
Abstract
Objective:
Our objective was to perform a meta-analysis to compare the effectiveness of steroids and diuretics in the treatment of acute low-tone sensorineural hearing loss (ALHL).
Methods:
PubMed, Google Scholar, and Sci databases were searched for randomized controlled trials (RCTs) examining the treatment of ALHL with steroids and diuretics. The Cochrane Reviewer’s Handbook 5.0 evaluation criteria were used to evaluate the quality of the included RCTs. Meta-analysis was performed using Revman 5.3 software to compare the recovery rate of low-tone hearing levels between patients treated with steroids and diuretics.
Results:
A total of 3 RCTs were included. There was no heterogeneity between the 3 studies (χ2 = 2.61, P = .27, I2 = 23%); thus, a fixed-effects model of analysis was used. Meta-analysis showed there was no significant difference in the recovery rate of patients treated with steroids and those treated with diuretics (odds ratio = 1.48, 95% confidence interval: 0.64-3.40, P = .36).
Conclusion:
Steroids and diuretics are equally effective for the treatment of ALHL.
Introduction
Acute low-tone sensorineural hearing loss (ALHL) is a clinically common disease. Acute low-tone sensorineural hearing loss patients have tinnitus, ear fullness, a slight sense of dizziness, and low-tone hearing loss. The diagnostic criteria for ALHL are not yet clear. Most scholars currently refer to the diagnostic criteria from the Japan Foundation’s Acute Profound Deafness Research Committee of the Ministry of Health, Labor and Welfare: (1) patient attendance at department within 7 days of symptom onset; (2) hearing loss is purely sensorineural and has normal tympanic membrane performance, and a radiological examination of temporal bone and brain ruling out possible organic causes; (3) pure tone audiometry: The sum of hearing loss is 70 dB or higher at 3 low frequencies (125, 250, and 500 Hz), and the sum of hearing loss is 60 dB or less at 3 high frequencies (2, 4, and 8 kHz). In the past, ALHL was considered to be an idiopathic sudden sensorineural hearing loss (SNHL). However, in 1982, Abe 1 for the first time described ALHL as an independent disease. Endolymphatic hydrops 2 -5 and an autoimmune response 6 are considered to be possible causes of ALHL. In addition, more than half of ALHL patients’ hearing is automatically recovered without treatment. However, for all that, there are still some patients who develop symptoms of deafness or progress to the possibility of progression to Ménière disease. Therefore, patients with ALHL should be actively treated rather than managed conservatively, not just waiting for natural recovery. In view of the lack of systematic reviews related to the treatment of ALHL, the purpose of this study was to conduct a meta-analysis of the current literature to compare the effectiveness of steroids and diuretics for the treatment of ALHL.
Methods
Search Strategy
PubMed, Google Scholar, Embase, and Sci databases were searched for randomized controlled trials (RCTs) examining the treatment of ALHL with steroids and diuretics. The search terms were “acute low-tone hearing loss,” “acute low frequency hearing loss,” “low frequency sensorineural hearing loss,” “low-tone hearing loss,” “therapy,” “treatment,” and “RCT.” And the year of the search was from 1990 to 2017.
Inclusion and Exclusion Criteria
The inclusion criteria were RCTs comparing steroids versus diuretics for the treatment of ALHL. The diagnosis of ALHL was required to conform to ALHL diagnostic criteria. Patient age, sex, ethnicity, and time of illness were not restricted and were required to be the same between the steroid treatment group and the diuretic treatment group. The primary outcome measure was the recovery rate of low-frequency hearing after treatment. Studies were excluded if the data of interest were incomplete and if the relevant outcome indicator was not provided.
Quality Assessment
Quality assessment of studies was performed by 2 trained persons. Disputes were resolved by discussion with a third person. The Cochrane Reviewer’s Handbook 5.0 evaluation criteria were used to evaluate the quality of the included RCTs. Evaluation measures were (1) random sequence generation (selection bias), (2) allocation concealment (selection bias), (3) blinding of participants and personnel (performance bias), (4) blinding of outcome assessment (detection bias), (5) incomplete outcome data (attrition bias), (6) other bias. Each measure was classified as “yes,” “unclear,” and “no.” “Yes” represents low risk of bias, “unclear” means that the risk of bias is uncertain, and “no” represents high risk of bias.
