
Abstract
The posterior transverse cordotomy (PTC) can be performed for posterior glottic stenosis (PGS) in the operating room through suspension laryngoscopy. This procedure requires adequate exposure of the vocal cords. An alternative PTC approach was carried out on a 56-year-old man without a view of the vocal cords during suspension laryngoscopy. After anteriorizing the hypertrophic tongue with a glide scope, the surgeon reached the vocal folds through a flexible nasofibroscopy with an operative channel. The adequate exposure of the posterior part of the vocal cords allowed the blue laser PTC through the operative channel in the cut setting. The postoperative outcomes were adequate in the follow-up period. This paper describes an alternative approach to PTC in a patient with PGS and several unsuccessful laryngeal exposures.
Introduction
Posterior glottic stenosis (PGS) is a total or partial fixation of the vocal folds as a result of cricoarytenoid joint fixation, scarring of the posterior glottic structures, interarytenoid fibrous adhesion, or synechia. 1 The PGS occurs in 14% of adult patients following prolonged intubation. 2 The treatment depends on the severity of the PGS that can be evaluated with the Bogdasarian and Olson Classification. 1 Four PGS types were described with type IV consisting of the fixation of both cricoarytenoid joints. 1 To date, there is no consensus on the surgical management of PGS. The surgical procedures can include uni- or bilateral posterior transverse cordotomy (PTC), posterior transverse cordectomy with or without ventriculostomy/ventriculectomy, total or partial cricoarytenoidectomy, and laryngeal framework with a posterior flap or costal graft. 