
Abstract
Objective:
The aim of this study was to determine the incidence of inner ear involvement in various forms of acute otitis media (AOM) in ear, nose, and throat (ENT) practices in Germany.
Methods:
Patients who had been diagnosed with various forms of AOM in the years 2010 to 2017 were enrolled in the study from a nationwide, representative practice database (Disease Analyzer, IQVIA). In these patients, the incidence of simultaneous or subsequent inner ear disorders (IED) was determined within 7 days and within 12 months from the date of an AOM diagnosis.
Results:
A total of 286 186 patients with AOM were enrolled. The most frequent diagnoses were “nonsuppurative otitis media, unspecified” (47.6%) and “otitis media, unspecified” (39.0%). The diagnoses of hemorrhagic bullous myringitis (BM) or influenza-induced AOM were very rarely found in the database. The highest incidence of IED after 7 days and 12 months was found in “nonsuppurative otitis media, unspecified” (7.7% and 15.9%, respectively), followed by “otitis media, unspecified” (5.6% and 13.5%, respectively). The incidences of the most frequent IED “hearing loss, unspecified” and “sensorineural hearing loss, unspecified” increased proportionally with increasing patient age, while the rare diagnoses of “labyrinthitis” and “ototoxic hearing loss” were evenly distributed among the age groups.
Conclusion:
In ENT practices in Germany, both various forms of AOM, as well as simultaneous or subsequent IED, are mostly being coded in an unspecific way, while specific forms such as hemorrhagic BM, influenza-induced AOM, and labyrinthitis are coded very rarely. Older patients have a higher risk of IED in AOM. A visit due to AOM seems to be a regular occasion for the initial diagnosis of hearing impairment in the elderly individuals. The highest risk of IED was found in nonsuppurative AOM.
Keywords
Introduction
Acute infections of the middle ear (acute otitis media [AOM]) are among the most frequent causes worldwide for the use of medical care and the prescription of drugs (annual incidence in 2005: globally 10.9%, North America and Central Europe 5%-7%) 1 and represent a relevant proportion of the patient population in ear, nose, and throat (ENT) practices in Germany. In the first quarter of 2017, the statistics of the North Rhine Association of Statutory Health Insurance Physicians (Kassenärztliche Vereinigung Nordrhein) ranked nonsuppurative otitis media (ICD group H65) in 10th place, with 7.8%, and suppurative and unspecified otitis media (ICD group H66) in 17th place, with 4.5% of the most frequent diagnoses in ENT practices. 2 Bullous myringitis (BM), which is clinically characterized by serous and/or hemorrhagic blisters on the tympanic membrane, is a particular manifestation in the spectrum of AOM and was observed and described for the first time in medical history in the context of major influenza epidemics at the end of the 19th and beginning of the 20th century. 3,4 To this day, the term “Grippeotitis” (“influenza otitis”) is still widely being used in otorhinolaryngology in German-speaking countries and in almost all German-language ENT textbooks, in which the influenza virus is often regarded as the etiological agent for hemorrhagic BM. 5 However, a review of the scientific literature shows that BM, which is present in less than 10% of all cases of AOM, has a pathogen spectrum similar to that of ordinary AOM but with a higher proportion of Streptococcus pneumoniae and Haemophilus influenzae 6 -8 ; clinically, BM is characterized by more severe symptoms compared to ordinary AOM, with a more pronounced bulging of the tympanic membrane and more severe pain. 9
Acute otitis media may be complicated by an inner ear disorder (IED), which primarily affects the basal cochlear turn (localized serous or toxic labyrinthitis) and manifests itself clinically as temporary or permanent sensorineural hearing loss (SNHL). 10 Although observed in practice on a regular basis, it is noteworthy that there are little data in the literature on the incidence of IED due to AOM. A study in Korea found an incidence of 9.6% in 75 patients with AOM, with SNHL occurring within 0 to 10 days of AOM onset and regularly beginning with high-frequency hearing loss. 11 However, the incidence of SNHL in BM has been investigated in several studies, with significantly higher rates of SNHL in up to 67% of cases. 12 -14
The studies on IED in various forms of AOM that have been published to date have all come from hospitals and are, therefore, likely to have a selection bias in favor of more severe cases. Data from ENT practices, which are the first diagnostic gatekeeper in health care for patients with acute ear symptoms, are not yet available. Moreover, since only studies from individual institutions are available, the number of cases in previous studies is relatively low. Thus, the aim of the present study was to determine, with the help of a nationwide and representative practice database: how frequently the various forms of AOM are being diagnosed in ENT practices in Germany; which form of AOM presented the highest risk for an IED; and whether other risk factors for the occurrence of an IED can be identified.
Methods
Data Source
The data source for this retrospective study was IQVIA’s Disease Analyzer database, which contains patient-related diagnostic and therapeutic information from approximately 3000 medical practices in various disciplines. The data are acquired via a standardized interface from the IT systems of the participating practices and checked for plausibility. Subsequently, the available information is linked with relevant additional information such as coding according to International Classification of Diseases, Tenth Edition (ICD-10) and Anatomical Therapeutic Chemical Classification System, as well as drug prices, and is updated monthly. The database contains only anonymized data in accordance with the applicable data protection directives. 15 The database has been used several times for epidemiological studies in the field of otorhinolaryngology. 16 -18
Collected Data
The present study used data from ENT practices in Germany, which continuously provided data from January 2010 to December 2017. Patients who had been coded as having the following AOM diagnoses (ICD-10) during this period were included: “acute serous otitis media” (H65.0), “other acute nonsuppurative otitis media” (H65.1), “nonsuppurative otitis media, unspecified” (H65.9), “acute suppurative otitis media” (H66.0), “suppurative otitis media, unspecified” (H66.4), “otitis media, unspecified” (H66.9), “otitis media in viral diseases classified elsewhere” (H67.1), and “acute myringitis” (H73.0). The date of AOM diagnosis (= index diagnosis) was defined as the index date. From this group, those patients were identified who had received a first diagnosis of an IED within 12 months of the index date (= outcome diagnosis). The following IED diagnoses were included as outcome diagnoses: “labyrinthitis” (H83.0), “disease of inner ear, unspecified” (H83.9), “sensorineural hearing loss, unspecified” (H90.5), “ototoxic hearing loss” (H91.0), and “hearing loss, unspecified” (H91.9). The basic characteristics such as age, sex, and insurance status (statutory vs private health insurance) were recorded for all study patients. In patients with an IED, the diagnosis date of the IED was recorded.
