
Abstract
Soft tissue defects in the head and neck are frequently encountered, often resulting from trauma or the surgical management of malignancies. Flap reconstruction plays a critical role in the closure of these defects, aiming to minimize complications and improve cosmetic outcomes. While various flap techniques are commonly utilized in head and neck reconstruction, to the best of our knowledge, the bilobed flap has not been previously reported in this anatomical region. We present a case involving a patient with a complex underlying medical condition, which elevated the risks associated with prolonged anesthesia. In light of these considerations, we opted to use a bilobed flap, which was successfully employed for the reconstruction of an intermediate-sized soft tissue defect in the right submental area following resection of recurrent oral cancer. After undergoing multiple surgeries and concurrent chemoradiotherapy, the 65-year-old male patient developed significant neck stiffness, making direct closure unfeasible and traditional local flap techniques ineffective for wound management. The bilobed flap was meticulously planned, with the first lobe positioned over the adjacent site of the right submental defect and the second lobe located next to the first lobe, employing a double transposition design. The flap healed without complications, and the patient experienced a good recovery. This case report underscores the effectiveness of bilobed flaps in reconstructing moderate-sized soft tissue defects in patients with recurrent neck metastatic oral cancer after previous neck dissection and concurrent chemoradiotherapy.
Introduction
Oral cancer (OC) is the most common malignancy of the head and neck region, exhibiting significant variations in incidence based on geographic location and age group. The global age-standardized rate of OC is 6.0 per 10,000 in males and 2.3 per 10,000 in females. 1 Surgical excision and reconstruction for OC often lead to substantial functional and aesthetic deficits, profoundly impacting patients’ quality of life. The etiology of OC is multifactorial, with key risk factors including smoking, other forms of tobacco consumption, snuff dipping, alcohol use, sunlight exposure, and viral infections. Managing recurrent neck metastatic OC, particularly following neck dissection and concurrent chemoradiotherapy (CCRT), presents substantial challenges in surgical reconstruction. This necessitates innovative techniques such as a bilobed flap to improve the outcome if the patient is not feasible for prolonged anesthesia.
The bilobed flap, a local transposition flap, is a double transposition technique wherein the first lobe fills the primary defect and the second lobe fills the defect created by the transposition of the first lobe, known as the secondary defect. 2 Initially described in 1918 by Esser, the bilobed flap was primarily used for reconstructing small- to moderate-sized cutaneous nasal defects. Zimany later expanded the utility of this flap, suggesting that the second and third lobes could be smaller than the first, thus allowing its application in a broader range of anatomical areas. In the 1980s, McGregor and Soutar further refined the technique, emphasizing that a reduced pivotal angle would result in smaller standing cutaneous deformities and decreased pincushioning, thereby improving the aesthetic and functional outcomes of the reconstruction. 3 Over time, the bilobed flap has undergone numerous modifications and has been adapted for use in various anatomical regions, such as infra-auricular flaps, lateral cheek defects, and the reconstruction of large keratoacanthomas on the thumb. In this report, we present a case involving a recurrent tumor that necessitated surgical intervention and further adjuvant CCRT. 4
Case Presentation
The case presented was a 65-year-old male with a medical history of coronary artery disease, end-stage renal disease on regular hemodialysis, type 2 diabetes mellitus, hyperlipidemia, and prostate adenocarcinoma (cT2cN0M0, stage IIIC). The patient also had a previous diagnosis of 2 right tongue squamous cell carcinomas (both were pT1N0M0, stage I), for which he underwent wide excision, right selective neck dissection, and adjuvant CCRT 10 years ago. Furthermore, he developed squamous cell carcinoma of the right floor of the mouth (pT1cN0M0, stage I) and underwent tumor wide excision with fascia lata reconstruction 1 year ago.
