyroid adenomas. 11 Therefore, 18F-fluorocholine PET/CT may have an adjunctive role in the postoperative follow-up of PC, in particular in early stages.
However, PC is rare and poorly represented in the studies. Therefore, no consensus about its management is clearly established.
Footnotes
Authors’ Note
The authors certify that they have obtained all appropriate patient consent about the images and other clinical information reported in this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.