
Abstract
Keywords
Introduction
The reconstruction of maxillofacial skin and soft tissue defects after resection has always been a challenge in oral and maxillofacial surgery. For small and medium-sized defects, various local flaps, such as rotary flaps, rhomboid flaps, double-lobed flaps, V-Y propulsive flaps, perforator propeller flaps, perforator island flaps, etc., are mainly used in clinical repair. 1 The advantages of such flaps are that the tissue quality, thickness, shape, and color are similar to the skin of the defect area, and the damage to the donor area is small. However, the auxiliary incision made by obtaining the flap is often not consistent with the wrinkle line or across the facial cosmetic subunit, resulting in irregular scars and affecting the postoperative facial beauty. The incision design is often complex and flexible; beginners should not master it. Since Behan 2 designed the keystone design perforator island flap (KDPIF) in 2003, the application of the KDPIF has been mostly reported in the trunk and limbs, while the application of the maxillofacial flap has been rarely reported. In recent years, we applied KDPIF to perform 16 cases of small and medium-sized soft tissue defects in different locations of the maxillofacial region in middle-aged and elderly people, and all achieved good results. The following reports are presented:
Methods
Clinical Data
General information
The 16 patients enrolled were all patients who underwent maxillofacial mass resection and applied KDPIF to repair maxillofacial soft tissue defects in the oral and maxillofacial surgery department of the Affiliated Hospital of Qingdao University from June 2021 to June 2023. There were 9 males and 7 females. Age: 49 to 93 years old, average 64 years old. Causes of soft tissue defect: there were 3 cases of benign lesions, including 1 case of common wart, 1 case of keloid, and 1 case of basal cell papilloma; there were 13 malignant lesions, including basal cell carcinoma (7 cases), squamous cell carcinoma (5 cases), and facial skin lymphoma (1 case). Soft tissue defects ranged from 1.0 cm × 1.5 cm to 6.0 cm × 5 cm. Defects: eyelid in 1 case, temporal in 1 case, cheek in 9 cases, upper lip in 1 case, nose in 1 case, infraorbital region in 2 cases, behind the ear in 1 case.
Surgical methods
Resection of the lesion
General or local anesthesia was selected according to the surgical site, surgical difficulty, and the patient’s general condition. Benign lesions with incision lines designed along the outer edge and the malignant tumor was completely removed according to the principle of no tumor. The safe boundary was the incision line was 1.0 cm away from the tumor edge, and intraoperative cryo-pathological examination was performed to ensure that there was no tumor residue at the resection margin and base.
Flap design
Variants of Type I and Type IIB KDPIF were designed based on the defect areas. The short side of the flap is close to the wound edge of the defect, and the top angle of both sides is 90° outward to the long bottom edge. If the tumor is located in a specific area of the jaw and face, to ensure the aesthetic appearance after defect repair or to avoid important structures around the defect, other angles can be designed based on facial wrinkle lines and facial aesthetic subunits. The width of the flap is 1:1 with the maximum width of the wound, and the flap is fan-shaped as a whole. Depending on the size of the tumor and the relaxation of the surrounding tissue, the flut-defect ratio can be expanded to more than 1:1. The designed incision line should be within the same cosmetic subunit as far as possible, and the blood supply vessels on the deep side of the deep fascia should not be damaged. After the tumor was removed, 3 edges of the flap were cut along the incision line, reaching the superficial layer of superficial musculoaponeurotic system (SMAS) or the superficial layer of the deep fascia of the neck. The superficial surface is separated from the periphery of the flap to the center, ensuring 30% to 35% of the flap attaching area to its bed (Figure 1).