This time he presented with a right submental mass noted for 2 months. Upon physical examination, a right fixed submental mass was observed. After the image studies and tissue sampling, the diagnosis was recurrent right submental soft tissue metastasis (cN3b). Given this diagnosis, the patient was admitted for surgical intervention. The patient’s general condition was not suitable for free flap reconstruction or prolonged anesthesia. Consequently, a bilobed flap reconstruction was planned and executed, with the first lobe positioned adjacent to the excision site of right submental area and the second lobe situated connecting to the fist lobe, utilizing a double transposition design (Figure 1). Intraoperatively, significant neck stiffness attributable to prior CCRT was observed, and minimal soft tissue remained following the extensive tumor excision. The right submental area skin defect size was 6 cm × 5 cm after soft tissue tumor wide excision (Figure 2A). Modified radical neck dissection on the left side was also performed simultaneously under the same skin incision design with a horizontal extension at the end of the bilobed flap (Figure 2A). This approach facilitated effective reconstruction and promoted favorable recovery in the limited soft tissue area (Figure 2B). His postoperative care was smooth and was discharged from our ward on postoperative day 4. The patient underwent adjuvant radiotherapy 1 month postoperatively, demonstrating good tolerance. At the 3rd month follow-up, the wound exhibited excellent healing with no evidence of infection or contracture (Figure 2C).
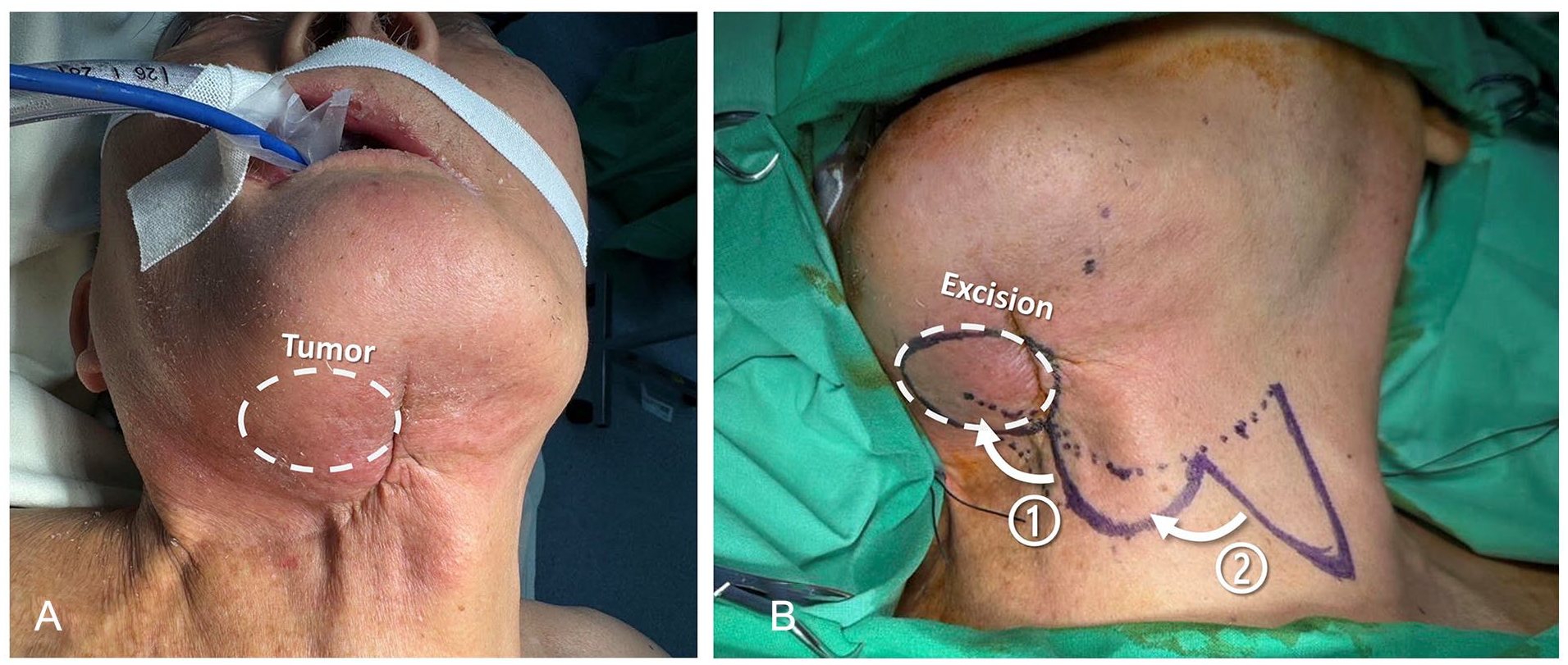
(A) Lump within the white circle indicates the recurrent neck metastatic oral cancer. (B) Surgical planning utilizing a bilobed flap and double transposition design.
