
Abstract
Cutaneous involvement of chronic lymphocytic leukemia (CLL) is rare but has been previously documented to involve the head and neck region. Generally, involvement to the ears is limited to the ear lobule; however, this study presents a unique case of recurrent CLL with cutaneous involvement overlying the auricular ear. The presentation was initially concerning for possible perichondritis but remained unresponsive to antibiotics and steroids. Eventual punch biopsy confirmed the recurrent CLL, although the lesion also presented with unique pathology, notably associated granulomata. This case demonstrates auricular involvement of CLL with unique pathology and highlights the importance of a widened differential and early, definitive tissue biopsy when evaluating refractory inflammation of the external ear.
Case
A 64-year-old male with a past medical history of chronic lymphocytic leukemia (CLL) and current prostate cancer workup presented to a community otolaryngologist for a worsening right auricular lesion. The patient first noticed the lesion 1 month prior and denied any inciting event or trauma. The lesion initially began with swelling, mild loss of cartilaginous contours of the ear, and mild erythema that spared the lobule (Figure 1A). This presentation was most concerning for external otitis or perichondritis; however, over the course of 2 months, the lesion continued to progress despite multiple rounds of antibiotic treatments (including levofloxacin, a cephalosporin, and clindamycin) and eventually progressed to develop an eschar overlying the scaphoid fossa (Figure 1B). Skin culture grew normal flora, and a superficial shave biopsy revealed fibrinous exudate and reactive squamous epithelium without evidence of malignancy. In addition to the eschar, swelling, and erythema, the patient endorsed tenderness to touch, but denied any hearing loss, vertigo, or any other otologic symptoms. There was no other cartilaginous involvement noted. The initial differential diagnoses included external otitis, autoimmune perichondritis, and malignancy. The community otolaryngologist referred the patient to our clinic for further evaluation.

Right auricular lesion when first presenting (A), 2 months later after eschar formation (B) and after in office punch biopsy (C) after treatment with obinutuzumab/venetoclax and radiation (D).
In clinic, debridement revealed de-epithelized granulation tissue with overlying exudate (Figure 1C). Two separate 4-mm punch biopsies through the underlying cartilage revealed dense CD20 and CD5+ B small cell lymphoma with associated granulomata (Figure 2A-D). The nuclei were dense and secondary structures such as prominent germinal centers were not identified, which are features typical of CLL (Figure 2B). The slides also showed significant expression of CD20 and CD5, consistent with the morphologic impression of a B-cell neoplasm (Figure 2C and D). The lymphocytes did not have significant expression of CD23 (Figure 2E), or of Cyclin-D1 or Sox-11 (not depicted), which confirm the diagnosis of CLL over other B-cell lymphomas such as marginal zone or mantle cell lymphoma.
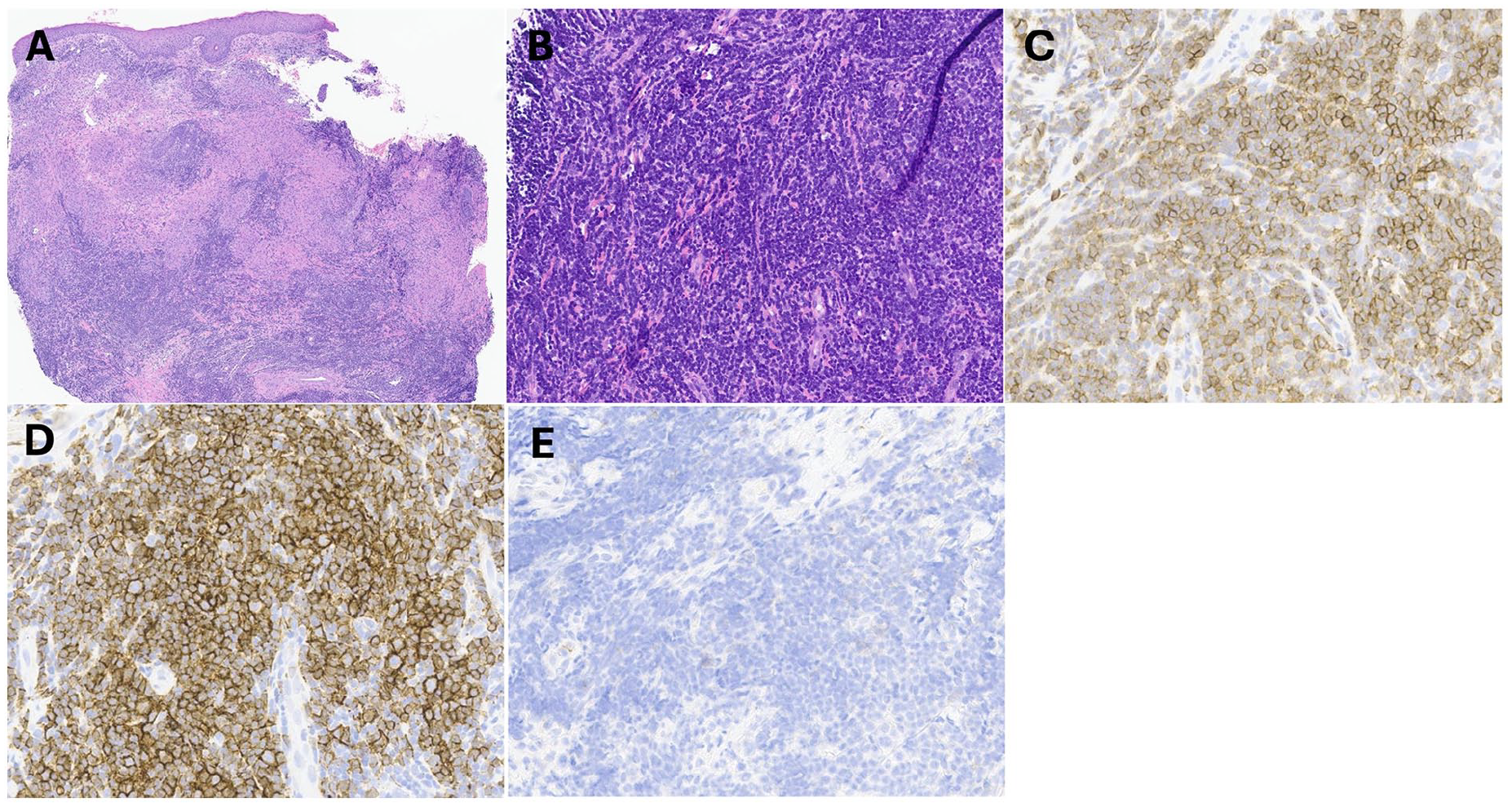
(A) There is a dense, sheetlike infiltrate of lymphocytes in the deep dermis, as well as numerous associated granulomata in the superficial dermis. (B) The lymphocytes are small and have scant cytoplasm, small nuclei, and condensed chromatin. (C) The lymphocytes have significant expression of CD20. (D) The lymphocytes have significant expression of CD5. (E) The lymphocytes do not have significant expression of CD23, or of Cyclin-D1.