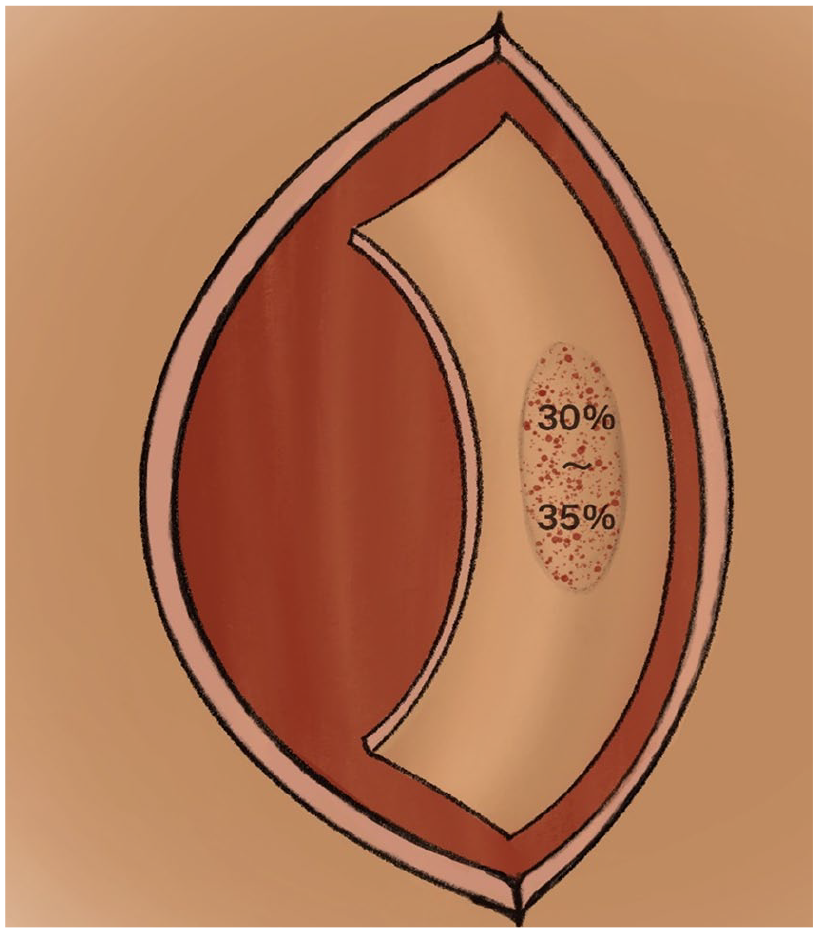
After the tumor was removed, 3 edges of the flap were cut along the incision line, reaching the superficial layer of SMAS or the superficial layer of the deep fascia of the neck. The superficial surface is separated from the periphery of the flap to the center, ensuring 30% to 35% of the flap attaching area to its bed.
Transfer and suture of the flap
After obtaining sufficient mobility of the flap, the flap was pulled toward the defect, and after the flap covered the defect wound with basically no tension, the flap was sutured to the defect first, and then V-Y propulsive suture was performed from both bottom corners to trim the “dog ears” formed by the 2 bottom corners, and the sutures were removed 1 week after surgery.
Postoperative management
For patients with large areas and dead space in the operative area, rubber drainage strips were placed on the deep surface of the flap; the drainage strips were removed within 24 to 48 hours according to the amount of leakage, antibiotics were applied prophylactically for 2 days, the operative area was kept warm, the blood flow of the flap was observed daily, stitches were removed 7 days after surgery, and follow-up was conducted at half a month, 1 month, 3 months, 6 months, 12 months, and 18 months after surgery.
Patients and public involvement
Neither patients nor the public was involved in the study.
