
Abstract
Background:
The recent introduction of 445 nm blue laser to office-based laryngology presents potential advantages. These include a desirable combination of cutting and photoangiolytic qualities and a lightweight, shock-resistant design. Despite its increasing use, current evidence is limited to experimental data and case reports.
Objectives:
The authors present a case series and overview of office blue laser transnasal flexible laser surgery (TNFLS), considering indications, patient selection, safety, technique, and surgical outcomes. We also review the safety and relevance of TNFLS to the ongoing coronavirus pandemic.
Methods:
Retrospective case series and narrative review. Our primary outcome measure was preoperative and postoperative Voice Handicap Index (VHI-10) score. Complications were documented by nature and severity.
Results:
Thirty-six cases of office blue laser TNFLS were performed. A statistically significant improvement in VHI-10 score was demonstrated in cases of recurrent respiratory papillomatosis (RRP) and benign laryngeal lesions causing dysphonia (P < 0.01 and 0.045). Blue laser also proved effective in assisting office biopsy procedures. A minor and self-limiting complication was reported.
Conclusions:
Office blue laser TNFLS is safe and effective in the treatment of RRP and a range of benign laryngeal lesions. Future research should compare the efficacy and safety of blue laser with potassium titanyl phosphate laser in office-based treatment of these conditions. Further assessment of the cutting qualities of blue laser, initially in the theater environment, is necessary to refine our understanding of future applications.
Keywords
Introduction
Since its introduction by Zeitels et al in 2004 in the treatment of recurrent respiratory papillomatosis (RRP), office-based transnasal flexible laser surgery (TNFLS) has become widespread in laryngology. 1,2 A multitude of benefits are well established, primarily relating to minimized morbidity, patient inconvenience, and associated costs of theater-based surgery under general anesthesia. 3 -5 A range of lasers are currently used in TNFLS, primarily photoangiolytic varieties such as the 585 nm pulsed-dye laser (PDL) 1,6 and the 532 nm potassium titanyl phosphate (KTP) laser, 7 the latter being the most widely studied and utilized. 7 The use of cutting lasers such as the 10 600 nm CO2 laser 8 remains limited in the office setting due to its comparatively expensive flexible glass fibers and poorer coagulation profile.
The 445 nm blue laser (TruBlue; A.R.C. Laser Company), recently CE mark certified, was first described in its applications to laryngology in 2018 and represents the most recent development in TNFLS. 9 Proposed advantages include device portability and a desirable blend of photoangiolytic and cutting properties. Although the feasibility and efficacy of blue lasers and its “dual” characteristics have been clearly demonstrated in laboratory- and animal-based studies, there is no systematic data on clinical outcomes. 9,10 The authors address this with a case series of office-based blue laser TNFLS, with additional consideration given to case selection, technique, safety considerations, and applications in the context of the ongoing coronavirus pandemic.
Case Selection
A wide range of laryngological diseases are amenable to TNFLS, including telangiectasia, RRP, polyps, granulomas, and biopsy, when patients are not suitable for general anesthesia. 5 Although specific data on blue laser are limited to cases performed under general anesthesia, 9 in the authors’ experience, office blue laser TNFLS is both efficacious and safe in all of the above applications.
Patient Selection
Theoretically, any patients able to remain stationary and composed for the duration of the procedure may be considered for TNFLS, and it is often the favored modality of treatment precisely because of a patient’s high general anesthetic risk. Nonetheless, the physical and psychological stress of undergoing invasive airway surgery, unsedated and in unfamiliar surroundings, must not be underestimated, with particular attention given to underlying cardiovascular disease, with transient periprocedural hypertension and tachycardia commonly reported. 11 Preoperative cardiovascular screening through history and basic examination with onward referral when appropriate is therefore essential to minimizing perioperative risk.
In one of the largest TNFLS case series, the most commonly encountered complications were transient vasovagal episodes (4.1%) and early termination of the procedure due to patient tolerance (13.1%). 12 Comprehensive preoperative counseling on patient experience is essential to mitigate these risks and should include patient familiarization with the office environment and team, completion of informed consent, and provision of written and video literature on TNFLS, prior to the day of surgery.