Data Presentation
For each AOM diagnosis, the distribution of all IED diagnoses within 7 days of the index date was presented.
The age and sex distribution of patients with IED diagnoses within 7 days of the index date was shown.
For each AOM diagnosis, the probability of an IED diagnosis was displayed over a period of 12 months from the index date using Kaplan-Meier curves.
The associations between AOM diagnoses and IED diagnoses as well as between IED diagnoses and age, sex, and insurance status were presented as odds ratios (OR). A P value of <.05 was considered significant. Statistical analyses were carried out using SAS Version 9.4 (SAS Institute Inc).
Results
Index Diagnoses
In the period between January 2010 and December 2017, a total of 286 186 patients with various forms of AOM were available in the database (average age 33 ± 24 years, 51.8% female, and 88.8% with statutory health insurance coverage). The most frequent diagnoses were “nonsuppurative otitis media, unspecified” (47.6%) and “otitis media, unspecified” (39.0%), while specific forms of AOM were rare. The distribution of diagnoses is shown in Table 1. The diagnosis “otitis media in viral diseases classified elsewhere” was not found in the database. The original text “Grippeotitis” (“influenza otitis”) was found approximately 3 times per practice per year.
Baseline Characteristics of Study Patients.
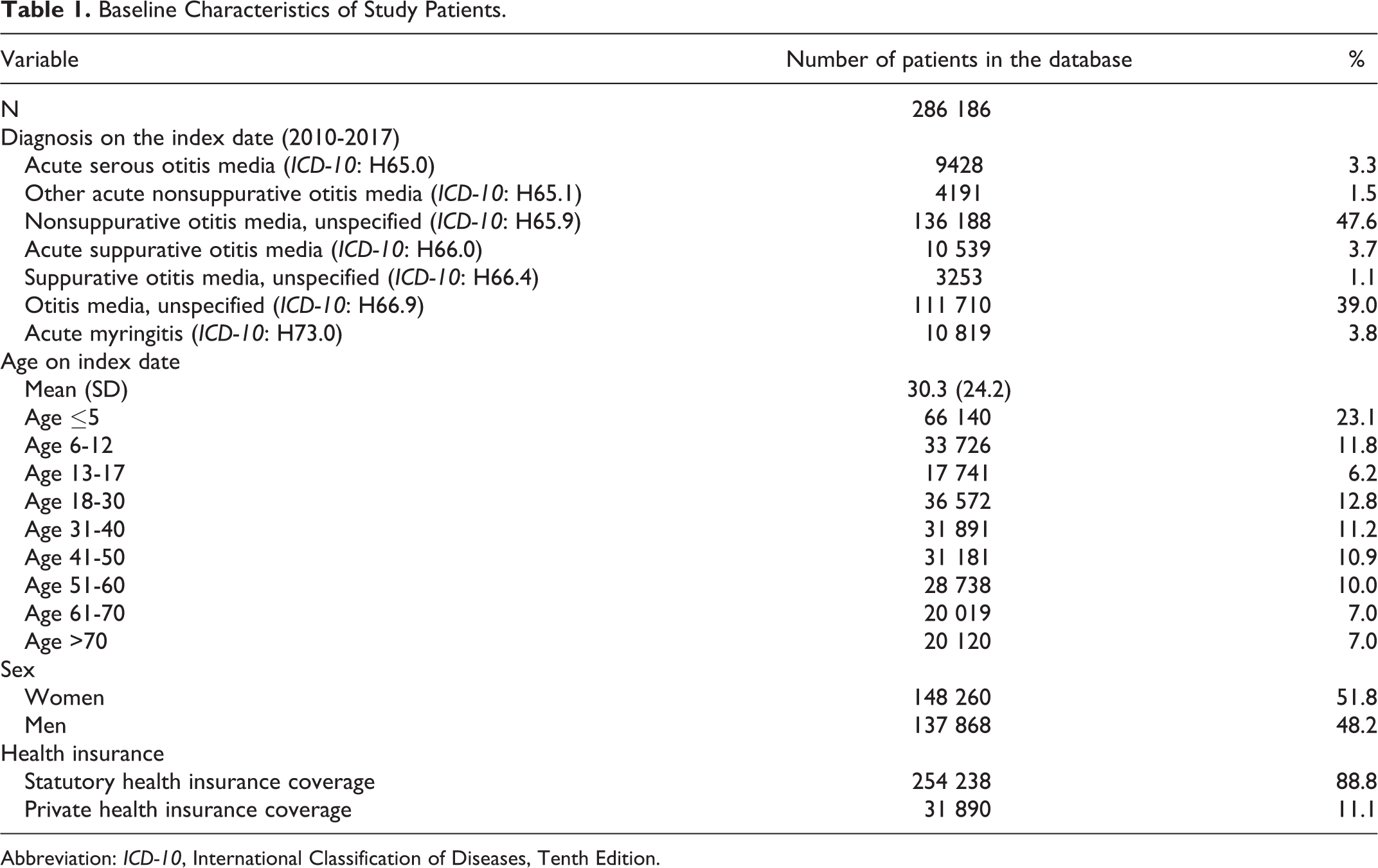
Abbreviation: ICD-10, International Classification of Diseases, Tenth Edition.
