
Abstract
Introduction
Military personnel are a high-risk group for acute hearing loss, commonly caused by acoustic trauma. 1 Acute acoustic trauma (AAT) is a clinical condition characterized by immediate and/or persistent hearing loss following exposure to impulse or blast wave noise. 2 This condition is frequently observed in the military as a result of gun shooting training or sudden explosions. Common sequelae include tinnitus, vertigo, and acute hearing loss, which typically resolve within a few days. 3 However, these symptoms can also become chronic and permanent, causing both physiological and psychological problems for veterans post-service. 4 In the French military, the prevalence of long-term hearing loss following AAT was reported to be greater than 20%. 5
In addition to acute hearing impairments caused by AAT, various forms of sudden hearing loss can also occur.6,7 Sudden sensorineural hearing loss, also known as sudden deafness, is defined as a rapid 30 dB decrease in 3 continuous hearing frequencies and may be associated with accompanying vertigo and tinnitus. Approximately 80% to 85% of cases occur without an identifiable cause, a condition referred to as idiopathic sudden sensorineural hearing loss (ISSNHL), and the remaining 15% to 20% may be attributed to factors such as viral infections, vascular thrombosis, cellular pressure in the cochlea, immune dysregulation or trauma. AAT can also be a cause of sudden hearing loss. However, establishing a clear association between these factors and sudden hearing loss is challenging and often based on medical history and clinical presentations.
Our study examined the characteristics of gunshot–related AAT among military personnel, including the interval between trauma and treatment initiation, accompanying symptoms, and hearing thresholds before and after treatment. We compared AAT with ISSNHL among military personnel for the same period to identify the factors influencing prognosis in acute hearing loss.
Materials and Methods
For this retrospective chart review, data was collected between 2009 and 2021 from the Tri-Service General Hospital in Taiwan, a tertiary center for active-duty enlisted personnel, non-commissioned officers, and officers. All military personnel undergoing pure tone audiogram (PTA) for reasons such as tinnitus, vertigo, hearing impairment, or routine checkups were reviewed. Cases of acute hearing loss, defined as a decrease in hearing compared with the unaffected ear or previous audiogram or self-reported sudden hearing loss, with hearing threshold levels exceeding 30 dB at 2 continuous audiometric frequencies, were included in the study.
The exclusion criteria were (1) onset time of hearing loss greater than 30 days, (2) sudden hearing loss with an identifiable cause (such as viral infection, autoimmune disease, ototoxic medication use, or Meniere’s disease), (3) acoustic trauma unrelated to gun shooting training (in AAT group), and (4) tympanic membrane perforation or otitis media. Military regulations require all soldiers to wear ear protection (3M 1100 Earplugs) during gun shooting practice.
The remaining cases were divided into AAT and ISSNHL groups. The AAT group included individuals who experienced subjective hearing loss immediately after gun shooting training. The ISSNHL group included individuals who experienced sudden hearing loss, defined as sensorineural hearing loss of at least 30 dB affecting 3 continuous audiometric frequencies occurring within 72 hours. No patients in this group had been exposed to gunshot noise within 72 hours of hearing loss onset, but they may have previously participated in gun shooting training.
Systemic oral steroid therapy (1 mg of prednisolone per 1 kg of body weight) was administered for 2 to 3 weeks in accordance with the 2019 AAO-HNS guidelines on sudden hearing loss. 8 Hyperbaric oxygen therapy (HBOT), which improves vascular compromise and associated cochlear ischemia (a potential etiology of ISSNHL), and intratympanic steroid injection (ITSI), which enhances steroid concentration through middle ear diffusion into the cochlea, are increasingly recommended as optional treatments.3,9-11 The route of steroid administration and adding optional therapies were based on the severity of hearing loss, patient receptivity, and the physicians’ clinical assessment. In our present study, 76 patients (21 of 53 total cases in the AAT group and 55 of 58 total cases in the ISSNHL group) were treated with 7 days of intravenous steroid (betamethasone tapered from 12 to 4 mg/day per 60 kg of body weight) during hospitalization. Additionally, 4 patients in the AAT group and 2 patients in the ISSNHL group received ITSI. Five patients in the AAT group and 20 patients in the ISSNHL group received HBOT. All patients underwent follow-up PTA within 6 months.
