
Abstract
Keywords
Introduction
Infection caused by Mycobacterium tuberculosis (Mtb) species has been included among the ten leading causes of death worldwide in recent years, with millions of individuals developing tuberculosis (TB) infection every year. 1 Rifampicin and isoniazid (INH) are reported to be the most effective first-line drugs against TB. 2 Tuberculosis typically manifests as pulmonary infection, although 14%–20% of the TB cases are those with extrapulmonary infection with lymph nodes as the most frequently affected regions in the body.3,4
Tuberculous lymphadenopathy comprises 35% of all the reported cases of extrapulmonary TB. 4 Lymph nodes serve as favorable sites for the persistence, dissemination, and reactivation of Mtb, while the penetration of anti-TB drugs is lower in the lymph nodes compared to lung granulomas. 5 A large-scale Russian study conducted with several hundred TB patients undergoing lung resection evaluated the levels of RIF and/or INH in the tuberculous foci, bronchopulmonary lymph nodes, and caseous lymph nodes in the period between 2 h and 5 h post-dosing. 6 The study reported that the RIF concentrations in these tissues were 2.43 μg/g, 1.41 μg/g, and .03 μg/g, respectively, while the INH concentrations were .6 μg/g, .53 μg/g, and .21 μg/g, respectively.2,6 This lower drug penetration in the lymph nodes, particularly in caseous lymph nodes, is a challenge encountered in the treatment of tuberculous lymphadenopathy.
Tuberculous lymphadenopathy occurs most commonly in the cervical region (60%–90% of all cases) and typically manifests as unilateral and painless cervical swelling.1,4,7 A definitive diagnosis of tuberculous lymphadenopathy is established based on the detection of Mtb in an affected lymph node by culture or polymerase chain reaction (PCR) analysis, with culture continuing to be the gold standard for this diagnosis even though it requires 2–4 weeks to yield results. 8 Specimens may be collected using one of the following 2 approaches: fine-needle aspiration (FNA) biopsy and excisional biopsy. Fine-needle aspiration biopsy is minimally invasive, cost-effective, and particularly useful in resource-limited developing countries. The PCR analysis enables the detection of Mtb even at numbers as low as 10 Mtb organisms, thereby significantly increasing the overall sensitivity of test. 9 In addition, the time for obtaining the results is dramatically reduced to approximately 6–8 h. 1 Nonetheless, a definitive diagnosis may not always be established due to various reasons, including the paucibacillary nature of tuberculous lymphadenopathy, the limited amount of aspirated tissue available for testing, and a non-uniform distribution of microorganisms in the specimens resulting from the apportioning of the sample for different diagnostic tests (such as histology/cytology, biochemical analysis, microbiology, and PCR analysis).1,4
Current recommendations are to perform an excisional biopsy when the FNA biopsy results are inconclusive. However, excisional biopsy is potentially hazardous as it could spread the disease and lead to sinus formation, 10 particularly in cases with abscess formation. Therefore, when excisional biopsy becomes inevitable, en bloc resection of the entire level of involved lymph nodes is recommended.
It is noteworthy that certain cases of cervical tuberculous lymphadenopathy (CTL) present no positive history, symptom, or positive results in laboratory assays, skin tests, and sputum examinations, and even thorough examination of a FNA specimen could not provide any indication of TB. Only the detection of Mtb nucleic acid in the PCR analysis and/or positive results of culture for the excisional biopsy specimen would firmly establish the diagnosis of CTL. We refer to this condition as occult CTL (OCTL). The present report discusses the diagnosis and management of 14 such cases in immunocompetent adults, whose outcomes were satisfactory.
Patients and Methods
The present study was designed as a retrospective study of patients with OCTL treated at the Department of Otolaryngology-Head & Neck Surgery, Beijing Friendship Hospital, Capital Medical University, between June 2015 and Dec 2020. The definition of OCTL considered in the present study is provided in the “inclusion criteria” section below. The clinical and demographic data of these patients were collected from case notes.