Outcome Diagnoses
The most frequent IED diagnoses within 7 days of an AOM diagnosis were “hearing loss, unspecified” and “sensorineural hearing loss, unspecified,” while the diagnoses “labyrinthitis,” “disease of inner ear, unspecified,” and “ototoxic hearing loss” were rare in the database. The percentage distribution of IED diagnoses, stratified by AOM diagnoses, is shown in Figure 1.
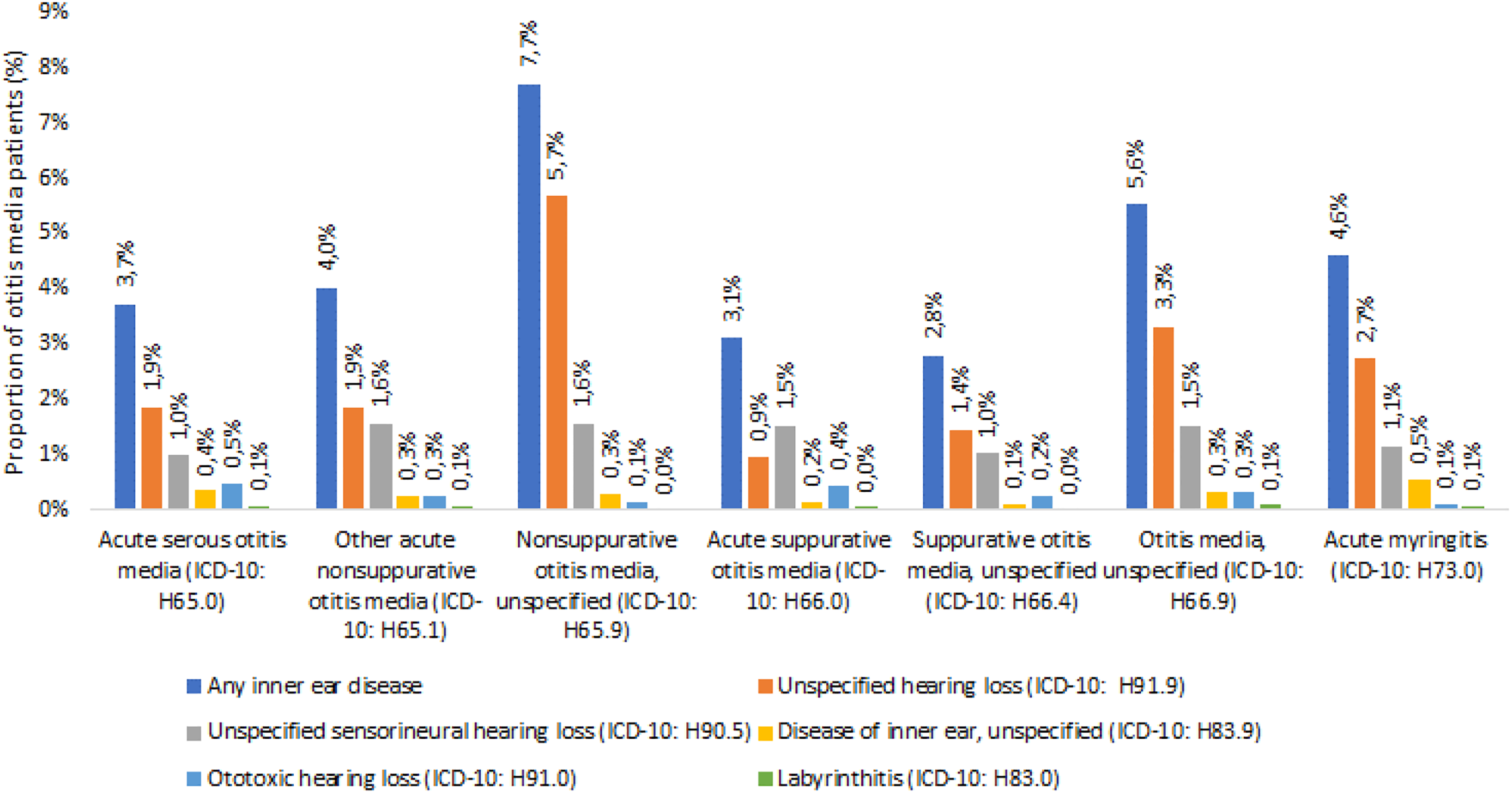
Proportions of patients with inner ear diseases diagnosed within 7 days following an acute otitis media diagnosis, stratified by index diagnosis.
Influence of Age and Sex on Outcome Diagnoses
With increasing age, the incidences of the IEDs “hearing loss, unspecified” and “sensorineural hearing loss, unspecified” increased steadily. The diagnoses “labyrinthitis,” “disease of inner ear, unspecified,” and “ototoxic hearing loss” were not found in children and adolescents, were rare in adult patients from 18 years of age, and did not increase with age. Sex had no influence on the frequency distribution of IED diagnoses (Figure 2).