Although early data suggest that continuation of antithrombotic medication is safe in TNFLS, pending more robust data, the authors continue to recommend cessation where possible, in liaison with relevant medical teams, given the implications that a significant airway hemorrhage in the office setting would pose to both patients and future practice. 13
Laser and Office-Based Procedure Safety in the Context of Coronavirus
As with all procedures involving lasers, specific laser safety precautions are paramount to minimize risk, which can arise from both inexperience and over familiarity. In our practice, all outpatient staff involved in TNFLS complete a formal laser safety training program, and a standardized preoperative laser safety checklist is completed prior to the commencement of surgery. 14 This includes universal standard precautions such as goggles worn by patient and staff and clear signage outside the procedure room.
In the context of the ongoing coronavirus pandemic, a majority of professional bodies have recognized office-based surgery as a high-risk aerosol-generating procedure, 15 -20 and in the authors’ view, it is difficult to overstate the importance of adequate personal protective equipment and ventilation. In our institution, all team members present during surgery wear powered air-purifying respirator hoods in addition to full-length gown and gloves (Figure 1). To ensure adequate ventilation, the procedure room is fitted with a negative pressure high-efficiency particulate air filtration unit (Filtrex).

Demonstration of standard personal protective equipment (powered air-purifying respirator hood, full-length gown, and gloves) worn during office blue laser transnasal flexible laser surgery.
Technique
Following administration of 2.5-mL 5% lidocaine/5% phenylephrine (co-phenylcaine) spray and 10 sprays of 10% oral xylocaine, a transnasal channeled endoscope is introduced. The epiglottis and larynx are further anesthetized with 2.5 mL lidocaine/phenylephrine; this is applied either transorally with a transoral “MADgic” atomizer (Teleflex) or by a catheter dropper through the instrument channel, with the patient asked to phonate on application, to ensure comprehensive distribution (Figure 2). Completeness of anesthesia may be assessed by gently palpating the epiglottis and arytenoids with the endoscope tip, with top-up anesthesia applied as required.
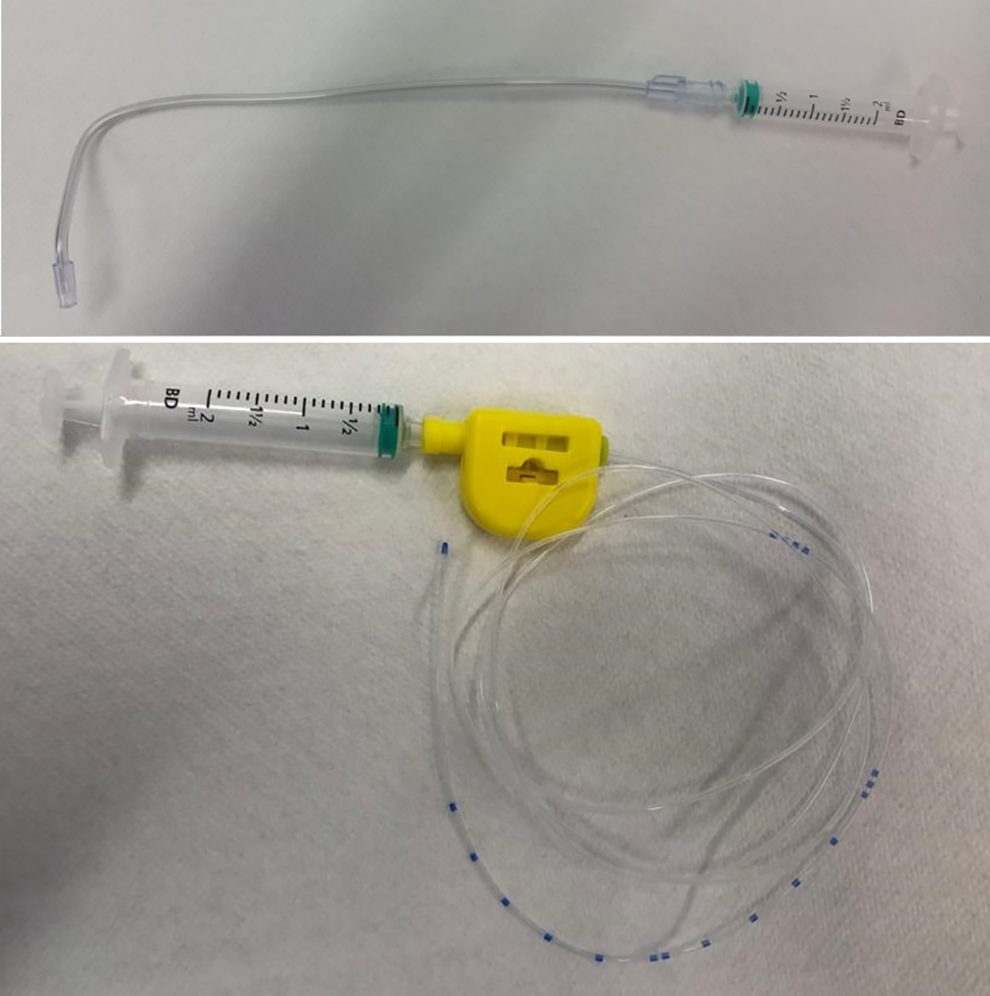
MADgic atomizer (above) and catheter dropper (below). The latter is commonly available in epidural catheter packs.