All PTA assessments were conducted by the same team of audiologists in a certified soundproof room and examined 5 audiometric frequencies (500, 1000, 2000, 4000, 8000 Hz). The initial average PTA data indicate disease severity at the first visit, whereas the final average PTA data indicate hearing threshold after treatment. The difference between the 2 datasets was calculated and represented as hearing gain.
Statistical analysis was performed using IBM SPSS Statistics version 22 software (Armonk, NY, USA; IBM Corp.), with a significance level of .05. We used the chi-squared test for dichotomous variables and the Mann-Whitney U test for continuous variables to determine the equivalence of baseline characteristics. A paired t-test was used to assess treatment efficacy, and the Mann-Whitney U test was used to compare hearing recovery outcomes between the AAT and ISSNHL groups. To evaluate the impact of covariates, 2 models were developed: model 1 was adjusted for gender, age, and time to treatment initiation, and model 2 was adjusted for gender, age, time to treatment initiation, and disease severity. We assessed these models using linear regression analysis with enter method and set .05 as the significance threshold.
Results
From 2009 to 2021, 4225 military personnel who underwent PTA were enrolled, among whom 118 individuals were included based on a history of acute/sudden hearing loss and PTA results showing a hearing threshold above 30 dB at 2 consecutive frequencies. At acute hearing loss onset, the hearing thresholds of the unaffected ear were within the normal range (<20 dB) across all frequencies in 102 individuals, whereas 9 individuals had experienced one or more instances of high-frequency hearing loss (3 in the AAT group and 6 in the ISSNHL group). We excluded 5 individuals whose disease onset time exceeded 30 days, one whose acoustic trauma was non-gunshot-related, and another who was diagnosed with Meniere’s disease, leaving 111 eligible participants. These were divided into an AAT group (53 individuals) and an ISSNHL group (58 individuals) based on their medical history of exposure to gunshot–related noise (Figure 1).