Results
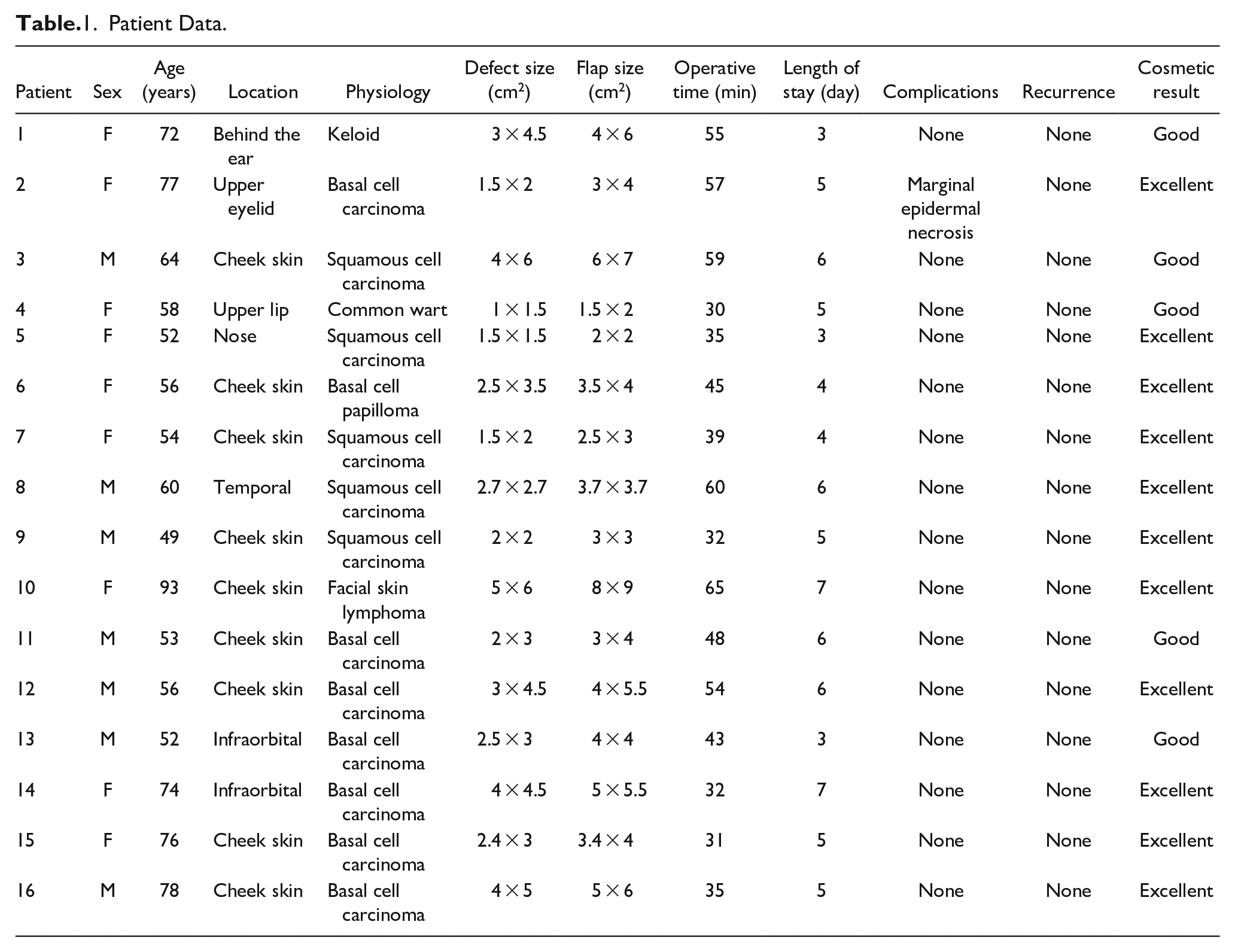
The operation time in this group was 30 to 70 minutes, with an average of 45 minutes. The hospital stay lasted from 3 to 7 days, with an average of 5 days. After surgery, 1 patient had dark red congestion and marginal epidermal necrosis within 1 week. After the dressing change, the color of the skin flap returned to normal 7 days later, and the incision healed 3 weeks later. All the patients survived, and the healing time was 1 to 3 weeks, with an average of 1.5 weeks. All 16 cases were followed up for 3 to 12 months (mean 6.5 months). For patients with keloids, we administered triamcinolone injections post-surgery, and no recurrence was observed during the follow-up period. There was no recurrence of tumor, no obvious scar clonus, and no facial dysfunction; the texture and color of the skin in the affected area were similar to the surrounding tissue, and the clinical effect was good (Table 1).
Patient Data.
Case 1
A 77-year-old patient with basal cell carcinoma of the upper eyelid. The patient was found to have a black painless swelling on the right upper eyelid for more than 10 years, which had recently grown rapidly. The right upper eyelid mass was excised along the outer edge of the mass. A 1.5 cm × 2 cm size defect was formed after resection of the tumor. Raise the flap (3 cm × 4 cm in size) to maximize the shape of the upper eyelid and successfully cover the defect (Figure 2a-c). Follow-up 12 months after surgery (Figure 2d), the flap heals well and the scar is concealed.

(a-d) Upper eyelid defect.