3 All of these procedures are carried out in suspension laryngoscopy in an operating room. The success of the procedures is influenced by the laryngeal exposure of patients. 4 In practice, the larynx of some patients is difficult to expose, and they need to undergo open procedures with tracheotomy, and related quality-of-life and cost burdens. 4
In this paper, we described the realization of a transoral flexible blue laser PTC in a patient without adequate laryngeal exposition.
Case Presentation
A 56-year-old man was referred to the Laryngology Division of the EpiCURA hospital for a 12-month history of dyspnea related to a type IV PGS. The PGS occurred after a 6-week history of intubation for severe coronavirus disease 2019. The patient was limited to walking more than 400 m. The medical history of the patient included obesity and obstructive sleep apnea syndrome. The laryngostroboscopic examination showed total immobility of the right vocal cord (in adduction), and partial but limited mobility of the left vocal cord (Figures 1 and 2). The lung evaluations did not reveal pulmonary disorders (forced expiratory volume 1/vital capacity = 85%). A PTC was proposed to the patient in 2 academic hospitals before the consultation but the laryngologists failed to expose the larynx with several laryngoscopes due to severe tongue base hypertrophy, and a reduction of the laryngopharyngeal space related to the obesity of the patient.
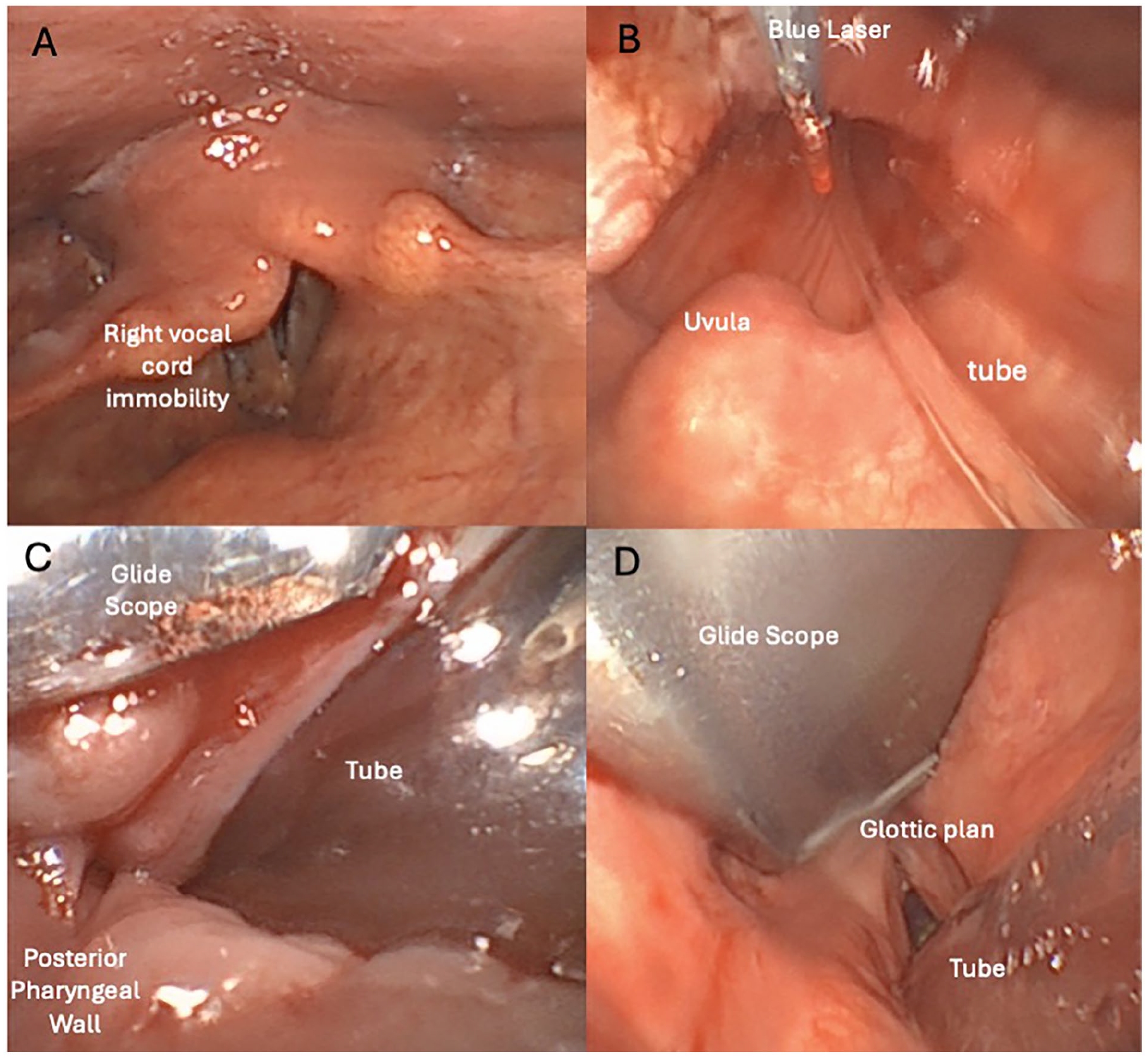
Surgical exposition of the glottic plan. The patient had total right vocal cord immobility and partial mobility of the left vocal cord (A). The oropharyngeal space was obstructive (B, C). The glide scope allowed the opening of the supraglottic space (D), leading to better access for the fiberscope with the blue laser fiber (B).