Diagnostic Examination
All included patients had presented with unilateral painless swelling in the neck. The medical history of each of these patients was reviewed in detail, and the history of Bacillus Calmette–Guerin (BCG) vaccine inoculation (mandatory in China) was confirmed. The patients were inquired regarding any history of possible Mtb exposure and significant associated symptoms such as fever and night sweat. After the physical examination, these patients were subjected to different analyses, including chest CT, tuberculin skin test (TST) with purified protein derivative (PPD), and interferon-gamma release assay (IGRA), along with the evaluations of blood cell count and C reactive protein, erythrocyte sedimentation rate (ESR), serum glucose level, renal function, hepatic function, and anti-human immunodeficiency virus (HIV) antibody. Cervical CT and MRI with contrast were conducted. Fine-needle aspiration biopsy was performed under the guidance of ultrasound. Acid-fast bacilli staining and culture for Mtb were performed using sputum samples. In addition, histology, AFB staining, and culture and PCR for Mtb were performed using the FNA biopsy specimens. When none of these analyses could establish a definitive diagnosis, the surgical excision of the entire levels of involved lymph nodes was performed, and the excisional specimens were subjected to histology, AFB staining, and culture and PCR for Mtb to establish the final diagnosis.
Inclusion and Exclusion Criteria
Inclusion criteria. In order to be included in the present study, the individual had to be diagnosed with OCTL. A patient was considered to be having OCTL if all the following criteria were fulfilled: the presence of painless cervical lump (gradual increase in its size was acceptable), no prior history of Mtb exposure, history of BCG vaccine inoculation was confirmed, and no typical TB symptoms were present; no signs of pulmonary TB (not even calcified foci, as these indicate prior infection) appeared on chest CT; the results of both TST with PPD and IGRA were negative; ESR was not elevated; HIV seronegative; not diabetic; no renal insufficiency; results of both AFB staining and culture of sputum specimen were negative; the results of histology, AFB staining, and the culture and PCR of the FNA specimen were negative; in the final excisional specimen examinations, PCR and/or culture was positive for Mtb, AFB staining could be positive or negative, and granulomatous inflammation and/or caseous necrosis could be present or absent.