Findings were consistent with CLL/small lymphocytic lymphoma and patient was started on obinutuzumab and venetoclax. The ear lesion continued to be raw and oozing despite treatment and was treated with silvadene. After 3 months of obinutuzumab/venetoclax as well as 2 cycles of radiation, patient reported some improvement in his ear lesion (Figure 1D).
Discussion
CLL is characterized by the uncontrolled proliferation of B-cell leukocytes leading to various complications such as anemia, coagulopathies, lymphadenopathies, and infiltration of impaired B cells into various tissues. Although CLL primarily affects the blood and bone marrow, there have been documented cases of cutaneous manifestations in individuals with previously-diagnosed CLL.1,2 Among the skin manifestations, malignancies such as basal cell or squamous cell carcinoma are the most common, likely secondary to the impaired immune response associated with CLL. 1 In rarer instances, CLL itself can present as a cutaneous lesion; however, when cutaneous manifestations do result, they are generally found incidentally after the diagnosis has been established. 2
Cutaneous manifestations involving the head and neck, specifically the ear, are rare; however, there have been reported cases of CLL involving the external ear.1,3-7 Notably, previous reports have mainly described involvement of the ear lobule, making our case especially unique. These past case reports also indicate that CLL of the external ears tends to manifest as more discrete nodules unlike the diffuse inflammation seen with our patient.5,7 While 1 report does demonstrate a case with pinna involvement of diffuse B-cell lymphoma, the lesion in this instance was not subtle and clearly reflected a malignant process. 8 On the other hand, our case highlights how cutaneous manifestations of CLL can also easily be mistaken for more common, benign processes such as perichondritis.
Furthermore, the pathological examination of the lesion revealed a distinct feature not commonly associated with CLL (Figure 2). In addition to CD20 and CD5+ B cells consistent with CLL, the pathology showed associated granulomas (Figure 2A). While this may have been secondary to reactive inflammatory changes, it is worth noting that there have only been 2 documented cases of CLL associated with granulomas in the literature.9,10 In both cases, the cutaneous lesions observed differed from the generalized inflammation and eschar seen in our case. The clinical significance of this unique pathology has not yet been established given its rarity; however, documentation of this phenomenon can help to strengthen the association between CLL and granulomas as well as offer insight into the unique cutaneous presentation of CLL.
Ultimately, this case highlighted the importance of performing a thorough deep punch biopsy (through the cartilage but not all the way through the skin of the posterior auricle) in cases of external otitis that are not responding to antibiotics. The superficial shave biopsy that was originally taken did not yield a diagnosis and, in this case, may have offered false reassurance. While some may be reluctant to perform a punch biopsy, this case highlights that the biopsy sites heal very well (Figure 1D), and sampling the perichondrium and cartilage is critical in order to diagnose perichondritis or cartilage invasion of malignancy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Signed informed consent was obtained from the patient for this written case report (can be uploaded with submission if requested or required).