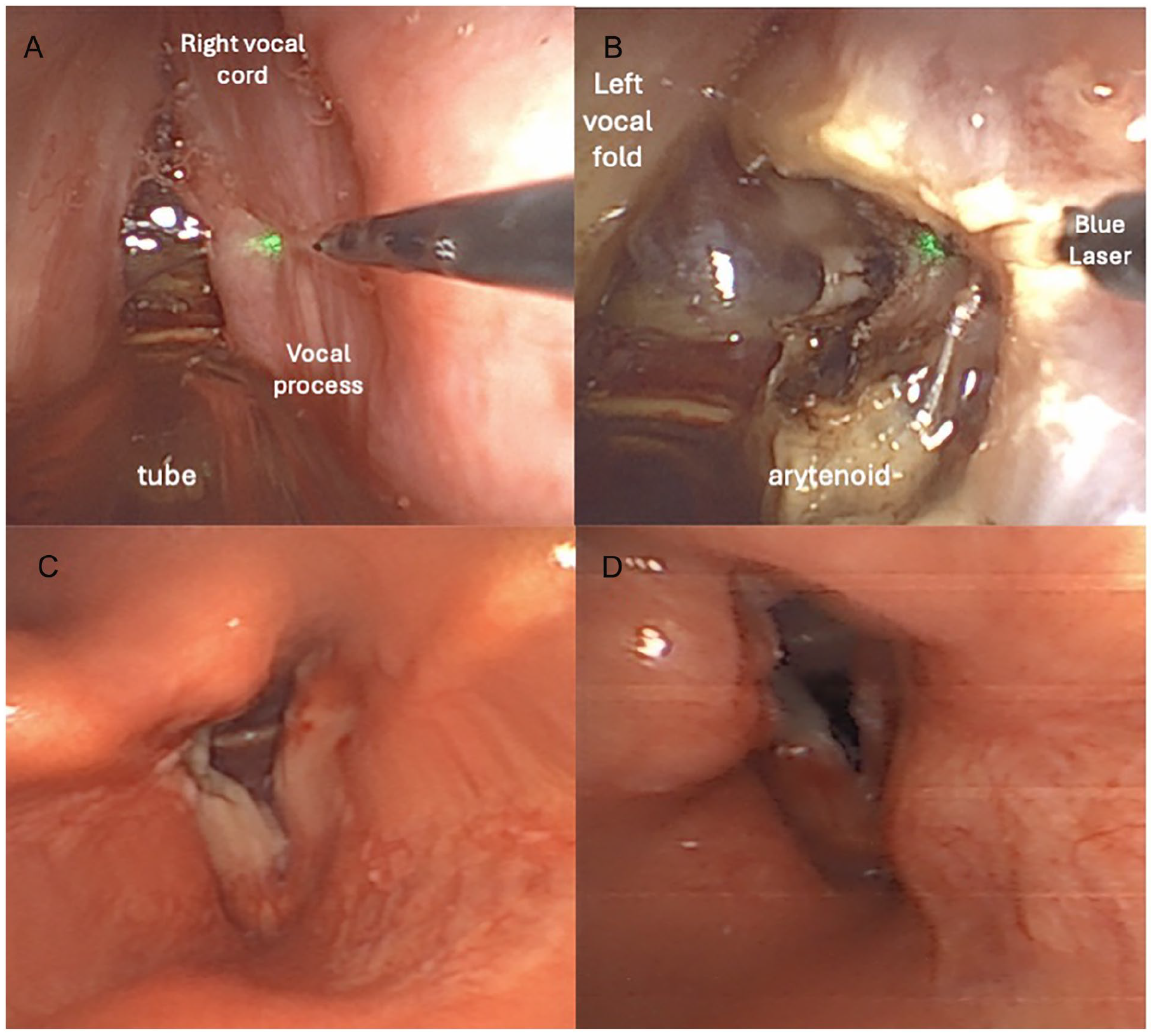
Vocal cord incision and postoperative examination. The limit between the anterior part of the vocal process and the vocal cord soft tissue is delimited with palpation with the blue laser fiber (A). The posterior transverse cordotomy is carried out (B), leading to adequate postoperative outcomes at 1 week (C) and 1 month (D) follow-up.