Exclusion criteria. A patient was excluded from the present study if any of the following conditions were fulfilled: history of Mtb exposure, BCG vaccine not inoculated, any TB-related symptom such as fever and/or night sweat, positive findings on chest CT, positive result in TST with PPD or IGRA, elevated ESR, HIV seropositive, diabetic, renal insufficiency, positive result in sputum examination (AFB staining and/or culture), or positive FNA specimen examination result (histology, AFB staining, and culture and/or PCR).
Surgical Procedure
An incision was made along the cervical skin crease adjacent to or on top of the cervical lump Subplatysmal flaps were elevated, which revealed an evident lump anterior or posterior to the sternocleidomastoid muscle (SCM). After the identification of important nerves (such as accessory nerve or hypoglossal nerve) and vessels (such as the internal jugular vein (IJV) or common carotid artery), the en bloc resection of the entire levels of involved lymph nodes was performed. The wound was irrigated sequentially with peroxide, saline, diluted iodophor, and saline again. A negative-pressure suction device was placed, and the incision was closed. Preoperative imaging analysis of Case 5. (A) Computed tomography (CT) image with contrast depicting irregular right level V lesion with mild peripheral enhancement, which was indistinguishable from sternocleidomastoid muscle (SCM). (B and C) MRI T2 and T1 images depicting long T2 and long T1 signals at the center of the lesion, indicating abundant fluid content. (D) Magnetic resonance imaging T1 image with contrast, again depicting irregular right level V lesion with mild peripheral enhancement. SCM: sternocleidomastoid muscle.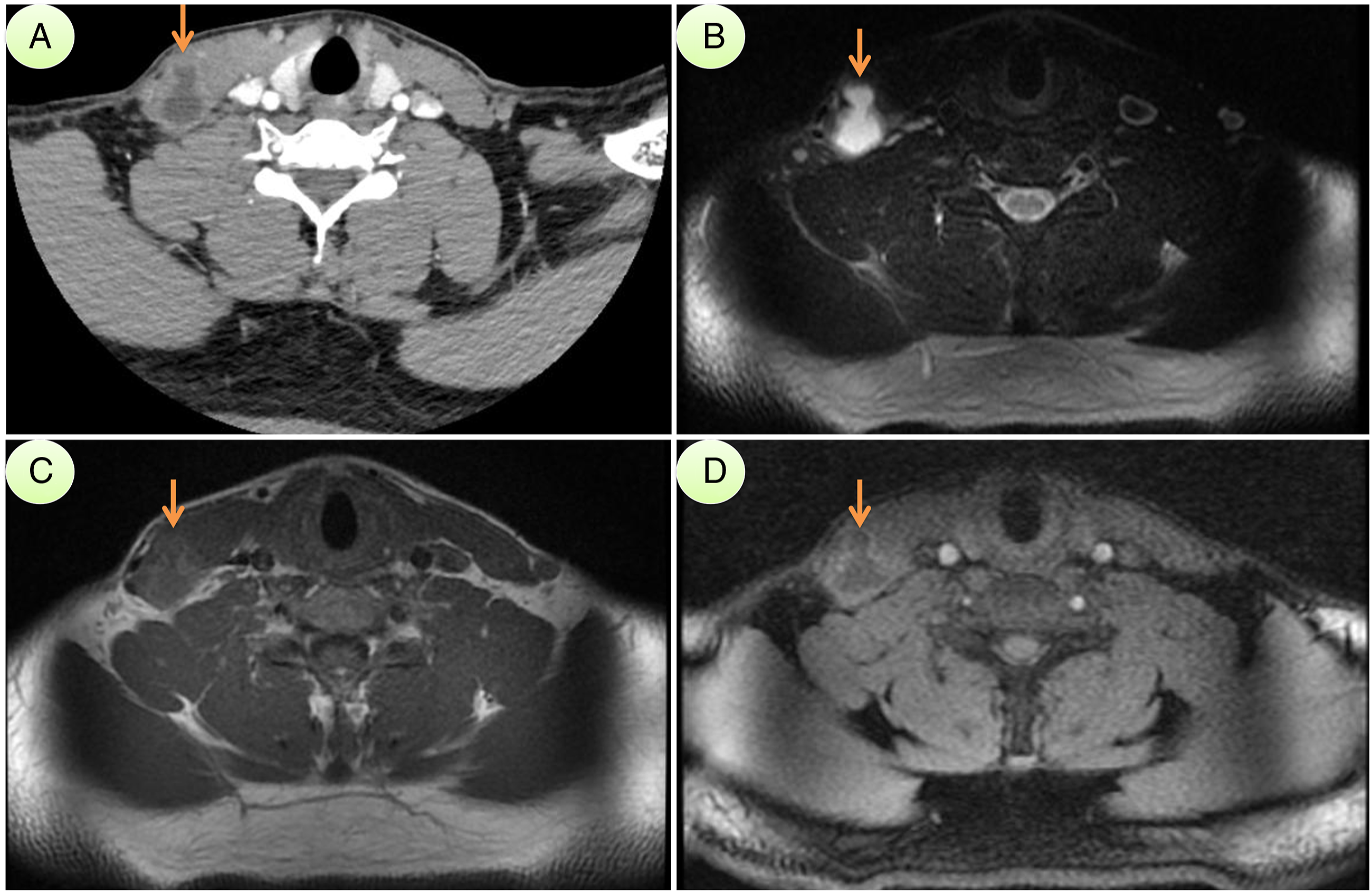
Anti-TB Chemotherapy
Upon the establishment of a definitive diagnosis of OCTL, the patient was prescribed 6 months of anti-TB chemotherapy, which included therapy with RIF, INH, pyrazinamide, and ethambutol for 2 months, followed by therapy with RIF and INH for the next 4 months. 8
Follow-Up
All patients were followed up routinely, every 2 months, after the surgery, for the inspection of wounds and identification of the signs, if any, of TB relapse.
