
Abstract
Introduction
The most common presentation of tuberculosis (TB) in the ears, nose, and throat (ENT) region is in the cervical lymph nodes, while extra nodal ENT presentation represents less than 1% of all TB sites. 1 Laryngitis and otitis media remain the most frequent ENT diseases of tuberculous origin, 2 whereas nasopharyngeal TB is rare, even in areas endemic for tuberculosis.3,4
Concomitant nasopharyngeal and otomastoid TB is an extremely rare condition, especially in those with accurate evidence of culture or polymerase chain reaction (PCR). To the best of our knowledge, there have only been 2 such cases reported in English literature.5,6 Another 2 such cases have been reported in Chinese literature.7,8 We have encountered 3 such patients (from 2 tertiary medical institutions), whose treatment had led to satisfactory outcomes. Hence, we want to report these cases, and a summary of all 7 cases with this particular condition is also presented.
Patients and Methods
A retrospective review of cases with concomitant nasopharyngeal and otomastoid TB treated at 2 tertiary medical institutions between June 2022 and May 2024 was undertaken. The clinical and demographic data were retrieved from case records. The protocol of the research project was approved by the institutional review board, and it conformed to the provisions of the Declaration of Helsinki. Written consent forms were obtained from the patients.
Strategy of Management
When patients present with various symptoms, including ear fullness, otorrhea, hearing loss, facial paralysis, and otalgia, careful diagnostic workup should be performed: physical examination could reveal ear canal skin to be swollen and tympanic membrane might not be seen; pure tone average of air conduction could be obviously reduced (68.33 dB HL for Case 3, see Figure 1A), while bone conduction was generally slightly reduced. Temporal computed tomography (CT) scan could show soft tissue inside the tympanic and mastoid cavity with multiple bony erosion, possibly involving the facial nerve canal (Figure 1B); while temporal MRI could reveal involvement of nasopharyngeal area beneath mucosa (Figure 1C). The fiberoptic nasolaryngoscope showed a bulging lesion on the posterosuperior nasopharynx (Figure 1D). For Case 3, the erythrocyte sedimentation rate was 22 mm/hour, and the purified protein derivative assay and interferon-gamma release assay both came back positive.