The laryngologist (J.R.L.) proposed to perform the laser PTC through the operative channel of a flexible nasofibroscopy. The intubation of the patient was difficult, but the anesthesiologist succeeded with the glide scope, a pediatric tube, and an incurved Eschmann tracheal tube. Note that the glottic plan was not viewable and the intubation was carried out blindly with the incurved Eschmann tracheal tube. An attempt to expose the larynx was carried out by the laryngologist but it was impossible with various laryngoscopes, including anterior commissure or pediatric laryngoscopes. The base of the tongue was therefore anteriorized with a glide scope, to open the oropharyngeal space and the flexible nasofibroscopy with an operative channel (Xion GmbH, Berlin, Germany) was introduced into the mouth with the blue laser fiber (Soluvos Medical BV, Eindhoven, the Netherlands) in the operative channel (Figures 1 and 2). The laryngologist performed the right PTC with the blue laser in a cut setting (Septoplasty Setting, 4 W). The surgery time was 30 minutes. The durations of the exposure of the vocal cords through the flexible fibroscopy and the PTC were 25 and 5 minutes, respectively. The saliva of the upper aerodigestive tract was continuously aspired with an incurved aspiration. The patient received IV corticosteroids (Solumedrol; 1 mg/kg) at the end of the procedure to reduce the risk of postoperative edema. The corticosteroid therapy was continued for 7 days (32 mg of per os Solumedrol). There was no immediate or delayed complication. The patient was discharged after 24 hours of clinical surveillance. The postoperative glottic space (Figures 1 and 2) was adequate, and the patient’s dyspnea disappeared. Note that the written consent was obtained for the patient.
Discussion
Some patients with severe PGS are difficult to expose for vocal cord surgery, leading to the consideration of other options, such as open procedure or tracheotomy, to address the dyspnea and the related breathing symptoms. The blue laser is mainly used for in-office procedures in awake patients with superficial benign lesions of the vocal folds with a small risk of perioperative bleeding. In the present study, we reported a case of PTC using a flexible nasofibroscopy in a patient with a glottic plan considered unexposable. To the best of our knowledge, there is no similar procedure described in the Medline literature. The PGS procedures are commonly performed in the operating room, given the risk of bleeding. 5 For this reason, the procedure reported in the present paper was not carried out in awake patients. Indeed, PTC includes a section in the vocal cord muscle, which can bleed, and, consequently, lead to the realization of an emergent tracheotomy in the patient.
The transoral flexible blue laser PTC can be indicated for patients with severe PGS without adequate laryngeal exposition. According to the possibility of cutting soft tissue with the blue laser fiber at a wide angle (Figure 3), the best indications are still unilateral or bilateral PTC in patients with the impossibility of exposing the larynx. The posterior partial cordotomy can be theoretically performed in all awake patients but considering the risk of hemorrhage, most authors did not perform this procedure in-office without intubation. The radial laser incision of a type I PGS in a patient without an exposed larynx could theoretically be an additional indication.
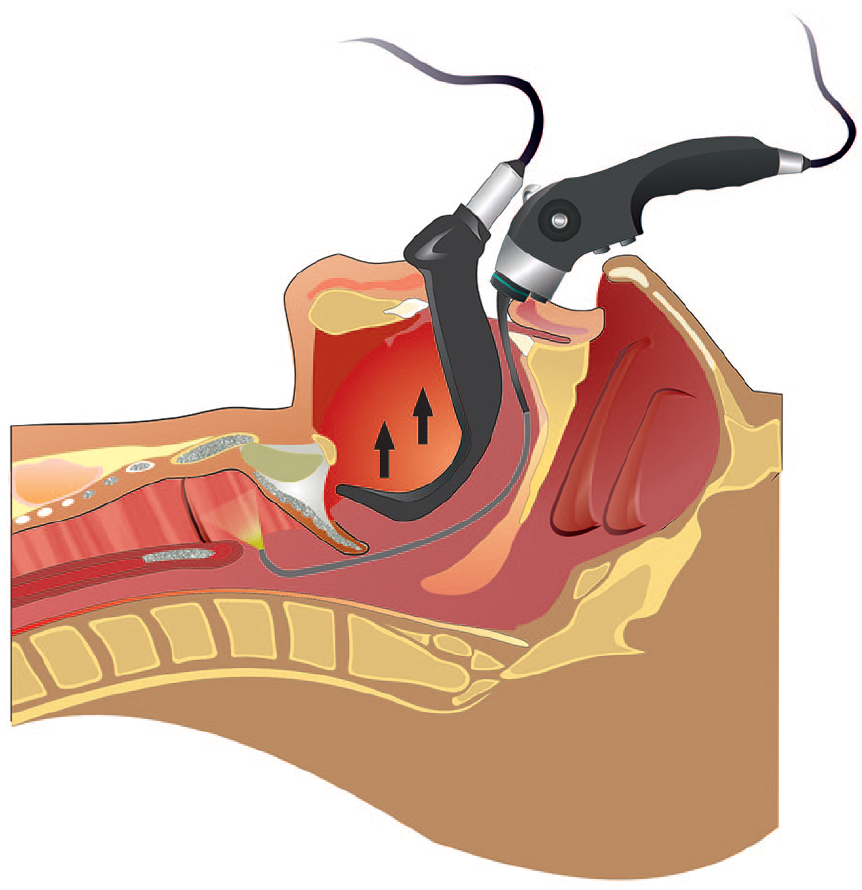
Summary of the procedure.
