
Abstract
Objectives:
The mainstay of cholesteatoma treatment is surgical and requires the removal of all squamous epithelium from the underlying normal structure. The application of laser technology in middle ear and mastoid surgery has shown promise in achieving both disease eradication and hearing preservation. This systematic review aims to include studies that have assessed the application of laser to the treatment of cholesteatoma and to review its outcomes in terms of disease eradication as well as hearing results.
Method:
Two independent researchers conducted a systematic review of the literature on MEDLINE and Cochrane library, according to PRISMA guidance.
Result:
The search resulted in 12 papers, reporting on 536 participants that fulfilled the inclusion criteria. The hearing results did not show that using laser surgery improved hearing in cholesteatoma surgery, but neither has the use of laser shown to deteriorate hearing. With regards to the prevention of residual/recurrent cholesteatoma, the current literature reports a residual/recurrent rate of 0% to 33%. The complication rate of facial palsy is 0.6%.
Conclusion:
While there is certainly a role for future studies especially randomised large-cohort prospective comparative studies, the current literature suggests that laser may have a role in prevention or minimizing of residual cholesteatoma and generally have a safe hearing outcome profile.
Introduction
Cholesteatoma is a collection of squamous epithelium with potential to cause progressive erosion and destruction of important structures within the temporal bone. The mainstay of treatment for this disease is surgical and requires the removal of all squamous epithelium from the underlying normal structure. While the prime objective of mastoid surgery for cholesteatoma is complete disease removal, creating a safe, dry, and disease-free ear, 1 preservation of hearing is also one of the important objectives. Traditionally, mastoidectomy techniques can be classified into 2 main categories: canal wall down and canal wall up. In recent times, a variety of surgical modifications have been developed and techniques such as transcanal endoscopic ear surgery 2,3 and laser-assisted cholesteatoma surgery have been applied.
The application of laser technology in middle ear and mastoid surgery has shown promise in achieving both disease eradication and hearing preservation. This systematic review aims to include studies that have assessed the application of laser to the treatment of cholesteatoma and to review its outcomes in terms of disease eradication as well as hearing results.
Methods
The systematic review was undertaken in accordance with the general principles recommended in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 4 A systematic computer-based literature search was performed on the biomedical bibliographic databases: MEDLINE and Cochrane library. The search was performed by 2 independent researchers and included the search terms: “(cholesteatoma) AND (laser)” with the filters: “Text availability: Full Text,” “Species: Humans,” and “Language: English.”
Inclusion and Exclusion Criteria
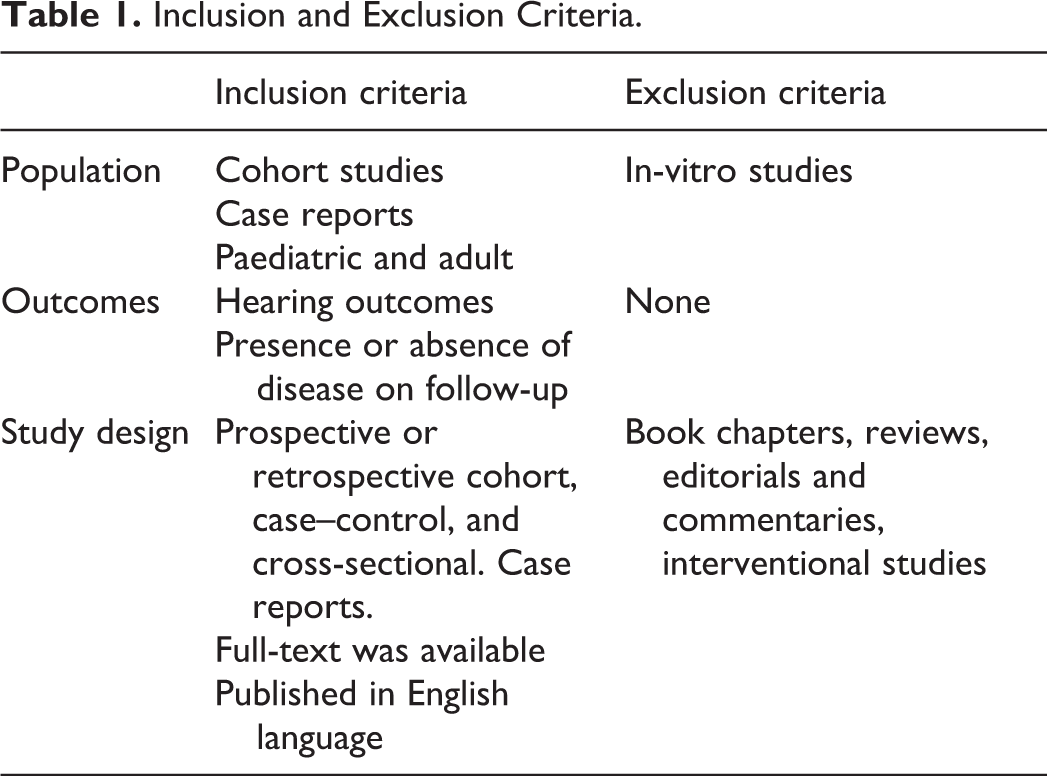
The inclusion and exclusion criteria for the population of interest, outcomes, and study design are presented in Table 1.