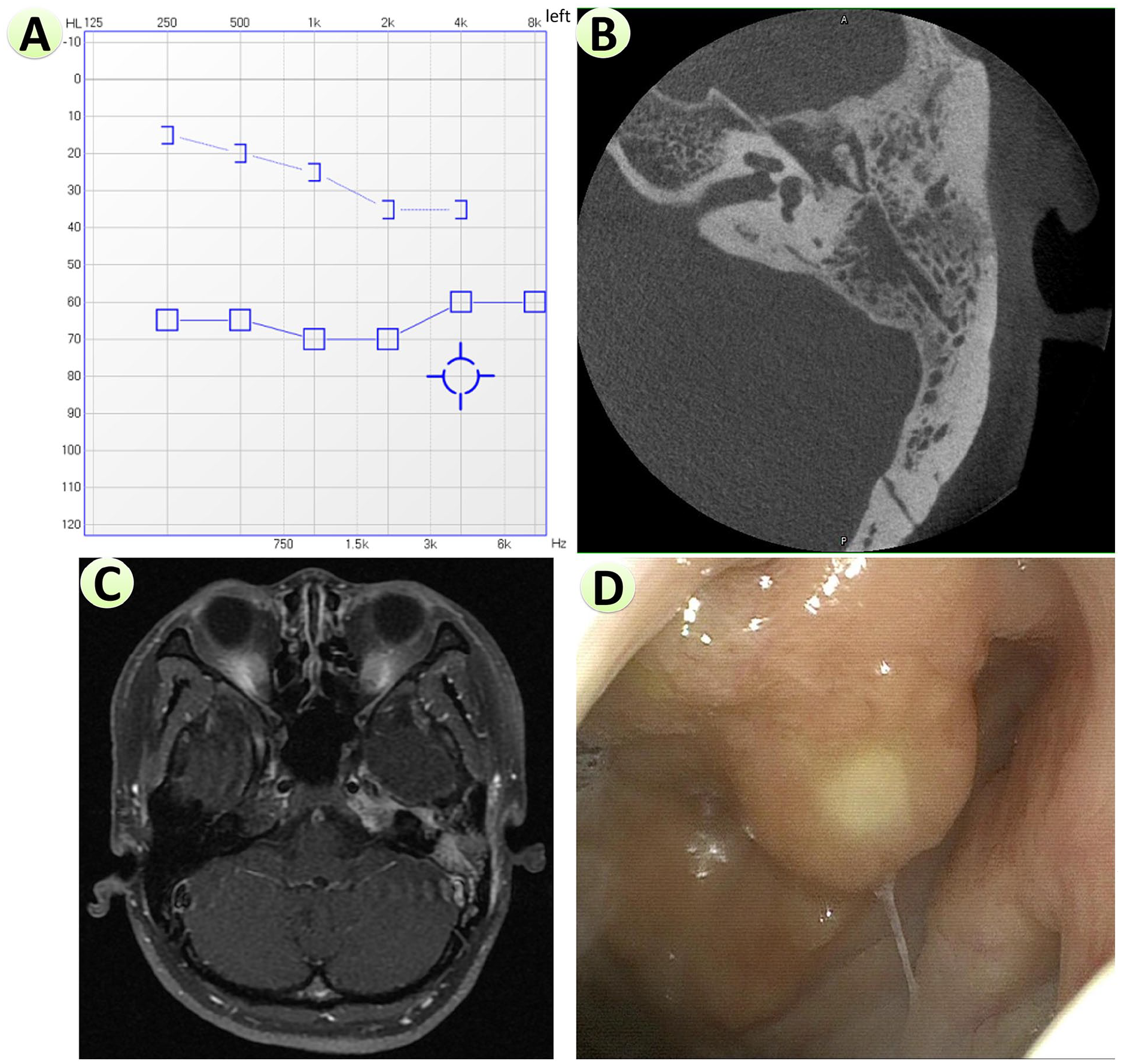
Preoperative examinations for Case 3. (A) Pure tone audiometry, showing moderate-severely decreased air conduction of left ear. (B) A temporal CT scan showed soft tissue inside the left tympanic and mastoid cavities with multiple bony erosion, possibly involving the facial nerve canal. (C) A temporal MRI scan revealed the involvement of the left nasopharyngeal area beneath the mucosa. (D) The fiberoptic nasolaryngoscope showed a bulging lesion on the posterosuperior nasopharynx.
After informed consent, mastoidectomy and/or tympanoplasty could be performed to relieve symptoms, and to acquire biopsy of otomastoid lesion; while in the same operative setting, biopsy of nasopharyngeal lesions could be performed. On the final pathologic report, chronic granulomatous inflammation with small foci of necrosis, caseous necrosis, or granuloma could be observed. Acid-fast bacilli (AFB) staining could be positive, and PCR could confirm the presence of Mycobacterium tuberculosis (Mtb). Symptoms usually improved after surgery, and patients would be referred to TB specialists, to start a full 6 months of standard anti-TB medication. 9
Follow-Up
Patients were routinely followed up every month in the outpatient clinic to observe the outcome of preoperative symptoms, especially the dynamic changes of tympanic condition. When symptoms were relieved, they were followed up every 3 months.
Results
In total, 3 cases were included (2 male patients were from the former institution, and 1 female patient was from the latter). One case was bilateral, and the other 2 cases were unilateral. Their age was between 23 years old and 49 years old (average and median age was 36.3 and 37 years old, respectively). Presenting symptoms included ear fullness, hearing loss, otorrhea, facial paralysis, and otalgia, as shown in Table 1. The pure tone average of the left ear of Case 1 was 50.0 dB HL for air conduction, and 9.2 dB HL for bone conduction; while that of Case 2 was 65 dB HL (left ear) and 92.5 dB HL (right ear) for air conduction, and 32.5 dB HL (both ears) for bone conduction.
Clinical Characteristics of Our Patient and Patients Reported by Literature (The First 2 Patients Were Male, While All Others Were Female).