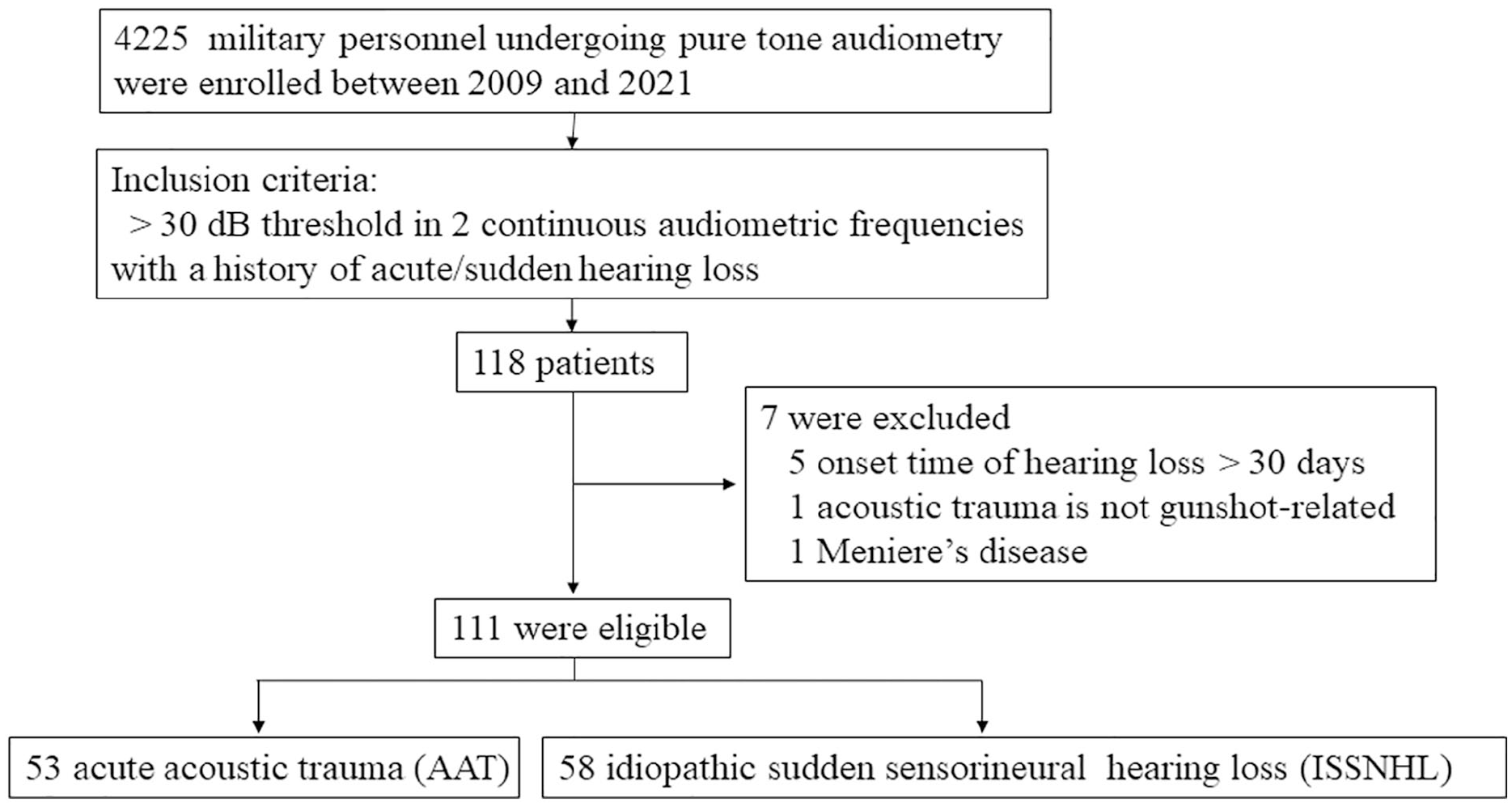
The flowchart of study sample collection.
Table 1 shows the mean age of all participants as 26.7 years old, with an average of 23.7 years old for the AAT group and 29.5 years old for the ISSNHL group. Males constituted 92.8% of participants (103 individuals). In the AAT group, left ear hearing loss was predominant in 66% of cases, compared with 55.2% in the ISSNHL group. The average time from symptom onset to treatment was 8.96 days in the AAT group and 4.6 days in the ISSNHL group. All patients in the AAT group experienced tinnitus (100%), but few reported vertigo (5.7%). By contrast, the ISSNHL group had a lower incidence of tinnitus (84.5%) but a higher incidence of vertigo (36.2%).
Characteristics of 111 Participants in the Retrospective Study.

Abbreviations: AAT, acute acoustic trauma; ISSNHL, idiopathic sudden sensorineural hearing loss.
Mann-Whitney U test.
Chi-Squared test.
The audiograms with average initial and final PTA results for both the AAT and ISSNHL groups are shown in Figure 2. The initial PTA results indicated that AAT-induced hearing loss primarily affected the high-frequency range, which was also where the greatest improvements post-treatment were observed, with an average improvement of 20.2 dB at 4000 Hz and 11.0 dB at 8000 Hz. By contrast, the ISSNHL group was affected across all audiometric frequencies, with hearing thresholds ranging between 64.2 and 72.5 dB, and exhibited more uniform recovery, with the best improvement at 1000 Hz (29.1 dB) and the least at 8000 Hz (19.3 dB). Follow-up audiograms showed that the AAT group exhibited better recovery in the high-frequency area while maintaining stability in the low-frequency area, whereas the ISSNHL group showed improvement across all frequencies, with both groups’ curves shifting upwards but slope remaining roughly unchanged.