Inclusion and Exclusion Criteria.
Data Analysis
Two authors (K.L. and M.S.) independently selected studies, extracted data, and assessed the quality of included studies. Data were extracted from each study and included information on the article identification, year of publication, population (continent), evaluation period (for longitudinal studies), number of patients, hearing assessment methods, residual or recurrent cholesteatoma outcomes, and mean age of subjects.
Results
The electronic searches identified 44 citations. Of these, 28 were excluded after reviewing their title and abstract. Of the remaining 16 citations obtained as full-text, 4 were excluded as they were review papers. 1,5 -7 Twelve studies, reporting on 536 participants, fulfilled the inclusion criteria and were included in the systematic review. A PRISMA flowchart of the study selection process is shown in Figure 1.
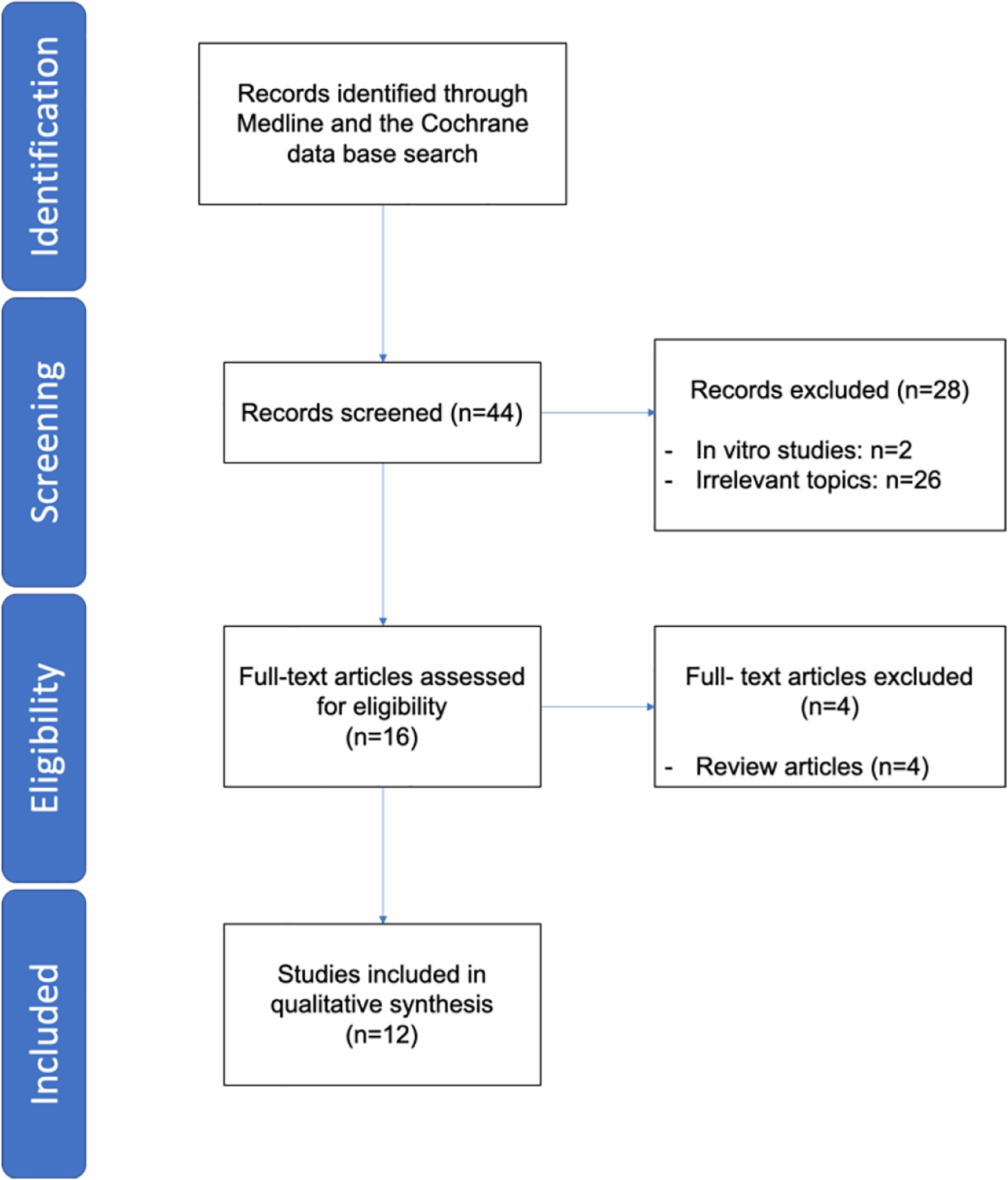