Case 2
Squamous cell carcinoma of right cheek skin in a 64-year-old patient. Ulcerated painful swelling on the right cheek for 4 months, with rapid growth of the swelling. Right buccal mass, 1.5 cm along the outer margin of the mass, all resection margins were negative. 4 cm × 6 cm size defect after resection of the tumor. Raised flap (6 cm × 7 cm size) to successfully cover the defect (Figure 3a-c). Follow-up 12 months after surgery (Figure 3d), the flap heals well, and the scar is concealed.

(a-d) Cheek defect.
Discussion
Maxillofacial trauma, tumors, and inflammation often lead to maxillofacial defects. However, how to reconstruct these defects has always been a challenging problem for clinical practitioners. The jaw and facial area involves numerous organs, and even minor changes can affect overall aesthetics. The 2 main goals of maxillofacial defect repair are to correct the dysfunction and restore or improve the appearance of the face. Although the facial defect hardly endangers the life of the patient, and usually the defect is not large, the repair and reconstruction are complex and significantly affect the facial function and aesthetics of the patient. For medium to small defects, various local flaps are mainly used in clinical repair. The advantages of these flaps are that their tissue quality, thickness, shape, and color are similar to the skin in the defect area, and they cause minimal damage to the donor area. The KDPIF was first described by Behan in the literature in 2003,2,3 where he mainly introduced the application of the flap in repairing soft tissue defects of the limbs and trunk. Subsequently, some scholars reported cases of KDPIF repairing facial defects of various sizes and locations, ranging from small defects on the nose to large defects in the parotid region.4-7 KDPIF has the advantages of convenient design, short surgery time, and good aesthetic results. This is a type of adjacent flap used to reconstruct facial defects. In this study, we introduced the concepts of facial wrinkle lines and facial aesthetic subunits into the KDPIF design, achieving excellent aesthetic results. Due to the lack of mature experience in the application of KDPIF to repair maxillofacial defects, middle-aged and elderly patients were selected in this group because these patients have relatively low requirements for facial beauty; in addition, their facial skin is more relaxed than that of young patients, and the range of flap movement is larger.8,9 In addition, the generation of age-related facial wrinkles can enable us to design the incision line in the wrinkles, and the scar is hidden after the recovery from surgery, which has little impact on facial beauty.
Behan’s classic classification of KDPIF has 4 subtypes 2 : Type I (skin incisions only), Type II (Type A, deep fascia divided along the outer curve; for type B, deep fascia was cut on the long side of the distal trapezoidal flap, and skin grafting was required in the donor flap area), Type III (wedge flap), and Type IV (double wedge flap). The Type I and Type IIB variants were applied in our study. These variants are generated after combining the concepts of facial wrinkle lines and facial aesthetic subunits. In 1956, Gonzales-Ulloa introduced the concept of facial aesthetic subunits, arguing that surgeons should strive to hide the surgical edge within the natural boundaries of each facial aesthetic subunit to achieve good aesthetic results. 10 Menick 11 et al found that if the incision sutures match the shape of specific subunits, the natural appearance of light and shadow can be restored, making the repaired scars imperceptible. 11 To avoid the flap design line crossing through the facial aesthetic subunits, we modified the short apex angle of the flap to a non-90° angle based on the location of the defect. All patients rated the aesthetic outcome as good or excellent during their 1-year postoperative follow-up. Notably, 2 cases of large defects (with sizes of 4 cm × 6 cm and 5 cm × 6 cm, respectively) also achieved excellent aesthetic results. Previously, KDPIF was applied to facial defects larger than 3 cm × 6 cm. However, without considering facial aesthetic subunits, the cosmetic effect may not be maximized.