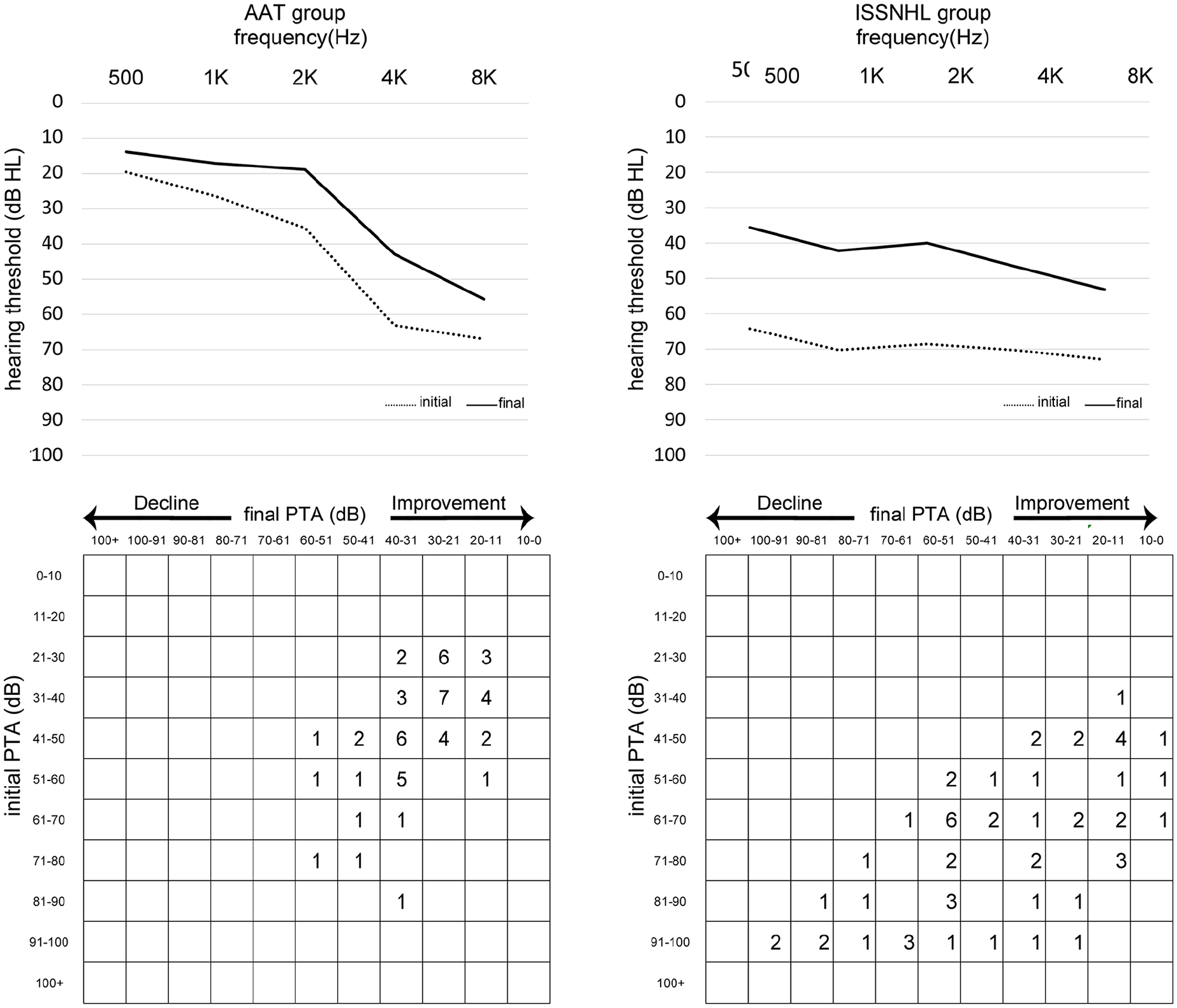
Initial and final PTA average was shown and scattergram demonstrated the number of patients with their respective initial and final PTA in the AAT and ISSNHL groups.
We also analyzed hearing recovery at each audiometric frequency within the AAT and ISSNHL groups, as detailed in Figure 3A and B. Although both groups showed hearing recovery across all frequencies after treatment, the AAT group exhibited poorer recovery, as shown in Figure 3C. This difference was statistically significant (P < .01) at 500, 1000, and 2000 Hz but not at 4000 or 8000 Hz.