Flowchart of the study selection process.
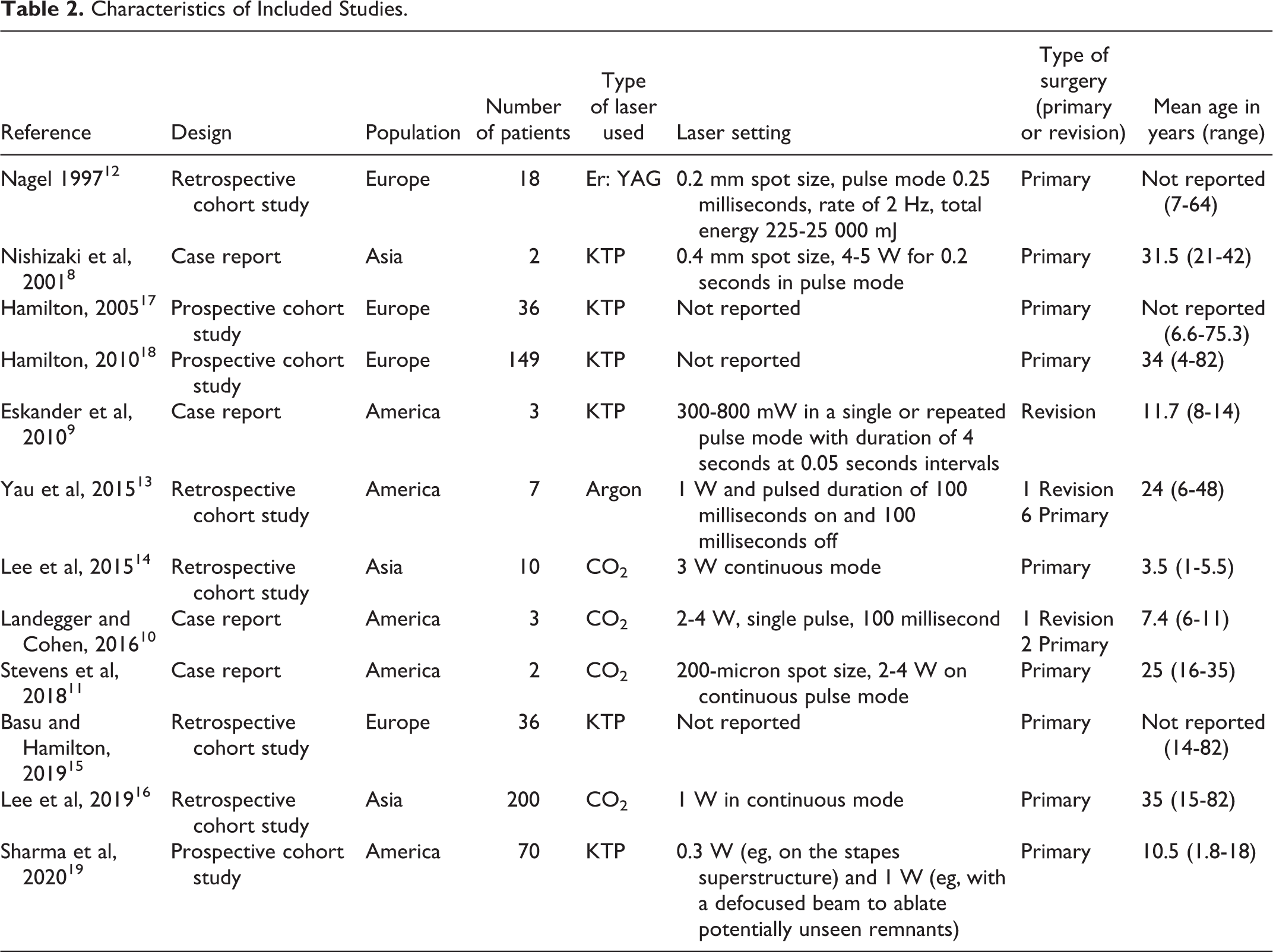
The characteristics of the included studies are shown in Table 2. These studies were published between 1997 and 2020 and conducted in America, Asia, and Europe. Four of them were case reports, 8 -11 5 were retrospective cohort studies, 12 -16 and 3 were prospective cohort studies. 17 -19 Recruited participant numbers ranged from 2 8,11 to 200. 16
Characteristics of Included Studies.
Application of Laser and Reported Complications
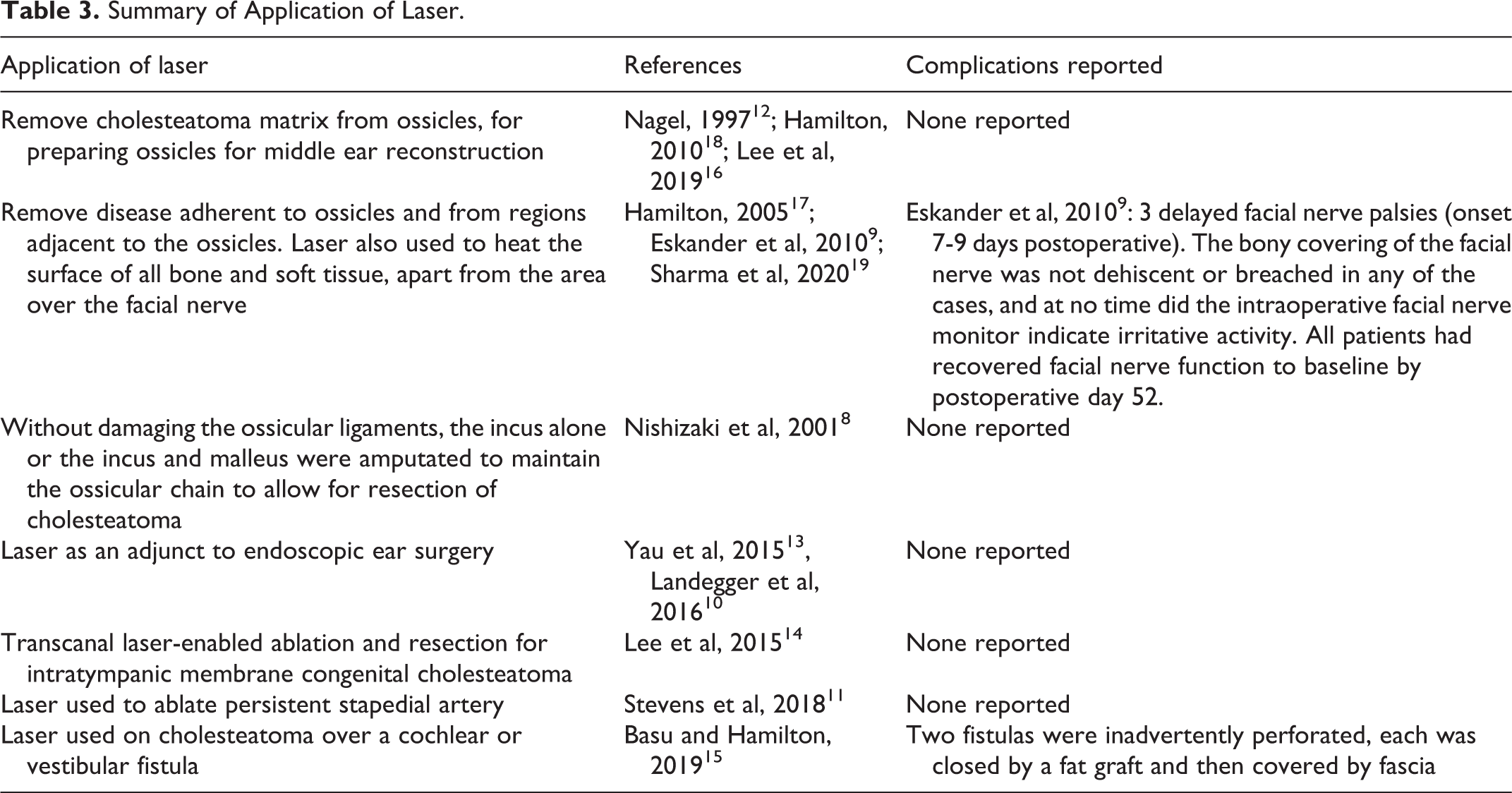
Table 3 summarizes the different ways laser was applied in surgery in all groups.
Summary of Application of Laser.
Hearing Results
Hearing results were not reported in 4 papers. 9,10,13,19 Hearing thresholds were reported using either pure tone audiogram results, bone conduction thresholds only, or distorted product otoacoustic emission (for children). Because