The intubation of the patient is an important step to avoid complications. Indeed, if bleeding occurs during the procedure, the patient’s airway is protected by the cuffed tube. Note that the blue laser setting can be changed from a cut mode to a hemostasis mode. The use of the Reinke edema mode can be adequate for performing superficial hemostasis.
Percutaneous transcricoid intubation can be an alternative airway approach in cases of inability to intubate the patient but this approach requires a trained anesthesiologist. A transient tracheotomy is another alternative for protecting the airway during the surgery, but it is associated with a quality-of-life and cost burden for the patient and healthcare system, respectively.5-7 Interestingly, given the flexible properties of the fiberscope and the wide-angle head of the fiberscope, the flexible blue laser PTC can be theoretically performed through the tracheotomy (modified fenestrated cannula) avoiding an open approach and the related muscle and laryngeal tissue injuries. Finally, the administration of IV corticosteroids (1 mg/kg) is particularly important to reduce the risk of postoperative edema and dyspnea in such patients who are difficult to intubate.
Some preoperative considerations have been made in the present case, including the health assessment for the anesthesiologic risk and the dental condition for a direct laryngoscopy attempt. The team must be carefully informed about all steps of the procedure, from the narcosis to the surgery. A tracheotomy instrument tray should be prepared in case of tracheotomy, as well as a pediatric tube and the Eschmann tracheal tube.
Specific information is important to give to the patient. The primary consideration is the risk of tracheotomy. The patient must be aware that the intubation procedure is as difficult as laryngeal exposure with the flexible fiberscope. In case of inability to intubate or ventilate the patient, the tracheotomy should be performed to protect the airway during the surgery. Because patients with intubation difficulties are often obese and have limited oropharyngeal and laryngopharyngeal space, ventilation through the oxygen mask is often ineffective. Tracheotomy carries an immediate or delayed surgical risk, the latter being related to a postoperative dyspnea or airway complication.
The secondary consideration is the risk of conversion to open surgery. Before potential conversion, the laryngologist could theoretically attempt to reach the vocal cords through the tracheotomy using a modified fenestrated cannula allowing the passage of the flexible fiberscope (upward exposition).
The inability to have an adequate vertical up-to-down view of the cricoarytenoid joint with the use of a flexible approach limits the use of this procedure for carrying out cartilage surgeries, such as anterior partial cricoarytenoidectomy or partial arytenoidectomy with posterior transverse cordectomy. Similarly, the lack of forceps to mobilize laryngeal tissues makes this approach limited for partial transverse cordectomy with or without ventriculectomy.
Conclusion
The rationale for publishing this case is to describe an easy and safe procedure which is an alternative approach to external procedure or long-term tracheotomy. Future case series are needed to provide functional and surgical outcomes of transoral flexible blue laser PTC.
Footnotes
Author Contributions
J.R.L.: writing, drafting, patient treatment, and follow-up. E.B.Q.: proofread the paper, patient treatment, and follow-up.
Data Availability Statement
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical/Consent Statement
The present case presentation did not require an ethics committee agreement.
Informed Consent
The patient consented to the publication.