Comparison of initial and final PTA results in the AAT (A) and ISSNHL (B) groups and of hearing recovery after treatment between both groups (C). Δ: hearing recovery = initial − final hearing threshold.
We designed 2 models to adjust for the effects of gender, age, time to treatment initiation, and disease severity, detailed in Table 2. Our initial model was focused on average threshold hearing recovery and indicated that the AAT group had a poorer prognosis, aligning with the results shown in Figure 3C. After adjusting for gender, age, and time to treatment initiation in model 1, results remained statistically significant. However, once model 2 adjusted for disease severity, the results did not reach statistical significance, indicating that disease severity is the main prognostic factor for recovery of both idiopathic hearing loss and that caused by acoustic trauma.
The Comparison Outcomes of the Hearing Recovery Between AAT and ISSNHL Group, Adjusted for Gender, Age, Time to Treatment Initiation and Disease Severity.

Δ: hearing recovery = initial − final hearing threshold. B: B value, unstandardized coefficient.
Abbreviations: AAT, acute acoustic trauma; ISSNHL, idiopathic sudden sensorineural hearing loss.
Model 1: adjusted for gender, age, and time to treatment initiation.
Model 2: adjusted for gender, age, time to treatment initiation, and disease severity.
Linear regression.
Discussion
Military personnel are particularly susceptible to acoustic trauma due to their profession. In the Finnish Defense Forces, 90% of all AAT-induced hearing loss was caused by noise from rifle-caliber weapons. 12 In our experience, about 5% of military personnel in Taiwan have consulted a physician for weapon-related AAT. 13 Data from both the industrial and military sectors indicate that damage from impulse noise is more severe than that from continuous noise with equivalent total acoustic energy. 14 Moreover, ATT-induced hearing loss and tinnitus can become permanent, leading to physiological and psychological challenges for veterans post-service.5,15 For more than a decade, pervasive noise-induced hearing loss and tinnitus have consistently been the second-most prevalent service-connected disabilities for US veterans receiving compensation.16,17 Thus, our study explored the characteristics, symptoms, and prognosis of acoustic trauma among military personnel in Taiwan to inform future diagnostic and treatment strategies.
Military personnel undergo health screenings upon enlistment to rule out specific concerns, theoretically reducing potential health problems.18,19 Therefore, our study focused on 2 primary groups of military personnel with acute hearing loss: those affected by AAT and those by ISSNHL. These groups represent the majority of hearing loss cases in the military and share similar treatment strategies, prompting our interest in understanding the differences in their prognosis. 20 The mean age of our study participants was relatively young, averaging 23.7 years old among the AAT group, possibly reducing the likelihood of concurrent chronic illness that could impact hearing. Two-thirds of the 53 AAT group participants suffered left ear damage, consistent with previous studies indicating a predominance of noise-induced hearing loss in the left ear in military contexts, which may be the result of shooting posture asymmetry. Given that most people are right-handed, the right ear is typically tilted away from the muzzle and partially shielded by the head from the muzzle sound. Another possible explanation is intrinsic differences between both ears. 19 In our study, all cases of AAT presented with tinnitus at the time of trauma, while vertigo was less common, affecting only 5.7% of participants.
Initial PTA results indicated that AAT-induced hearing loss primarily affected the high-frequency range, in contrast to ISSNHL, which affected all frequencies. 17 Following treatment, both groups exhibited overall hearing improvement, and a detailed analysis indicated statistically significant improvements across all frequencies, as shown in Figure 2. A further comparison of post-treatment hearing recovery levels between both groups indicated a poorer prognosis in the AAT group. However, a linear regression analysis that controlled for gender, age, time to treatment initiation, and disease severity indicated that prognosis primarily depended upon the severity of hearing loss at the time of injury, regardless of whether it was caused by acoustic trauma or idiopathic factors.