of the heterogeneous way of reporting hearing outcomes, it was not possible to compare hearing outcomes in different groups. Table 4 shows a summary of hearing outcomes and in general, any worsening of hearing was limited to a range of deterioration between 0.3 to 15 dB.
Hearing Outcomes.
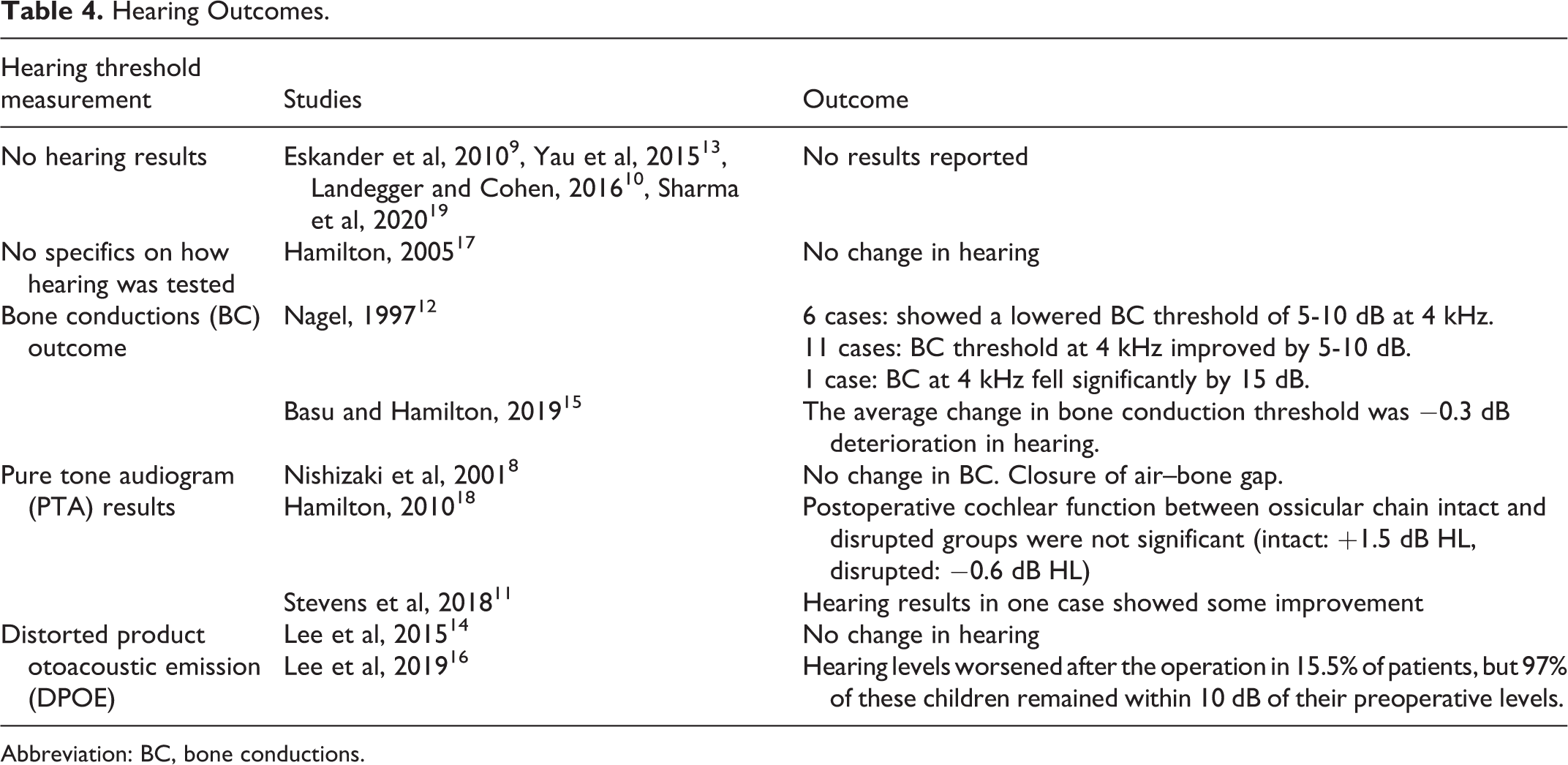
Abbreviation: BC, bone conductions.
Disease Eradication
As part of their outcome measure, 9 papers 10,11,13 -19 looked at the presence or absence of residual disease at either a second stage operation, with diffusion-weighted magnetic resonance imaging or computed tomography scan at least 12 months after the first operation or clinical observation. There were 2 papers that had a control group and compared the outcomes of laser versus no laser, while Hamilton in 2005 17 showed that using a laser significantly reduced the chance of residual disease after 12 months, Sharma et al in 2020 19 