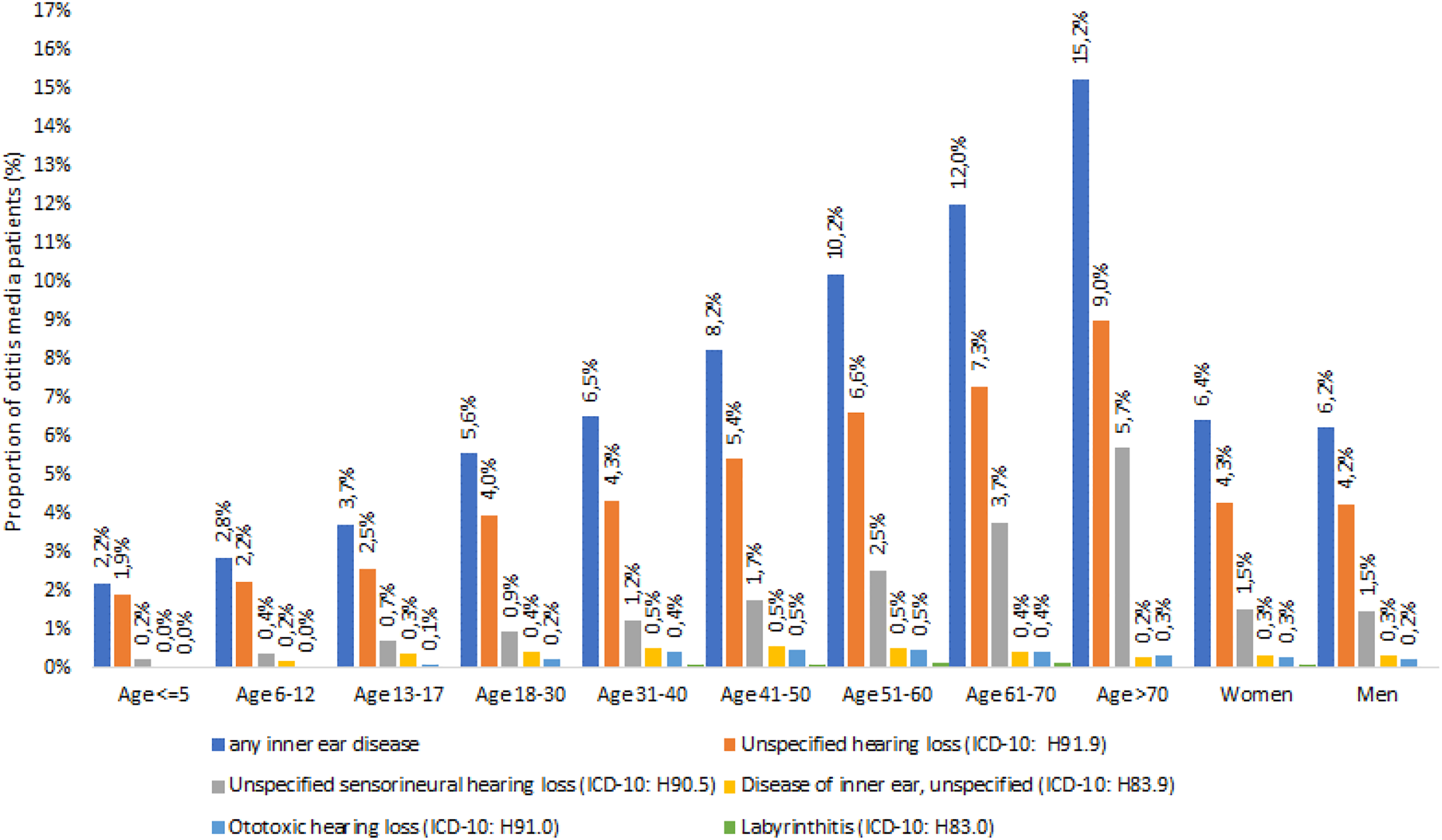
Proportions of patients with inner ear disorders diagnosed within 7 days following an acute otitis media diagnosis, stratified by age and sex.
Associations Between Outcome Diagnoses and Index Diagnoses or Basic Characteristics
Within 7 days of the index date, the highest chance of an IED diagnosis was found for “nonsuppurative otitis media, unspecified” (reference). The other AOM diagnoses all showed a significantly lower risk of an IED diagnosis (odds ratio [OR] between 0.34 and 0.63, each P < .001; Table 2).
Association Between Acute Otitis Media and the Incidence of Inner Ear Disorders Within 7 Days Following Otitis Media Diagnosis.a
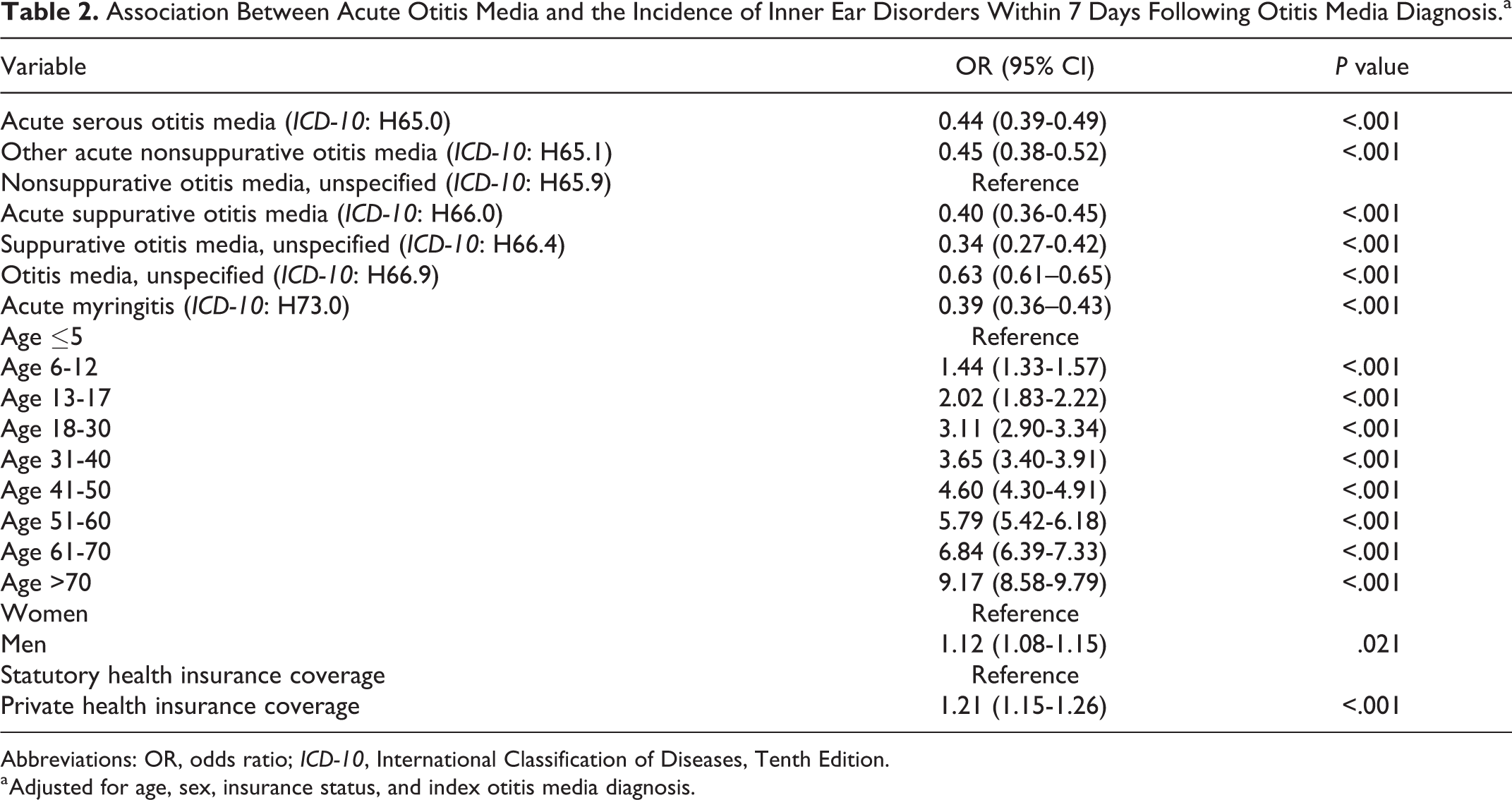
Abbreviations: OR, odds ratio; ICD-10, International Classification of Diseases, Tenth Edition.