Age did not influence AAT prognosis, which is consistent with findings in previous studies. 21 This finding suggests that individuals of all ages are vulnerable to acoustic trauma, highlighting the necessity for hearing protection measures to be universal rather than based on age. Additionally, our study found that the interval between trauma and treatment initiation did not significantly affect overall hearing outcomes. Nevertheless, in model 1, the P values for hearing recovery at 2000 and 8000 Hz exceeded .05, suggesting that at higher audiometric frequencies, the timing of treatment initiation becomes more critical than whether the hearing loss is due to AAT or ISSNHL. This finding aligns with those of Harada, which indicated that prompt treatment after acoustic injury was associated with partial hearing recovery.
Table 1 shows that the average time to treatment initiation was 8.96 days in the AAT group, which was higher than the 4.6 days in the ISSNHL group, suggesting that AAT may be easily overlooked, leading to a delay in treatment. Thus, physicians should be more vigilant and actively educate the military to prioritize early to treat hearing damage caused by shooting practices.
Our study compared the characteristics and prognoses of AAT and ISSNHL because both conditions are managed with similar therapeutic modalities. However, our findings indicated that condition type, whether AAT or ISSNHL, did not primarily influence acute hearing loss outcomes among military personnel. Instead, the severity of the condition emerged as a pivotal factor, corroborating our existing insights into AAT. 22 Harada was the first to reveal that poorer outcomes are associated with worse high-frequency hearing thresholds, although this conclusion has been challenged by subsequent research. 21 Similarly, our study evaluated AAT prognosis while controlling for extrinsic factors. We based our assessment of disease severity on the average hearing threshold across all frequencies to emphasize differences in overall hearing capability. A more detailed investigation of the features across various audiometric frequencies has the potential to substantially enrich our knowledge in this area.
The strength of this study is that our population is specific to military personnel, regardless of whether the cases are related to AAT or ISSNHL. However, our study had several limitations. Firstly, the retrospective, single-institution design may have led to sample bias and selection errors. Our individuals are military populations and more younger men, the results can not represent and compare to the general population. Second, we did not conduct hearing tests at 3000 and 6000 Hz frequencies, commonly affected by acoustic trauma. Third, we did not collect data on potentially relevant lifestyle habits such as smoking, alcohol consumption, betel nut chewing, obesity, or sleep deprivation. Finally, we did not adjust extra models to account for the effect of different treatment protocols. The treatment protocol may be varied in different hospitals/countries and may not be considered as a standard of care to reproduce the results. In the future, we will collect more patients to clarify the correlation between different treatment protocols and prognosis among these 2 groups of patients.
Conclusion
Our comprehensive analysis of military personnel experiencing AAT and ISSNHL underscores the effects of acute hearing loss and associated symptoms in this high-risk group. In our study, military personnel with AAT typically experienced asymmetric high-frequency hearing loss, predominantly in the left ear, along with tinnitus, and the average time from trauma to treatment was 9 days. AAT and ISSNHL share similar treatment strategies, and our study found that their prognosis is primarily determined by the severity of the condition at the time of injury, rather than whether hearing loss was caused by acoustic trauma or idiopathic factors. These insights provide a valuable foundation for future diagnostic and treatment strategies, highlighting the importance of prompt and accurate assessment of hearing loss severity to achieve optimal recovery outcomes for military personnel facing the challenges of AAT and ISSNHL.
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions of their colleagues.
Author Contributions
Ting-Li Hung analyzed the data and drafted the original manuscript. Chih-Hung Wang supervised and reviewed the manuscript. Shu-Chu Cheng collected the data. Hsin-Chien Chen designed the study and editing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a grant from the Tri-Service General Hospital (TSGH-A-113006 to H.-C. Chen), National Science and Technology Council, Taiwan (NSTC 113-2314-B-016-010 to H.-C. Chen), the Teh-Tzer Study Group for Human Medical Research Foundation (B1131005 to C.-H. Wang and H.-C. Chen), and Medical Affairs Bureau, Ministry of National Defense, Taiwan, ROC (MND-MAB-C12-113043 to H.-C. Chen).
Institutional Review Board (Human Subjects)
This retrospective study obtained approval from the Institutional Review Board of Tri-Service General Hospital (IRB approval number: B202305136).