did not report any significant difference between using the laser or not. The other papers report their recurrence rate between 0% and 33%. 10,11,13 -16,18 Table 5 summarized the disease eradication outcomes.
Disease Eradication Outcomes.
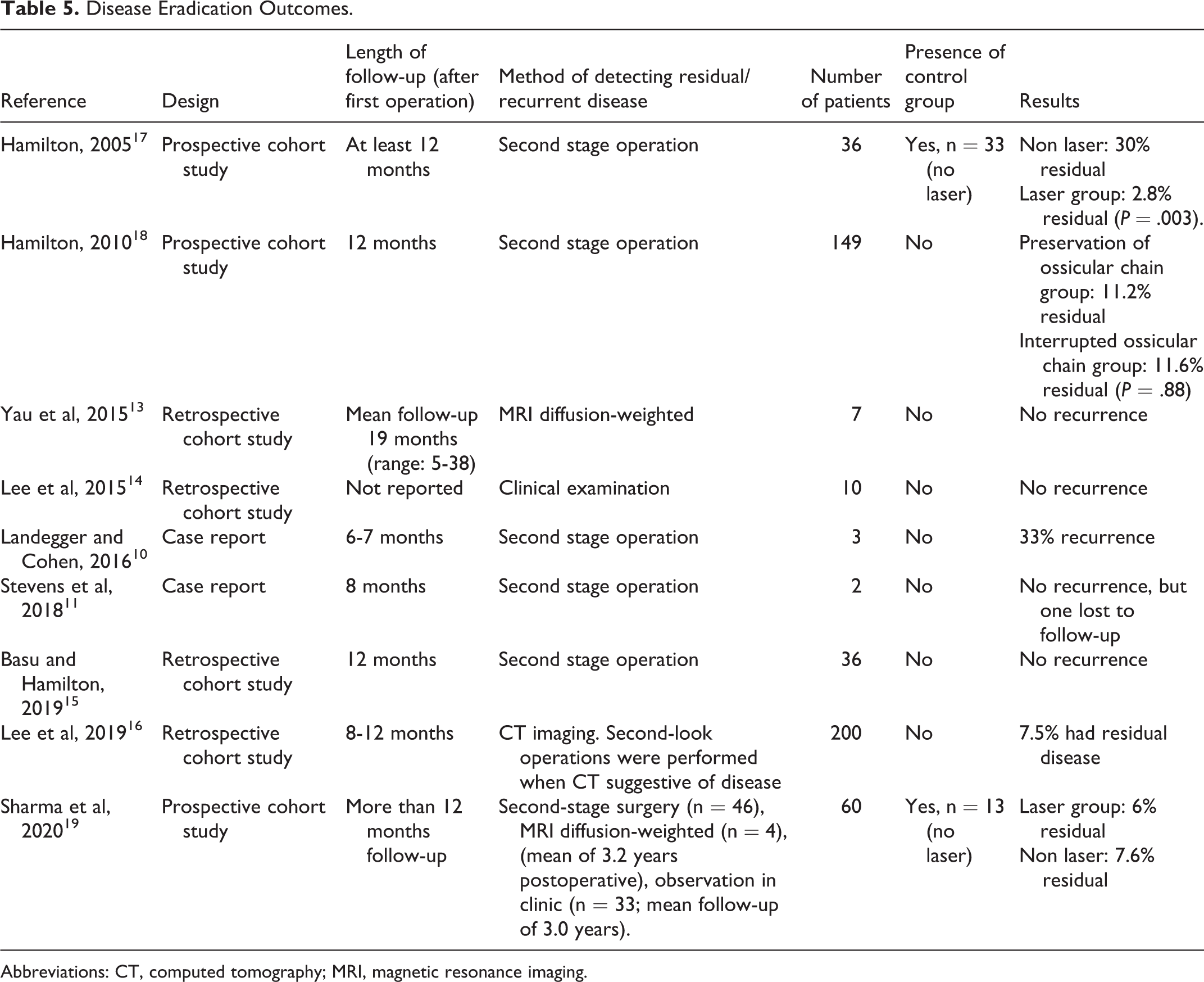
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging.
Discussion
In the last 2 decades there have been a variety of publications looking at the outcomes of laser on cholesteatoma surgery. Majority of them have been nonrandomized retrospective cohort studies and case reports, with very few large longitudinal cohort studies with a control group.
While laser surgery is thought to facilitate atraumatic dissection of cholesteatoma from mobile ossicles and therefore reducing the risk of trauma to the cochlea from mechanical traction, there has only been one study 18 that compared the outcomes from 2 groups that were treated with laser (patients