a Adjusted for age, sex, insurance status, and index otitis media diagnosis.
Incidences of Outcome Diagnoses Within 12 Months of the Index Date (Kaplan-Meier Curves)
The highest incidence of IED diagnoses was found in patients with “nonsuppurative otitis media, unspecified” (index date: 7.4%; after 7 days: 7.7%; after 12 months: 15.9%). The second highest incidence of IED diagnoses was found in patients with “otitis media unspecified” (H66.9; index date: 4.8%; after 7 days: 5.6%; after 12 months: 13.5%). The remaining index diagnoses had lower incidences of inner ear diagnoses (index date: 2.2%-4.1%; after 7 days: 2.7%-4.9%; after 12 months: 8.8%-11.2%; Figure 3).
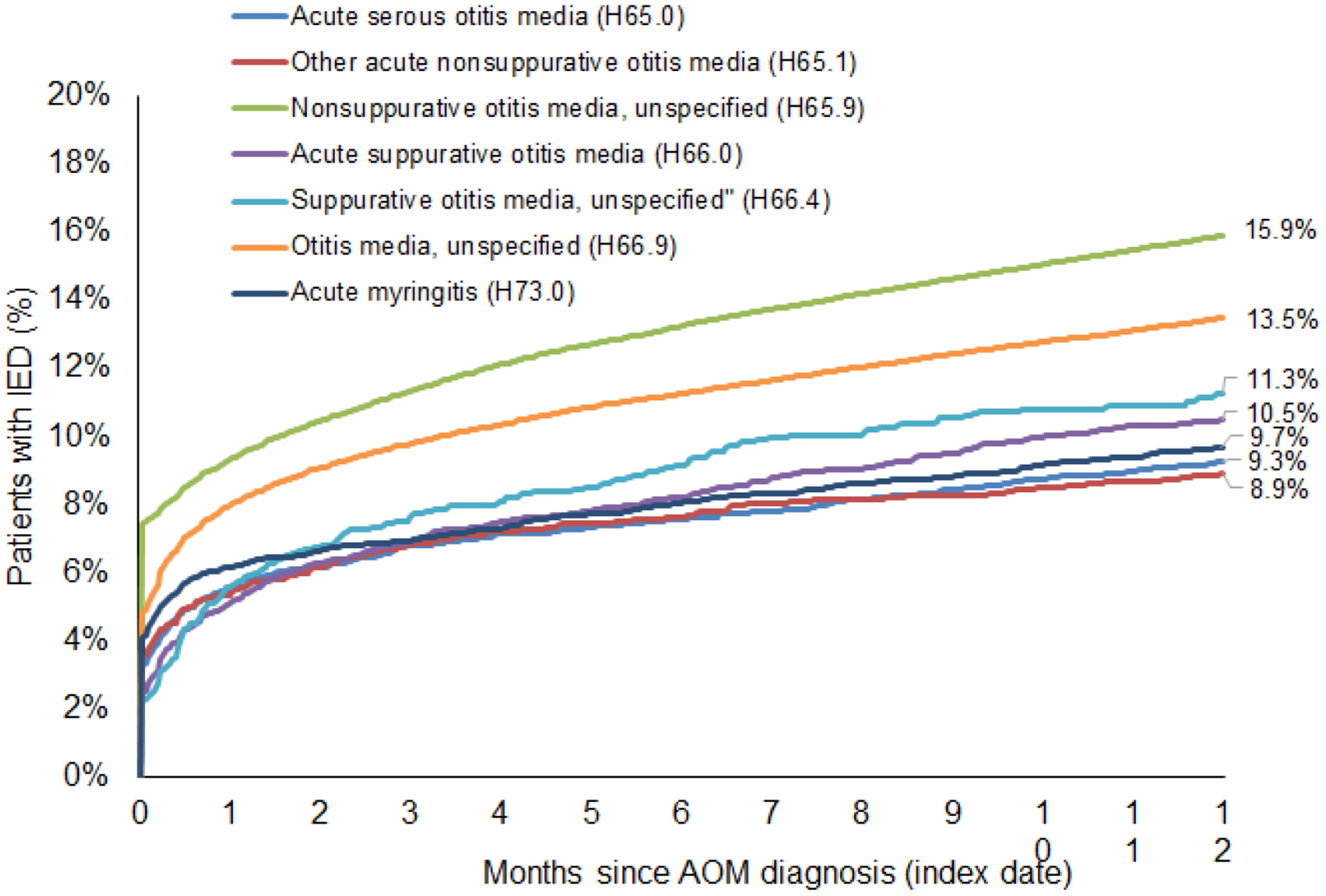
Kaplan-Meier curves for the occurrence of inner ear disorders (IED) after acute otitis media (AOM) diagnoses in ENT practices in Germany.