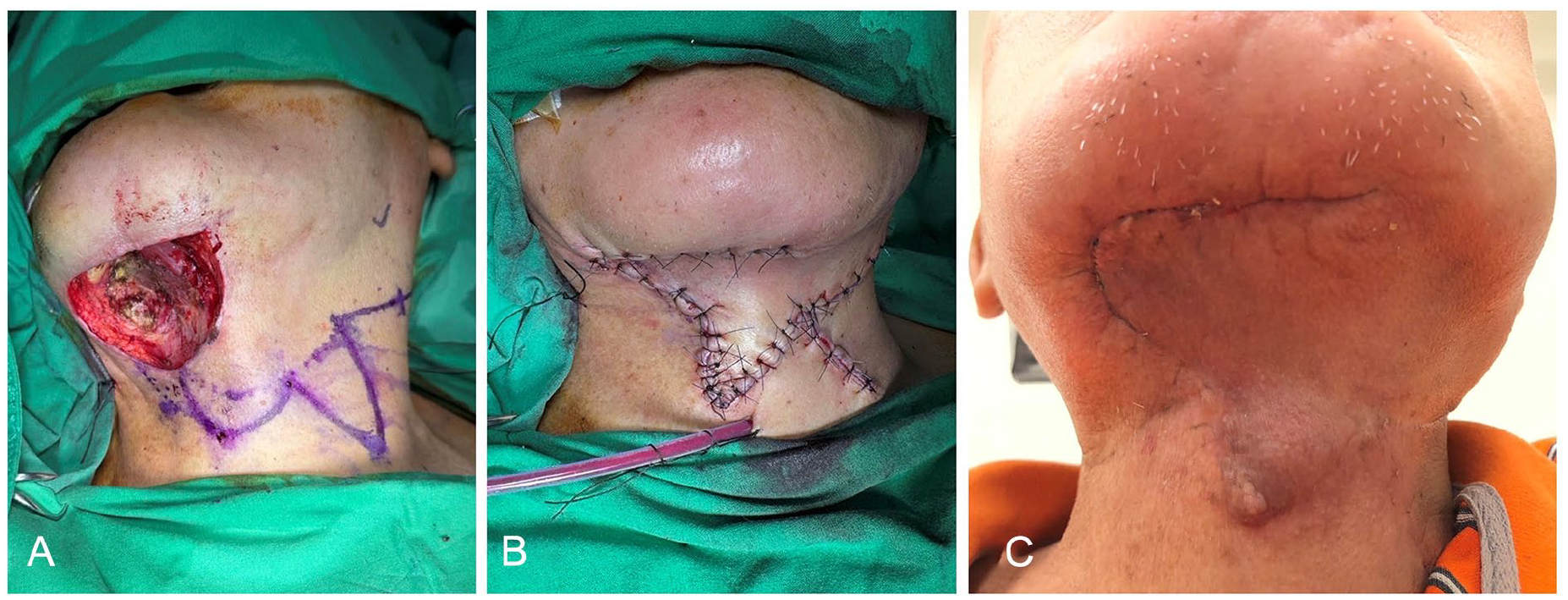
(A) Wound demonstrates significant depth and extensive soft tissue loss following excision, and the defect size is 4.9 cm × 4.0 cm. (B) Postclosure, there is no visible defect or tight suturing causing soft tissue ischemia. (C) At the 3rd month follow-up, the wound exhibits excellent healing and aesthetic appearance.
Discussion
Although the use of bilobed flap surgery is well-documented across various anatomical regions,5-9 to the best of our knowledge, there are no reported cases of its application in the neck region, particularly under challenging conditions such as scar formation and rigid soft tissue following previous surgery and concurrent CCRT. Patients undergoing head and neck reconstruction prioritize minimal visible scarring and the preservation of function. 10 This case represents the first reported use of a bilobed flap for reconstruction in the neck region.