Data Extraction
Data extraction was performed using predesigned forms independently by the 2 persons who did the quality assessment. Data extracted included the name of the first author, year of publication, article title, patient characteristics, interventions, disease course, and final outcome.
Data Analysis
Data were analyzed with RevMan 5.3 software. Evaluation of heterogeneity between included studies was done using the I2 test. When the value of P was ≥.1 and I2 was ≤50%, there was no statistically significant heterogeneity between studies, and a fixed-effects model of analysis was used. A value of P < 0.1 and I2 > 50% was considered to indicate statistically significant heterogeneity between studies, and a random-effects model of analysis was used, or sources of heterogeneity were analyzed, and subgroup analysis based on heterogeneity sources was performed. As recovery rate is a noncontinuous variable, treatment efficacy was expressed as odds ratio (OR). Interval estimates were expressed using a 95% confidence interval (CI). A value of P < .05 was considered to indicate statistical significance.
Result
Literature Search
Twenty-five articles were identified in the database searches and were screened based on the inclusion and exclusion criteria. Finally, 3 RCTs meeting the criteria were included in the analysis. 6 -8 None of the included studies were performed in China. The 3 studies included a total of 123 patients; 74 patients were treated with steroids and 49 were treated with diuretics. A flow diagram of the literature screening is shown in Figure 1, and general information of the included studies is shown in Table 1.
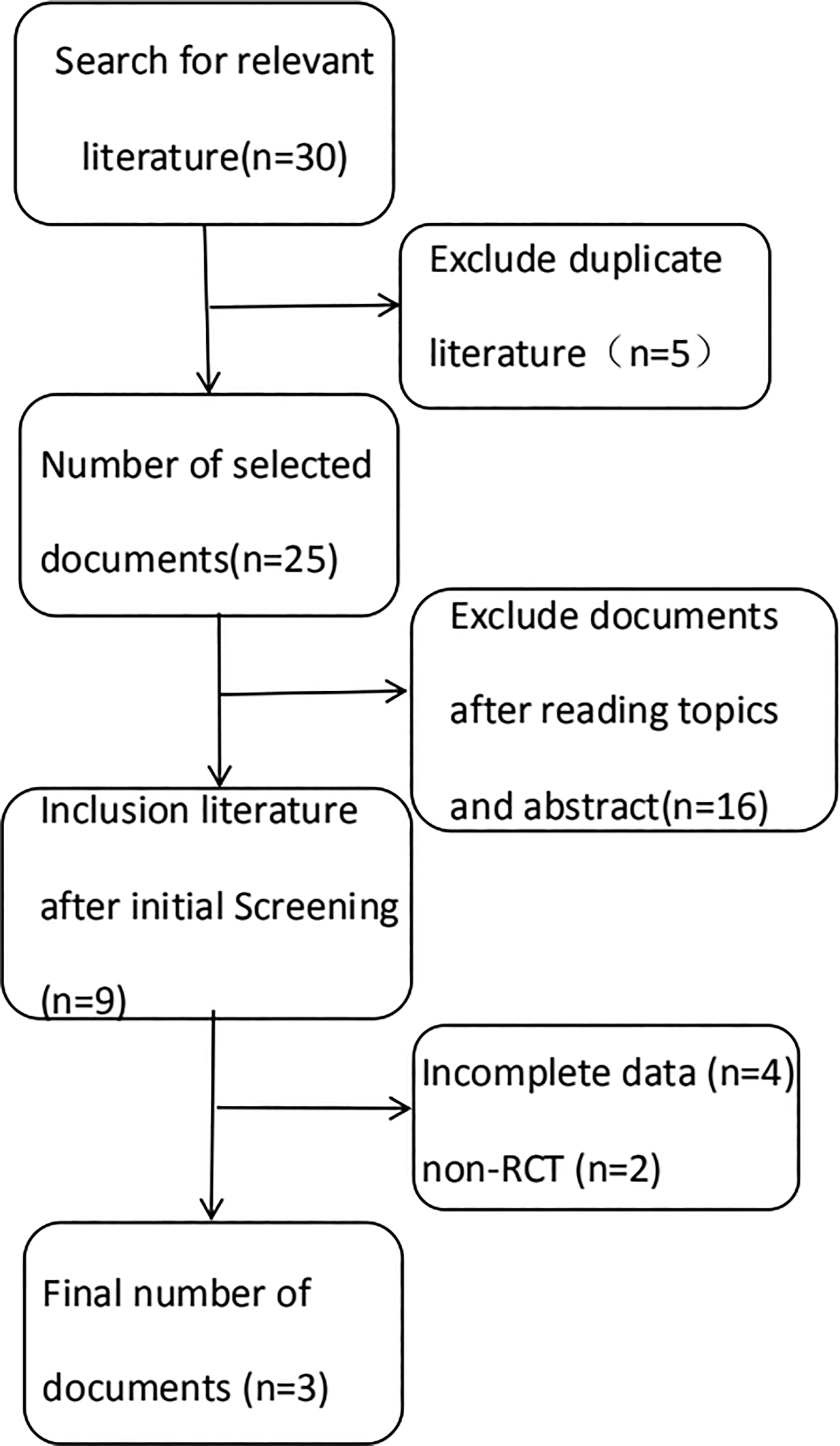
Flow diagram of literature search.
Basic Characteristics of the Included Studies.
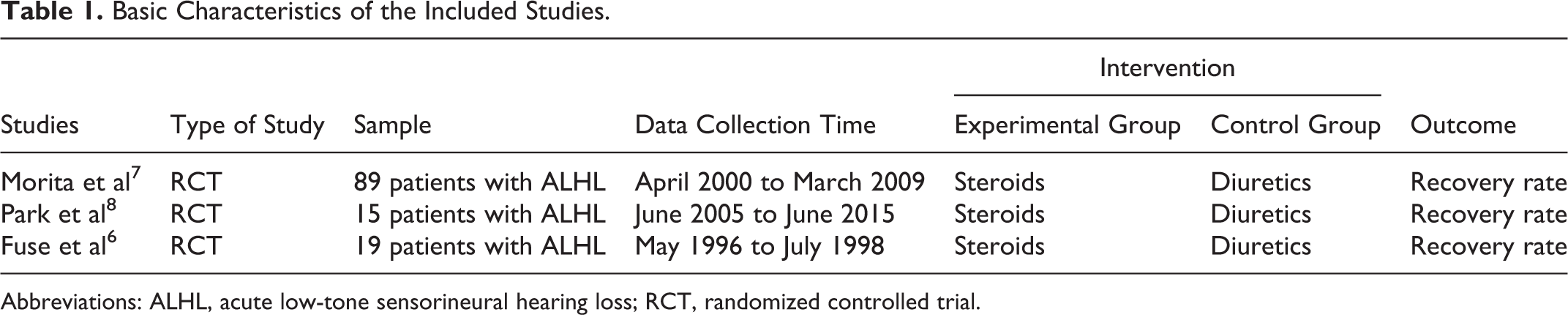
Abbreviations: ALHL, acute low-tone sensorineural hearing loss; RCT, randomized controlled trial.
Quality Assessment
All studies mentioned “randomized research.” However, none of the studies described the randomization method, the allocation concealment method, or the blinding method. All of the studies provided outcome data of interest. Quality assessment results are summarized in Figure 2.