Results
Clinical data of this series of occult cervical tuberculous lymphadenopathy.
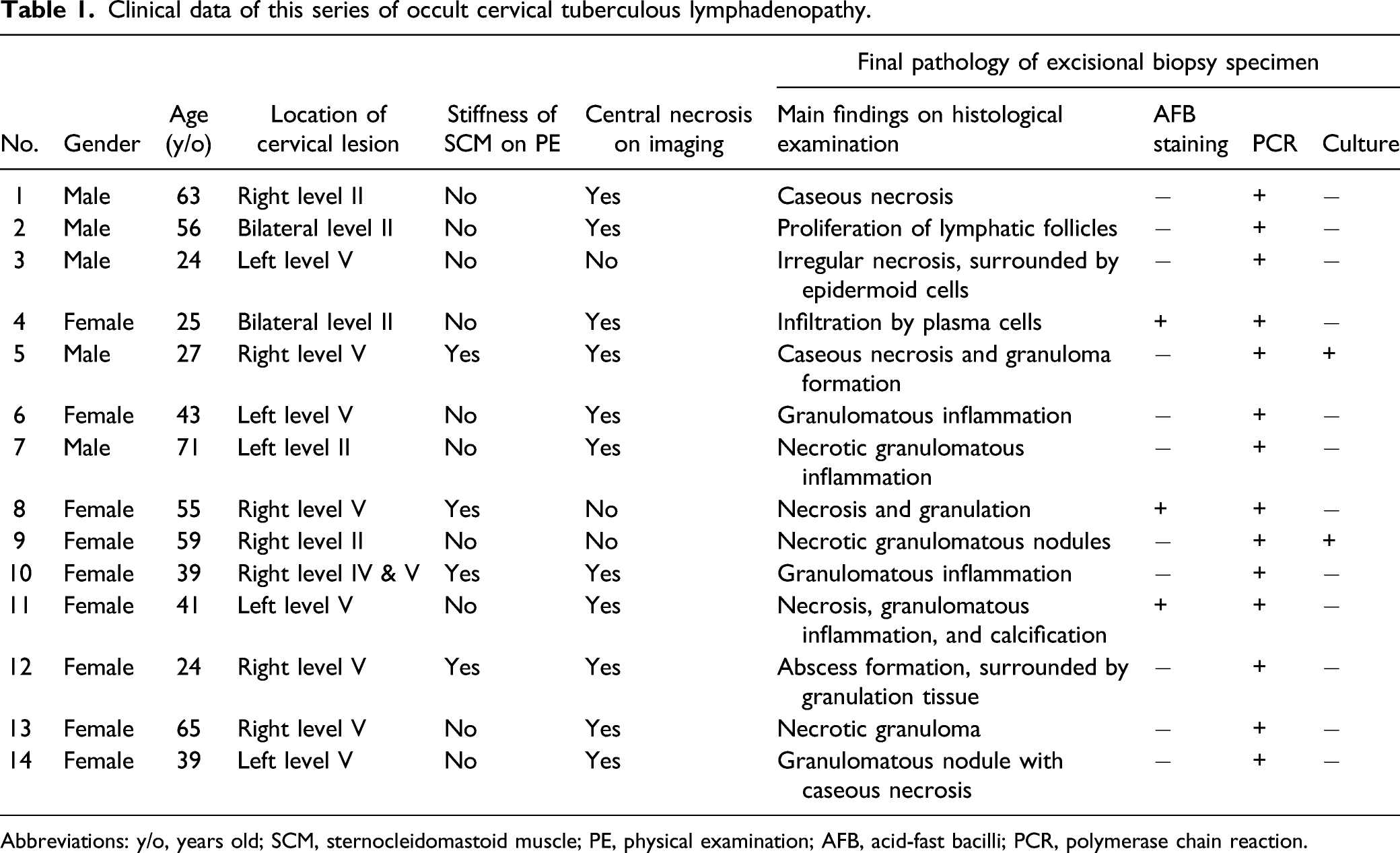
Abbreviations: y/o, years old; SCM, sternocleidomastoid muscle; PE, physical examination; AFB, acid-fast bacilli; PCR, polymerase chain reaction.