with ossicular chain intact vs disrupted). The hearing results did not show that using laser surgery improved hearing in cholesteatoma surgery, but neither has the use of laser shown to deteriorate hearing.
With regard to the prevention of residual/recurrent cholesteatoma, the current literature reports a residual/recurrent rate of 0% to 33% with 2 prospective papers comparing between a laser and nonlaser group. A single well-designed comparative study has shown sufficient benefit to lead to the claim that KTP laser use in cholesteatoma surgery has been shown to reduce the risk of residual cholesteatoma with a number needed to treat of 4 cases. 17 However, the follow-up duration of the studies mentioned in this review has not been sufficient to provide a dependable assessment regarding the longer-term effects of laser-assisted surgery on the recidivism of cholesteatoma, which is a time-dependent phenomenon. Continued long-term vigilance in this regard is therefore recommended.
Even though there were a variety of lasers being reportedly in use, there was no evidence portraying any laser as being ineffective at removing cholesteatoma. There have also been no studies directly comparing the different types of laser and any difference in clinical outcomes. Facial palsy is a potential complication of laser-assisted surgery and most papers recommend not applying laser to anywhere near or directly to the facial nerve. Combining all the cases together, the complication rate of facial palsy was 0.6%.
While there is certainly a role for future studies especially randomised large-cohort prospective comparative studies, the current literature suggests that laser may have a role in prevention or minimizing of residual cholesteatoma and generally have a safe hearing outcome profile.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.