KDPIF is a type of propulsive flap based on multiple perforating branches within the musculoderm or fascia. 12 The blood vessels of the subfascia or muscle layer should be designed in the center of the flap to obtain more perforating branches in the center of the flap and increase the blood perfusion of the flap. 13 In the preparation of KDPIF in the extremities and trunk, handheld Doppler ultrasound is usually used to determine the shape of intramuscular vessels and musculocutaneous perforating branches. Due to the abundant blood flow in the maxillofacial region, a large number of blood vessels send out enough perforator branches to supply the flap so that KDPIF can obtain reliable vascular perfusion. 13 Therefore, for maxillofacial defects, it is not necessary to locate the blood vessels and perforator branches during surgery. The area remaining attached to the bed in each flap (non-dissected) was called the pedicular area. 14 In a previous report, 89 patients underwent keystone flap restorations involving the trunk, extremities, and head and neck, with pedicular area ranging from 10% to 90%, with a 100% survival rate. 14 However, the design of the maxillofacial pedicular area has not been specified in the literature. Considering that the soft tissues of the maxillofacial region have a high degree of laxity, it is unnecessary to dissect up to 90% of the flap, and controlling the pedicular area to 30% to 35% can achieve a good blood supply and tension-free suture. In our study cohort, there was only 1 case of marginal epidermal necrosis postoperatively, and no flap dehiscence occurred. This indicates that controlling the pedicular area to 1/3 can provide sufficient blood supply and mobility.
Our series of case studies show that the application of KDPIF technology in the maxillofacial region has obvious advantages, such as simple design and easy to learn, adequate supply of blood vessels, short operation time, easy to form pathological scars, fast healing process, and matching with the surrounding skin color. For larger facial defects, using other adjacent flaps (such as rotary flaps and rhomboid flaps) often requires designing 2 flaps to cover the defect.11,14 The keystone flap only requires increasing the area of a single flap. Moreover, after integrating the concept of facial aesthetic subunits with KDPIF, reconstructing larger defects can achieve a good aesthetic outcome. The design of the skin flap should take into account the concept of facial wrinkle lines and facial aesthetic subunits. KDPIF can repair the defects of any maxillofacial cosmetic unit, especially suitable for middle-aged and elderly patients with small and medium-sized maxillofacial defects with maxillofacial skin relaxation and obvious wrinkles. In addition, in the maxillofacial region, the pedicle area accounts for 30% to 35%, which can achieve good blood supply and tension-free suture.
Conclusion
KDPIF technology has obvious advantages in the application of the maxillofacial region, which can repair the defects of any maxillofacial cosmetic unit, especially for small and medium-sized maxillofacial defects in middle-aged and elderly patients. We introduced the concepts of facial wrinkle lines and facial aesthetic subunits in the design of the flap, achieving a good aesthetic outcome. In addition, we designed the pedicle area of the flap to be approximately 1/3, which can achieve good blood supply and sufficient flap mobility.
Supplemental Material
sj-jpg-1-ear-10.1177_01455613241308727 – Supplemental material for Application of Keystone Design Perforator Island Flap in the Reconstruction of Maxillofacial Defect: A Case Series
Supplemental material, sj-jpg-1-ear-10.1177_01455613241308727 for Application of Keystone Design Perforator Island Flap in the Reconstruction of Maxillofacial Defect: A Case Series by Dongpo Li, Lin Wang, Yubo Wei and Shuangyi Wang in Ear, Nose & Throat Journal
Supplemental Material
sj-tif-2-ear-10.1177_01455613241308727 – Supplemental material for Application of Keystone Design Perforator Island Flap in the Reconstruction of Maxillofacial Defect: A Case Series
Supplemental material, sj-tif-2-ear-10.1177_01455613241308727 for Application of Keystone Design Perforator Island Flap in the Reconstruction of Maxillofacial Defect: A Case Series by Dongpo Li, Lin Wang, Yubo Wei and Shuangyi Wang in Ear, Nose & Throat Journal
Footnotes
Author Contributions
D.L.: Contributed to design, acquisition, analysis, and interpretation, drafted manuscript, and critically revised manuscript. Y.W.: Contributed to design, acquisition, and interpretation, drafted manuscript, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. L.W.: Contributed to analysis, and interpretation, drafted manuscript, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. S.W.: Contributed to design, acquisition, and interpretation, drafted manuscript, critically revised manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy. All authors gave their final approval and agreed to be accountable for all aspects of the work.
Consent for Publication
All the authors have consented to publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funed by National Natural Science Foundation of China “Study on the mechanism of EFNA3 induced oral squamous cell carcinoma regulated by KMT2D through H3K4me1/H3K27ac” (82203418).
Ethical Approval
This study protocol adhered to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Institutional Review Board of our University Hospital. Ethics No. QYFY WZLL 28277.
Informed Consent
Informed consent was obtained from each patient for this retrospective study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.