Discussion
The aim of the present study was to determine the incidences of various forms of AOM in ENT practices in Germany and to determine the incidences of subsequent IED diagnoses in the sense of an inflammatory inner ear involvement. For this purpose, a sample of nearly 290 000 patients from the years 2010 to 2017 was collected from an ICD-10-based nationwide and representative practice database, which included various forms of AOM as index diagnoses and various IED as outcome diagnoses. Problematic for the study design was the fact that there is no single and unambiguous ICD-10 code for inner ear involvement in AOM, but, rather, several specific and nonspecific ICD-10 codes are possible. Several terms for this condition are employed in the medical literature: While some authors call it serous or toxic labyrinthitis (in contrast to suppurative labyrinthitis, which is more severe and usually leads to deafness of the affected ear), 10,19,20 a common medical term in German usage is “toxic inner ear lesion”; 5,21 most authors, however, simply describe the phenomenon unspecifically as SNHL in AOM. 11,22,23 So far, it is not clear which ICD-10 codes are used regularly for inner ear involvement in AOM in ENT practices in Germany or other countries. Thus, for the current study, those ICD-10 codes that appeared possible and probable for the coding of an inflammatory inner ear involvement in AOM, according to the authors’ experience, were selected as outcome diagnoses.
One main result of this study was the fact that in ENT practices in Germany, AOM and IED are predominantly being documented with nonspecific ICD-10 codes. Such a nonspecific and pragmatic habit of clinical coding by physicians has already been found in earlier ICD-10-based database studies on other diagnoses in ENT practices in Germany. 16,24 As a result of this nonspecific coding method, the present study cannot determine clearly which forms of AOM have the highest risk of subsequent IED and which types of IED are specifically diagnosed as a result of AOM. Specific codes such as “labyrinthitis” or “ototoxic hearing loss” were rarely used. It should also be noted that the code “ototoxic hearing loss” could also have been used for the ototoxic effects of drugs (eg, aminoglycosides, cytostatics, diuretics, etc). As a result of this uncertainty, a causal relationship between index and outcome diagnoses cannot be established in the vast majority of cases.
The age distribution of the patients shows that children up to 5 years of age are by far the largest affected group, while patients aged 61 to 70 and over constitute the smallest group. On the other hand, the incidence of IED diagnoses after AOM is lowest in children, while it increases with patient age. The highest number of IED incidences is found in the eldest of the patients; however, this increase in IED diagnoses consists entirely of an increase in nonspecific codes (“hearing loss, unspecified” and “sensorineural hearing loss, unspecified”), while the rare specific diagnoses “labyrinthitis” and “ototoxic hearing loss” are evenly distributed among the age groups of adult patients. This raises the question of whether older patients have a higher risk of inner ear involvement as a result of AOM, which, again, cannot be verified due to the study design. However, it is likely that a large proportion of the IEDs found in older patients are preexisting conditions but with AOM being the occasion for the first diagnosis of this hearing impairment.
The highest risk of an IED at the index date was found in “nonsuppurative otitis media, unspecified.” In the following 2 weeks, an increase of IEDs in “otitis media unspecified” was observed, which then showed the second highest incidence of IED in the further course of the disorder. Assuming that the majority of suppurative AOM were coded here, this is an interesting finding because, to the authors’ knowledge, no studies comparing the inner ear risk and also the latency of an IED between nonsuppurative and suppurative AOM have been available so far. It seems that suppurative AOM may initially have a lower probability of an IED but at the same time a higher latency until the occurrence of an IED. This could be due to the fact that, according to clinical experience, suppurative AOM more frequently leads to perforations of the tympanic membrane, by which toxic agents may be drained from the middle ear, thus preventing further inner ear damage. This protective effect could possibly be reversed after spontaneous closure of the perforation and thus lead to damage of the inner ear with the observed temporal latency. However, which types of AOM were exactly diagnosed under the nonspecific codes H65.9 and H66.9 remains unclear due to the methodological limitations mentioned earlier. A prospective clinical study comparing the inner ear risk and the time course between nonsuppurative and suppurative AOM could provide further insights into this.