In the physical examination, stiffness of the entire posterior margin of SCM was observed in 4 patients, all of which were associated with level V lesions, as presented in Table 1. However, no complaint of discomfort associated with this physical sign was conveyed by these 4 patients. It was inferred that this physical sign could have resulted from the extensive involvement of SCM, yet it had evidently extended far beyond the superior margin of the cervical lesion. Fortunately, this physical sign was resolved between 10 days and 2 months after the initiation of anti-TB chemotherapy, further supporting the inference that it was a result of TB-related inflammation.
In preoperative imaging (CT and/or MRI with contrast), central necrosis was observed in 11 cases Figure 1. Intraoperatively, 12 cases presented the involvement of SCM, while 2 cases presented the involvement of IJV together with intra-SCM abscess formation. In 1 case with IJV involvement, the capsule of the removed cervical lesion was not completely intact, which happened in an attempt to preserve the IJV. In the other case with IJV involvement, 3 cm of the IJV was encased by the lesion and had to be sacrificed. Moreover, the surgical procedures were performed in the manner of selective neck dissection, with the removal of the part of the SCM involved (the complete transection of the SCM was not required in these 12 cases). Recovery of all patients was uneventful, without any major complications such as wound dehiscence or sinus formation.
The final pathology reports of the excisional specimens revealed positive PCR findings for all 14 cases, among which only 2 cases presented positive cultures (Case 5 with central necrosis and Case 9 without central necrosis), and 3 cases exhibited positive AFB staining (Case 4 and Case 11 with central necrosis and Case 8 without central necrosis). Various histological findings, presented in Table 1, were observed, although without any evident pattern.
Since the PCR analysis provided rapid and conclusive results, all 14 patients were prescribed standard anti-TB chemotherapy. The patients were followed up routinely, every 2 months, after the surgery. The follow-up duration was between 6 months and 69 months (median duration 29 months). All 14 patients completed the prescribed 6 months of anti-TB chemotherapy. No cervical discomfort or TB relapse was observed during the follow-ups to date, and no apparent side effects of the anti-TB chemotherapy were documented.
Discussion
In current times, TB remains a major health challenge in most developing countries, while the increased prevalence of HIV and an ever-increasing immigration rate had led to the re-emergence of TB in the developed nations. 7 Unfortunately, the route of Mtb into cervical lymph nodes remains elusive so far, particularly in cases not exhibiting pulmonary TB.
Differential diagnosis of cervical lymphadenopathy is challenging. The infectious causes of cervical lymphadenopathy include Mtb, nontuberculous mycobacteria (including Mycobacterium scrofulaceum, Mycobacterium avium, and Mycobacterium haemophilum), Toxoplasma species, Bartonella species, and fungi. The non-infectious causes of this disease include neoplasms, sarcoidosis, Castleman disease, drug reactions, and non-specific reactive hyperplasia. 8 Although a high index of suspicion of TB is fundamental, particularly in endemic regions, other unrelated conditions are also required to be excluded.