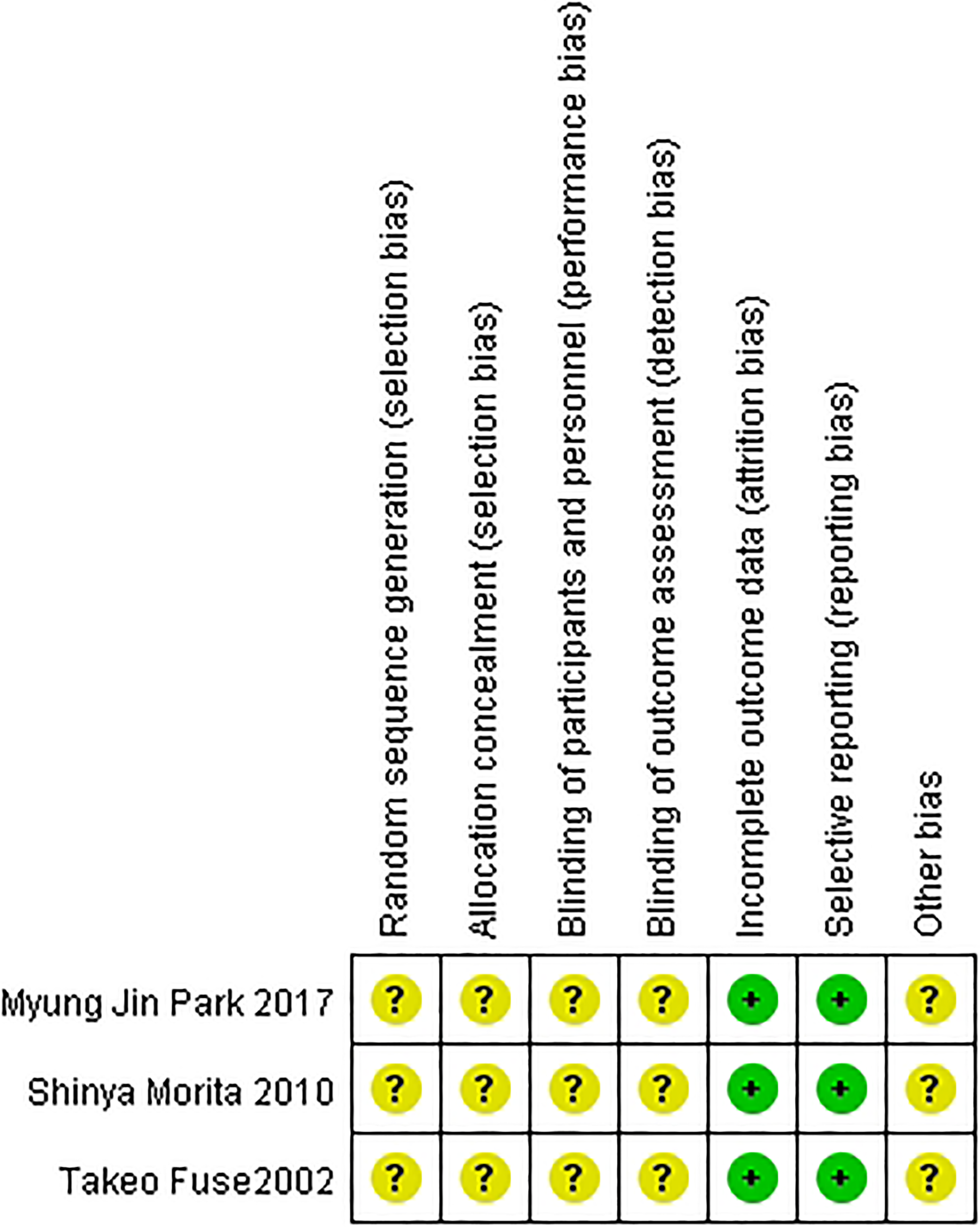
Quality assessment of the included studies. Quality assessment of the included studies according to Cochrane Reviewer’s Handbook 5.0. Two of the evaluations were low risk, and the risks of 6 evaluations are unknown. The overall quality of the included studies is not high.