Traditionally, in German medical practice, AOM with hemorrhagic blisters on the tympanic membrane is widely referred to as “Grippeotitis” (“influenza otitis”), while the term “bullous myringitis” is not very common in Germany, in the authors’ experience. With the current study design, neither of these diagnoses could be detected properly in ENT practices in Germany. A hemorrhagic BM is seen in less than 10% of all AOM cases 8 but is associated with a high rate of SNHL, which is seen in up to 67% of cases. 12 -14 Obviously, these forms of AOM are almost never documented as a diagnosis in ENT practices in Germany (the original text “Grippeotitis” was found approximately 3 times per practice per year, while the diagnosis “Otitis media in viral diseases classified elsewhere” was not found at all). The diagnosis “acute myringitis,” which could theoretically be used for BM, showed a comparatively low risk of a subsequent IED diagnosis. Thus, in ENT practices in Germany, this code is most likely not being used in connection with AOM but rather in myringitis without AOM. Clinical findings are not included in the database so that further outcome analyses with regard to hemorrhagic BM or influenza otitis are not possible. Here, also, a relevant weakness of the current ICD-10 classification becomes apparent, namely, that a hemorrhagic bullous form of AOM cannot be coded unambiguously. This is relevant, insofar as an exact documentation of this subtype appears to be reasonable from a medical and epidemiological point of view due to the increased morbidity associated with it (high rate of IED).
Interestingly, the phenomenon of IED in AOM has so far mainly been described in animal studies, histopathological and clinical case reports, as well as case series, 10,19,20,25,26 while epidemiological data on the incidence of IED in AOM are scarce. In fact, the authors were able to identify only 1 study that determines the incidence of IED in AOM in a clinical context. In 2014, Park et al 11 retrospectively analyzed the cases of 75 adult patients (83 ears) with AOM from a secondary referral hospital and found an SNHL in 9.6% of cases (8 ears), using rather strict inclusion criteria for SNHL (bone conduction [BC] loss of ≥ 30 dB in ≥ 3 frequencies in comparison with the opposite normal ear). Sensorineural hearing loss was observed early after the onset of AOM (average: 4.6 days) and recovered over an average of 18.6 days. However, the authors did not specify whether the AOM diagnoses were suppurative or nonsuppurative (Table 3). This incidence of SNHL of 9.6% is slightly higher than the incidence of any IED in this present study (at index date: 2.2%-7.4%; after 7 days: 2.7%-7.7%). This could be explained by several reasons: Firstly, in a secondary referral hospital, the average case severity in AOM may be higher than in primary care practices due to case selection. Secondly, audiometry may be performed more frequently in ENT referral hospitals than in ENT practices. Thirdly, in some cases in ENT practices, IED in AOM may be diagnosed and treated correctly, but without being coded, as there exists no specific ICD-10 code for this very common diagnosis, and searching for alternative codes may be laborious and impractical.
Studies on Inner Ear Involvement in Various Forms of Otitis Media.
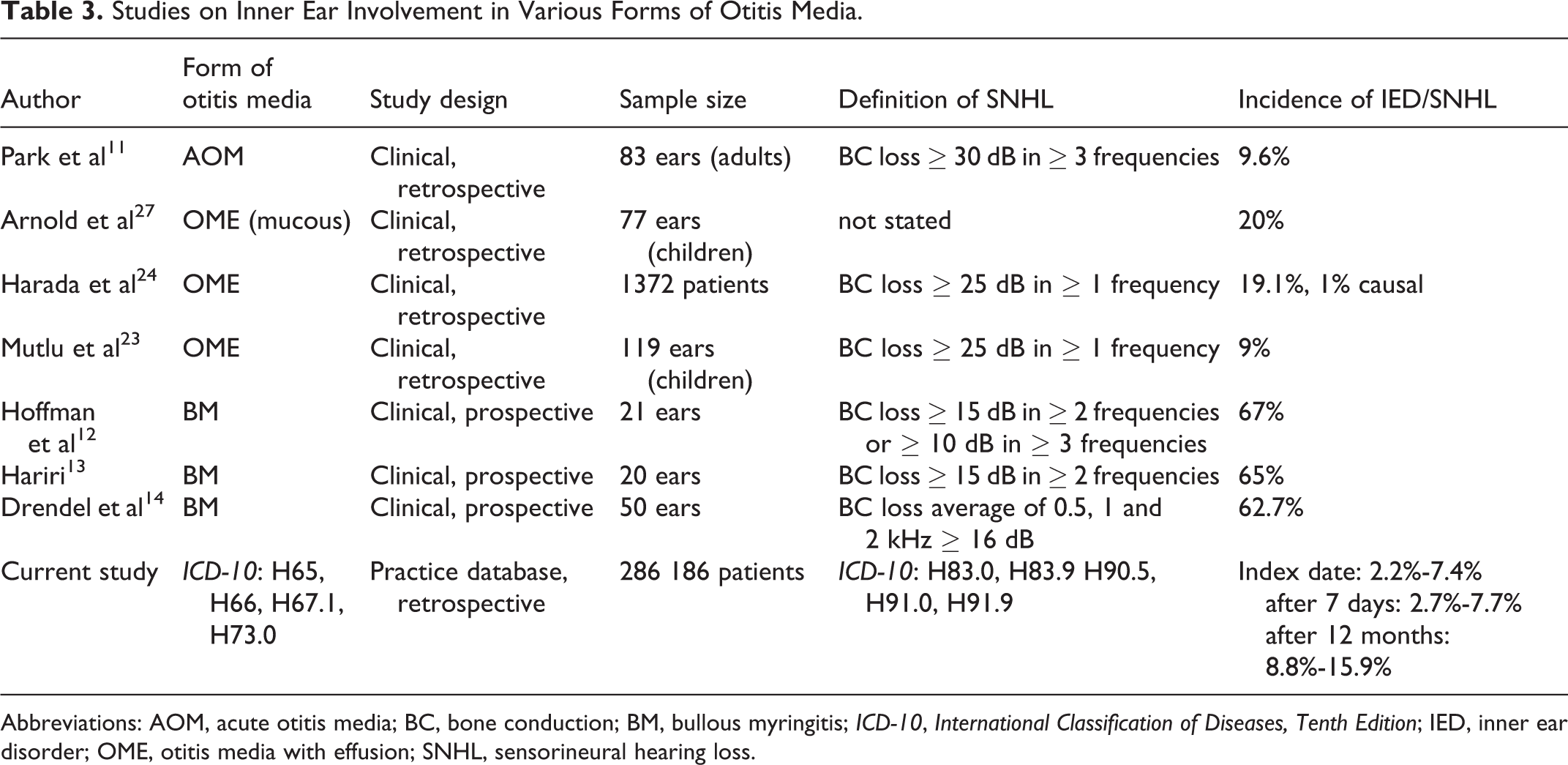
Abbreviations: AOM, acute otitis media; BC, bone conduction; BM, bullous myringitis; ICD-10, International Classification of Diseases, Tenth Edition; IED, inner ear disorder; OME, otitis media with effusion; SNHL, sensorineural hearing loss.