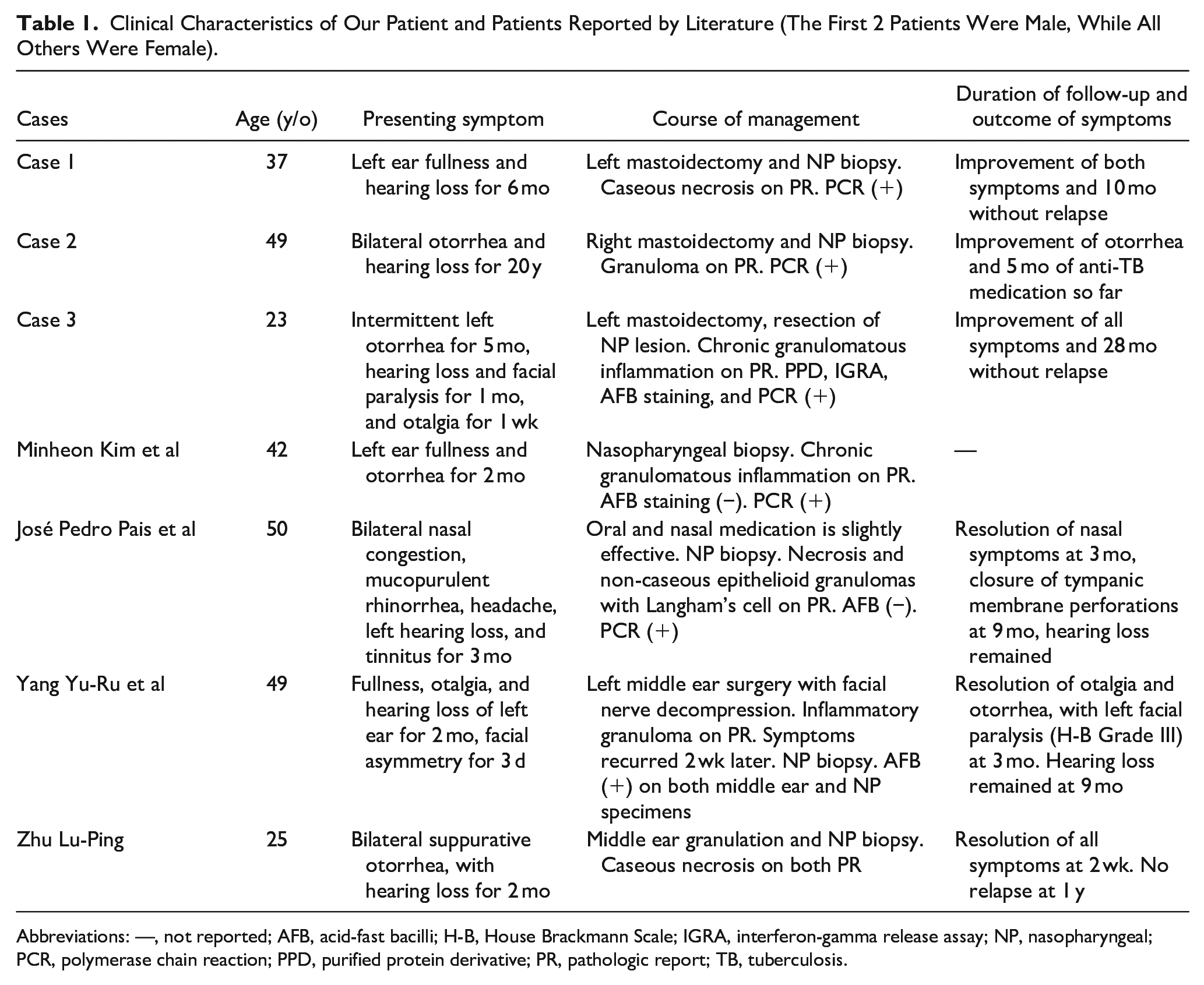
Abbreviations: —, not reported; AFB, acid-fast bacilli; H-B, House Brackmann Scale; IGRA, interferon-gamma release assay; NP, nasopharyngeal; PCR, polymerase chain reaction; PPD, purified protein derivative; PR, pathologic report; TB, tuberculosis.
Careful diagnostic work-up led to the discovery of both otomastoid and nasopharyngeal lesions in all patients. Surgical procedures were planned to relieve symptoms including hearing loss, otorrhea, facial paralysis, and otalgia, and to acquire the biopsy of the nasopharynx. During surgery, most of the middle ear lesions could be found to be soft granulation tissue (possibly involving the Eustachian tube), and the intraoperative frozen section could reveal chronic granulomatous inflammation.
Histopathological examination of lesions of both sites of all cases was suggestive of TB, while PCR examination of lesions of both sites confirmed the presence of Mtb. All patients were subjected to 6 months of anti-TB treatment (rifampicin, isoniazid, pyrazinamide, and ethambutol for 2 months, followed by rifampicin and isoniazid for another 4 months), which will reduce the number of relapses and failures.