Meta-Analysis
There was no heterogeneity between the 3 studies (χ2 = 2.61, P = .27, I2 = 23%); thus, a fixed-effects model of analysis was used. Results of the meta-analysis showed there was no significant difference in the recovery rate of patients treated with steroids and those treated with diuretics (OR = 1.48, 95% CI: 0.64, 3.40, P = .36; Figure 3).
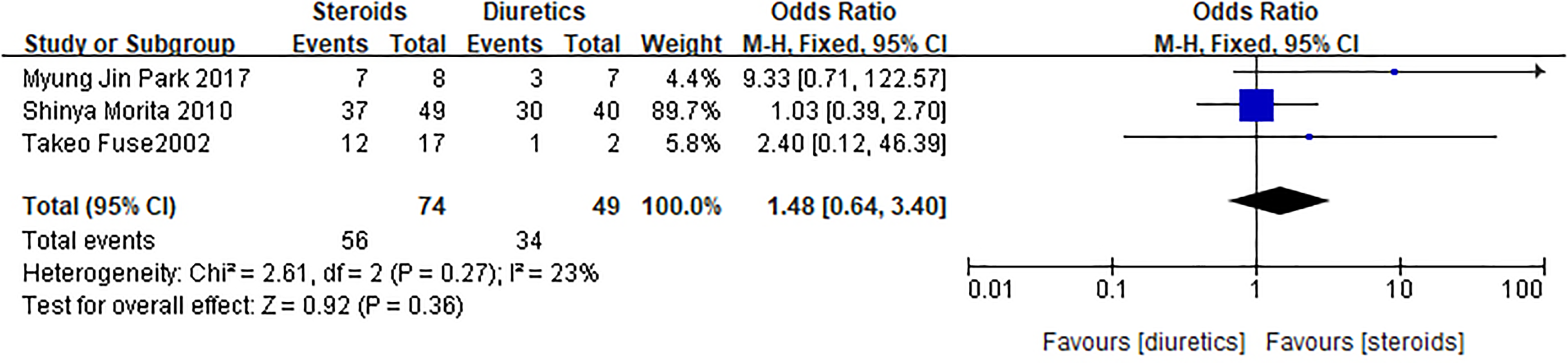
Meta-analysis of low-frequency hearing recovery rate. There was no heterogeneity between the 3 studies (χ2 = 2.61, P = .27, I2 = 23%); thus, a fixed-effects model of analysis was used. Meta-analysis showed there was no significant difference in the recovery rate of patients treated with steroids and those treated with diuretics (odds ratio = 1.48, 95% confidence interval: 0.64-3.40, P = .36).
Discussion
In 1994, Yamasoba et al 4 reported that 63% of patients with ALHL had an increase in summating potential/compound action potential ratio of electrocochleogram (ECochG), and 74% had a positive glycerol test (74%). Studies 4,9 have found that in the endolymphatic hydrops and Ménière disease, glycerol test and ECochG results are similar to ALHL results. At the same time, Im et al 10 found that the greater the low-tone hearing loss, the higher the ECochG value (the severity of endolymphatic hydrops). The authors concluded that ALHL is caused by endolymphatic hydrops. With ALHL, the more severe the low-frequency hearing loss, the better the hearing recovery, which is different than recovery after SNHL. In addition, the autoimmune response is also considered to be one of the causes of ALHL. McCabe 11 recognizes that patients with sensorineural hearing loss have an autoimmune response based on diagnostic studies and patient response to immunosuppressant agents such as cortisone. A study 12 has shown that although ALHL patients do not have vertigo, it is not uncommon to have abnormal vestibular function. The water caloric test suggests that some patients with early-stage ALHL have different degrees of vestibular dysfunction. Acute low-tone sensorineural hearing loss not only involves the top of the cochlear but can be complicated with vestibular dysfunction, which may be a cause of progression to Ménière disease. As such, treatment of ALHL is important.