Other studies investigated the incidence of IED in otitis media with effusion (OME). In 1977, Arnold et al 27 found an incidence of SNHL of 20% in children with OME (77 ears, no audiometric inclusion criteria stated). In contrast, in 1992, Harada et al 23 published a retrospective study of 1372 OME cases (children and adults) with 262 (19.1%) cases of SNHL (BC loss ≥ 25 dB in at least 1 frequency). However, the authors considered the SNHL to be etiologically related to OME in only 14 (1%) cases. In 1998, Mutlu et al 22 published a retrospective study of 71 children with OME (119 ears) and found an SNHL (BC loss ≥ 25 dB in at least 1 frequency) in 9% of the cases (Table 3). When comparing the 3 abovementioned studies with the current study, it should be noted that OME includes not only acute but also chronic tympanic effusions, which are coded with H65.2 (“chronic serous otitis media”), H65.3 (“chronic mucoid otitis media”), and H65.4 (“other chronic nonsuppurative otitis media”). However, these codes were not included in the current study, which focused only on acute, not chronic, forms of otitis media. It should also be noted that the inclusion criteria for SNHL were less strict in the work of Harada et al and Mutlu et al (OME) than in the work of Park et al (AOM). Thus, under the assumption of equal audiological inclusion criteria, the incidence of SNHL would most likely be lower in the OME studies or higher in the AOM study.
Among the different forms of AOM, the incidence of IED has been investigated most intensively in BM. In 1983, Hoffman et al 12 analyzed 15 patients (21 ears) with BM prospectively and found an SNHL (BC loss ≥ 15 dB in ≥ 2 frequencies or ≥ 10 dB in ≥ 3 frequencies) in 67% of the cases. In 1990, Hariri 13 examined 18 patients (20 ears) with BM prospectively and found an SNHL (BC loss ≥ 15 dB in ≥ 2 adjacent frequencies) in 65% of the cases. In 2012, Drendel et al 14 found an SNHL in 63% of BM cases in 43 patients (50 ears) in a prospective study (Table 3). According to these data, the incidence of IED in BM appears to be substantially higher than in AOM or OME, but this fact could not be demonstrated in the present ICD-10-based database study due to the limited diagnostic precision of the ICD-10 system discussed above.
Limitations and Strengths of the Study
The present study is subject to various limitations. First, the study is only based on ICD-10 codes, as the practice database does not contain any clinical information. The correctness of the diagnostic coding in general and the severity of hearing loss in particular could therefore not be determined. Although this is considered a main limitation if this study, ICD-10 is the international standard diagnostic classification what permits the systematic recording, and interpretation of diagnosis data collected in different countries, in different languages, and at different times. In the past, several studies based on the Disease Analyzer database, using ICD-10 codes were published. 16,17,27,28
Second, most diagnoses in the ENT practices had been coded in an unspecific way, which limited the accuracy of data acquisition for this study. Therefore, differences in IED incidences between certain subdiagnoses (eg, serous vs mucous AOM) were possibly not detected. Third, there is no single ICD-10 code for inflammatory inner ear involvement in AOM, so that the outcome diagnoses were mostly unspecific and ambiguous. Fourth, there is no separate code for AOM with BM so that this highly relevant form of AOM could not be analyzed with regard to IED. Fifth, due to the study design only associations, but no causal relationships, could be established between AOM and IED.
A strength of the study is the use of routine data from medical practices in which diagnoses are continuously documented (no recall bias). A major strength of the study is the first-time investigation of the incidence of IED in AOM with the help of a nationwide and representative practice database and a high number of cases. Moreover, the different incidences and latencies of IED in nonsuppurative versus suppurative AOM were described for the first time.
Conclusion
In ENT practices in Germany, various forms of AOM, as well as simultaneous or subsequent IED, are predominantly coded in an unspecific way. Hemorrhagic BM (the so-called “influenza otitis” in Germany), although being regularly observed, is very rarely diagnosed and coded in ENT practices. Moreover, the current ICD-10 system fails to sufficiently record the clinically relevant entities of hemorrhagic BM in AOM as well as inflammatory IED in AOM. Possibly, older patients have a higher risk of IED in AOM, but more likely, AOM is a regular occasion for the initial diagnosis of preexisting hearing impairment in older patients. The highest risk of IED was observed in nonsuppurative AOM, followed by suppurative AOM. The latency until the occurrence of IED was markedly higher in suppurative AOM. Most likely, SNHL in children is underdiagnosed in ENT practices in Germany.
Footnotes
Authors’ Note
Under certain conditions, German law permits the use of anonymized electronic medical data for research purposes. According to this legislation, this type of observational study without identifiable patient data does not require informed consent or an ethics committee vote. The authors did not have access to identifying patient data at any time before, during, or after the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.