It is believed that uncontrolled multiplication of bacilli within a lymph node causes the necrosis of the lymph node, leading to the formation of an abscess. Therefore, it is expected that the FNA specimen from a tuberculous abscess contains greater AFBs compared to the early tuberculous lymph nodes. 10 Moreover, the presence of necrosis and/or neutrophilic inflammation in the tissue samples is reportedly correlated with culture positivity. 11 However, this is not the case in OCTL, as revealed by the results obtained in the present study, according to which neither positive AFB staining nor culture positivity was detected in the FNA specimens, regardless of the central necrosis. Moreover, the examination of the excisional biopsy specimens revealed positive AFB staining in 3 cases and positive culture in 2 cases, although these cases were not related to central necrosis either (Table 1). It was inferred that this phenomenon occurred due to the paucibacillary nature of intranodal Mtb 4 combined with the immunocompetency of the host. In an immunocompetent adult, macrophages would be able to phagocytize all intranodal Mtb organisms, although these Mtb would not be eliminated because of the high lipid content of their cell walls and the high mycolic acid content of their outer capsules. 12 Therefore, the presence of abscess/necrosis in OCTL does not indicate uncontrolled Mtb proliferation.
In the 20th century, for the most part, tuberculous lymphadenopathy was treated by performing a wide excision followed by long-term anti-TB chemotherapy. However, in modern times, with the introduction of effective short-course rifampin-based chemotherapy, it has become an easily treatable disease. 11 Nonetheless, the cases of OCTL raise a unique challenge in terms of diagnosis and management, thereby rendering the use of wide surgical excision crucial. In addition, since OCTL presents no evidence of TB, it is important to broaden the range of differential diagnosis for OCTL and not to exclude the possibility of metastatic lymphadenopathy. The surgical procedures performed in the present study were in accordance with the principle of tumor excision, that is, the en bloc excision of the entire tissue involved through selective neck dissection while maintaining intact the outermost fibrous capsule, which is considered the most important marker of successful treatment. The advantage of this procedure is that the probability of disease spread is minimum, regardless of whether it is TB or tumor.
There are also other indications for utilizing surgical excision to manage CTL. One important among these is preoperative baseline tenderness, which predisposes the patient to paradoxical upgrading reaction (PUR) that manifests as an expansion of and drainage from the lymph nodes during the anti-TB chemotherapy. 11 The characteristics of biopsy or culture of the nodes involved in PUR are consistent with a robust immune response to Mtb upon the initiation of anti-TB chemotherapy, along with the release of mycobacterial antigens. 8 Indeed, PUR is not uncommon and reportedly occurs in up to 23% of patients after the initiation of anti-TB chemotherapy.13,14 PUR occurrence and significant discomfort experienced by the patient are indications for surgical excision. 11 Moreover, if the anti-TB chemotherapy fails to resolve lymphadenopathy, it is also an indication for surgical excision. 8 It is noteworthy that PUR did not occur in any of the cases in the present study as most Mtb organisms had been removed in the surgery itself.
Certain scholars advocate that in CTL, the scope of surgical excision is limited to guiding the FNA, incision and drainage, and incisional and limited excisional biopsy, while major excisional procedures should be avoided. 15 However, in the cases presenting OCTL, significant discomfort caused by PUR, and failure of anti-TB chemotherapy, en bloc surgical excision of all the involved tissues is recommended to relieve the patient from discomfort and the disease. Moreover, in the experienced hands of senior surgeons, it becomes possible to minimize complications, as demonstrated in the cases discussed in the present study.
Conclusions
Occult cervical tuberculous lymphadenopathy raises a significant challenge in the differential diagnosis of a cervical lump. Therefore, for diagnosis and management, it becomes crucial to perform en bloc excision of the entire levels of the involved lymph nodes, which, when combined with standard anti-TB chemotherapy, could lead to satisfactory outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Research and Development Project of Scientific Research Instruments and Equipment of Chinese Academy of Sciences-major instruments project (YJKYYQ20180039), and the Digestive Medical Coordinated Development Center of Beijing Municipal Administration of Hospitals (No. XXZ0604), and Key Science and Technology Program of Beijing Municipal Commission of Education (KZ202110025035).