In our patient, a moderate-sized (6 cm ×5 cm) defect was deemed unsuitable for local flap reconstruction, such as Z-flap technique, due to an elevated risk of dehiscence and infection. 11 Rhomboid flaps are ideal for small to moderate defects, offering efficient tension redistribution, good vascularity, and long-term favorable cosmesis. 12 However, they are less suitable for larger or more complex defects, especially in patients with limited tissue mobility, as is often seen in post-CCRT cases. Rotational flaps offer versatility for moderate defects but may lack sufficient reach for larger defects, and tension at the closure site can compromise blood flow, increasing the risk of wound dehiscence or infection. 13 Several regional flap options were considered prior to surgery. Deltopectoral flaps are highly reliable for head and neck reconstruction, but they can significantly limit arm mobility, require skin grafting at the donor site, and result in prominent scarring, potentially impacting postoperative aesthetics and patient satisfaction. 14 The Pectoralis Major flap, widely used for large defects, provides robust coverage and excellent vascularity; however, its tendency to create bulky reconstructions poses aesthetic concerns, particularly in the neck, where contouring is critical. 15 Free flaps can cover large and complex defects that are not amenable to local flap techniques and can be used in areas where local tissue is compromised, such as after radiation therapy or in cases of extensive scarring. However, the complexity of the operation increases the risk of complications, such as risk of flap failure and donor site morbidity, and requires longer operating time and increased postoperative care. In our case, due to multiple comorbidities, the patient was not suitable for prolonged anesthesia, making free flap or even regional flap reconstruction inappropriate.
Bilobed flaps offer significant advantages for patients. Compared to regional or free flaps, this technique shortens postoperative recovery time and reduces hospital stays without compromising flap survival or donor site healing. Additionally, it reduces discomfort associated with extensive wounds. The bilobed flap technique facilitates an inconspicuous donor site closure while ensuring adequate vascular supply, supporting reliable flap viability in a streamlined, single-stage repair. However, a limitation of the bilobed flap is its unsuitability for large defects (more than 6 cm), as inadequate blood flow at the flap intersection can lead to ischemia and necrosis. In our patient, the presence of systemic disease and compromised local circulation from prior neck dissection and CCRT posed unique challenges. Traditional local flaps and free flaps were not feasible due to the concern of defect size, the presence of scar and fibrous tissue, and the anesthesia time. To address these issues, we employed a bilobed flap, a technique typically reserved for facial and hand reconstructions, which resulted in a favorable outcome in this complex case by minimizing anesthesia risks while ensuring adequate coverage. One month postoperatively, the patient successfully underwent adjuvant radiotherapy without complications such as flap necrosis, ecchymosis, or contracture. Furthermore, neck extension and mobility remained largely unaffected. Before surgery, alternative regional flap options, including the deltopectoral and pectoralis major flaps, were considered. However, concerns regarding anesthesia time, postoperative aesthetics, and functional outcomes played a critical role in the decision-making process. Ultimately, the bilobed flap was chosen for its ability to provide both functional and aesthetic benefits in this challenging reconstruction. This case highlights the importance of a comprehensive understanding of anatomy, careful flap selection, and meticulous surgical planning in the management of soft tissue defects in the head and neck region.
In conclusion, we presented the case of a 65-year-old man with a regional recurrence of OC in the submental area. Following the wide excision of the metastatic soft tissue tumor, we utilized a bilobed flap for reconstructing the resulting defect. The patient achieved full closure of the neck wound, maintained neck mobility, and demonstrated a satisfactory cosmetic outcome. For moderate-sized neck defects, bilobed flap reconstruction is an effective option, particularly for patients who may not be suitable for prolonged anesthesia.
Footnotes
Author Contributions
Jiun-Yi Wu, Li-Jen Liao, and Wu-Chia Lo contributed to the conception and design of the study. Jiun-Yi Wu, Li-Jen Liao, and Po-Wen Cheng curated the data. Jiun-Yi Wu and Wu-Chia Lo wrote the first draft of the manuscript. Wu-Chia Lo supervised the concept and conducted the research. All authors contributed to manuscript revision and read and approved the submitted version.
Consent to Publish Statement
The written informed consent was obtained from the participant for publication of the details of their medical case and any accompanying images.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Study Approval Statement
This study protocol was reviewed and approved by Far Eastern Hospital, approval number: 113217-C.