After the above treatment, both ear fullness and hearing loss improved for Case 1 (a 37-year-old male patient); for Case 2 (a 49-year-old male patient), otorrhea stopped completely, but the hearing loss did not improve; and for Case 3 (a 23-year-old female patient), all symptoms improved, and she was satisfactory with her current condition, although hearing loss did not completely recover (slightly worse than her healthy ear).
The average and median duration of follow-up was 14.3 and 10 months, respectively. No recurrence was documented.
Discussion
Although otologic discomforts (ear fullness, hearing impairment, and otitis media) are common in nasopharyngeal TB, 3 the diagnosis of otomastoid TB needs confirmation by additional tests, including positive AFB staining of otorrhea (strongly suggestive), PCR, or culture of Mtb from the local discharge or a biopsy sample, and histopathological finds. 2 Hence, the case reported by Pais et al might not necessarily be concomitant nasopharyngeal and otomastoid TB, albeit highly possible, for lack of examinations on otorrhea samples. If this case was excluded from our discussion, then all 6 cases of concomitant nasopharyngeal and otomastoid TB presented with otologic symptoms initially, which might respond to routine antibiotic medications, but symptoms relapsed and progressed. In these scenarios, the nasopharynx should be examined. Should a nasopharyngeal lesion be found, a biopsy of both nasopharyngeal and middle ear lesions should be performed, to distinguish between an infectious condition that could spread along the Eustachian tube (ET) or a space-occupying lesion that blocks ET. Furthermore, the routes of entry of Mtb into the middle ear can not only be via aspiration through ET but also via hematogenous spread from distant sites, or direct implantation through the external auditory canal and tympanic membrane perforation.10,11
Features of middle ear TB have been concluded as painless otorrhea, multiple tympanic perforations, early severe hearing loss, abundant granulation, bony necrosis, whitish necrosis tissue of the middle ear mucosa, and facial nerve palsy. 12 Yet, this diagnosis could be very difficult to establish because of several factors: (1) low occurrence (less than 0.9% of chronic suppurative otitis media cases) and resultant low index of suspicion; (2) highly variable clinical symptoms; and (3) false-negative cultures because of the fastidious nature of Mtb. 11 In addition, many established diagnostic methods suffer from low sensitivity or delay of timely results and are inadequate for rapid detection of Mtb. 13 Fortunately, PCR has been established as a rapid and reliable method for the diagnosis of Mtb. 14 Prompt administration of anti-TB medication could lead to quicker resolution of symptoms and better prevention of relapses.
It is also worth noticing that non-tuberculous mycobacteria (NTM) share many of the clinical features with Mtb, especially positive AFB staining. 15 Yet, NTM is resistant to anti-TB medication.16-18 Hence, it was lucky for the last 2 cases in Table 1, to achieve satisfactory outcomes with anti-TB medication, without confirmation of the species of Mycobacterium. When TB was suspected based on positive AFB staining or characteristic histopathological findings, PCR should be performed to confirm the presence of Mtb, before the selection of treatment modalities. If NTM is present, treatment should be based on surgical resection, and administration of medications might be beneficial.18,19
Conclusion
When otomastoid symptoms respond poorly to local treatment, the nasopharynx should be examined. And biopsy of lesions at both locations should be actively undertaken, to provide histopathological information. If TB is suspected, PCR should be performed to confirm the presence of Mtb, and anti-TB medication could lead to a satisfactory outcome.
Footnotes
Acknowledgements
None.
Author Contributions
X.-S.Z. was the attending doctor of 2 patients in this series, and he reviewed case notes and followed up on the outcome of his patients. H.-Y.X. and S.-S.G. participated in the treatment of the other patient of this series, reviewed the medical record, and followed up on the outcome of this patient. Y.-B.D. and Y.-H.L. made contributions to revising manuscripts. W.-X.L. analyzed the data, reviewed the literature, and was the main writer of multiple versions of manuscripts.
Availability of Data and Materials
All data, models, and code generated or used during the study appear in the submitted article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Beijing Hospitals Authority’s Ascent Plan (grant number DFL20220102), National Natural Science Foundation of China for Young Scholars (grant number 82303642), and Beijing Friendship Hospital Seed Project, Capital Medical University (grant number YYZZ202125).
Ethics Approval
The protocol for the research project has been approved by the Ethics Committee of Traditional Chinese Medicine Hospital of Anshun City, and the Bioethics Committee of Beijing Friendship Hospital, Capital Medical University.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the institutional review board’s approved protocols (approval numbers 20240001 and 2023-P2-269, respectively).
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.