Various treatments have been used to treat ALHL. One study reported that low salt and low solute diets have a positive effect on ALHL patients. 10 Drug therapy is considered to be the most effective way to treat ALHL, and the most widely used drugs are steroids and diuretics. The degree of low-frequency hearing level changes in patients with ALHL after treatment is classified into 5 grades: (1) complete recovery, defined as a hearing threshold reduced to ≤20 dB, which is within normal range, at all frequencies below 500 Hz; (2) partial recovery, defined as an improvement in hearing threshold at low frequencies by 10 dB or more compared to the initial hearing threshold; (3) progression, defined as an increase in the low-frequency hearing threshold of more than 10 dB compared to the initial hearing threshold; (4) fluctuation, defined as an average loss of 30 dB or more at low frequencies seen after “complete recovery” or “partial recovery”; (5) unchanged, defined as a <10 dB difference in hearing thresholds from before to after treatment. These outcome criteria are based on the model of the Study Group for Acute Profound Deafness Research Committee of the Ministry of Health, Labor and Welfare of Japan. Clinically, the ratio of the number of “complete recovery” and “partial recovery” to the total number of patients is often defined as the recovery rate of low-frequency hearing level after treatment. On the contrary, “progression,” “fluctuation,” and “unchanged” refer to no improvement in low-frequency hearing level after treatment. The results of this meta-analysis found that there was no statistical difference in the recovery rate of low-frequency hearing levels between patients treated with steroids and those treated with diuretics. There are 2 possible reasons for the results. The number of studies included was small, and the treatment effect is not high. The effectiveness of the 2 treatments is similar, suggesting that both steroids and diuretics can significantly reduce endolymphatic hydrops. The efficacy of the above 2 drugs on ALHL is affected by the interval between the onset of symptoms and the start of treatment. The longer the interval, the lower the recovery rate of hearing. According to an earlier report, 13 when the patient started treatment within 7 days after the onset of ALHL symptoms, the hearing recovery rate increased significantly.
Regarding the relationship between ALHL and Ménière disease, some scholars 6 believe that ALHL and Ménière disease are different stages of the same immune inner ear disease, ALHL is early and Ménière disease is advanced. Because endolymphatic hydrops is restricted to the cochlea, patients in the initial state do not experience dizziness. However, as the cochlear hydrops progresses to the vestibular organs, patients with endolymphatic hydrops may experience dizziness, and ALHL progresses to Ménière disease. 4,14,15 Jinkyung et al 14 found that ALHL patients with vertigo had a higher possibility of developing Ménière disease (40%) than those without vertigo (12%). At present, the relationship between ALHL and Ménière disease is not fully understood, and relevant research is still needed in the future. In the study we included, only one study mentioned that the subject was a bilateral ALHL and the remainder was unilateral ALHL. Most of the current clinical cases are unilateral ALHL, and very few cases are bilateral, repetitive ALHL. Studies have found that females with ALHL are much higher than males, and unilateral ALHL female patients unaffected ears low-frequency hearing loss is greater than high-frequency hearing loss. Even if it is determined that the contralateral ear is a healthy ear, the low-frequency hearing is slightly damaged compared to the high frequency. The issue of bilateral ALHL, unilateral ALHL, and repetitive ALHL deserves further discussion.
Meta-analysis holds an important place in the field of evidence-based medicine. Although its advantages are obvious, there are still some limitations. An excellent meta-analysis incorporates homogeneous, high-quality studies. Generally, statistically significant results are more easily accepted for publication, and positive results are easier to publish than negative results. Because the drawing of a funnel plot requires a minimum of 5 studies, we were unable to perform a funnel plot analysis. With respect to homogeneity, the 3 trials included in this study exhibited good homogeneity and were suitable for combined analysis. The number of studies and the number of patients in this meta-analysis were small, so there are shortcomings in the strength of argumentation. In the future, large sample size, well-designed, multicenter RCTs are needed to arrive at a more reliable conclusions to guide clinical practice and provide evidence supporting treatment options for ALHL patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the National Natural Science Fund of China (81200748), the Natural Science Fund of Guangdong Province (2018A030313112), and the Science Plan Fund of Guangzhou (201803010033).