The laser is subsequently introduced through the working channel until fully visualized on the screen. The laser is fired at the target tissue from a working distance of between 1 and 4 mm until the desired outcome is achieved (Figure 3). In the absence of a handheld micromanipulator, cutting qualities are best achieved by means of a steady close to target movement. 9 If biopsy is to be performed, blue laser may be used to devascularize and thin a pedicle prior to its removal with channeled or transoral biopsy forceps (Figures 4 and 5). Care must be taken to avoid thermal injury to the biopsy specimen. Laser settings can be tailored to a wide range of contexts, although in the authors’ experience, a baseline setting of 10 W, continuous superpulse, 60 milliseconds on 120 milliseconds off, produces an effective blend of the cutting and photoangiolytic qualities.
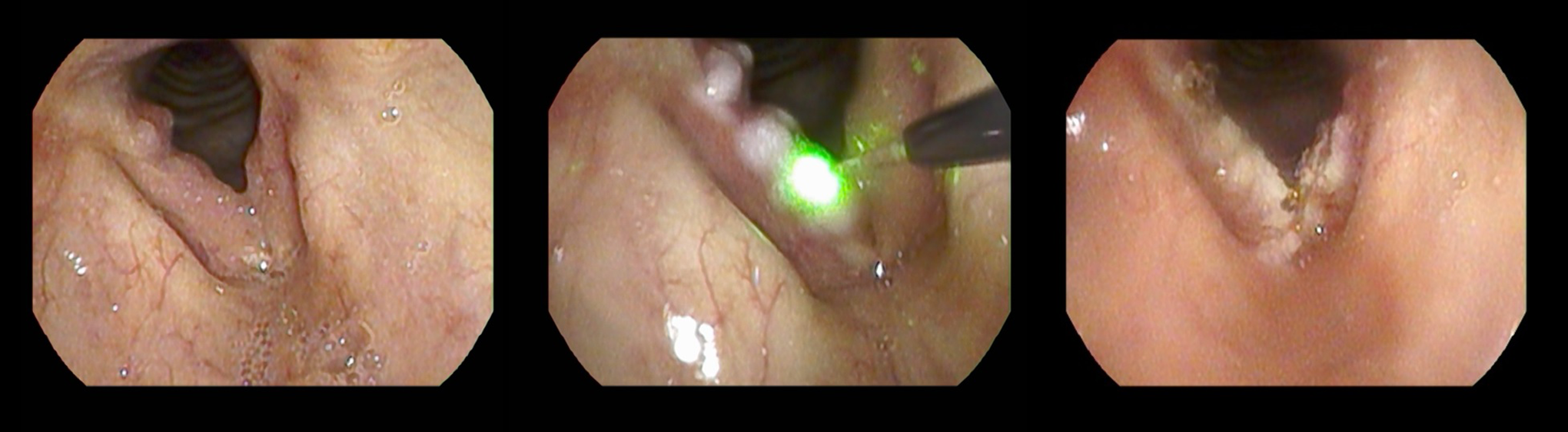
Recurrent respiratory papillomatosis (left). Intraoperative blue laser debulking (middle). Immediate postoperative appearances (right).
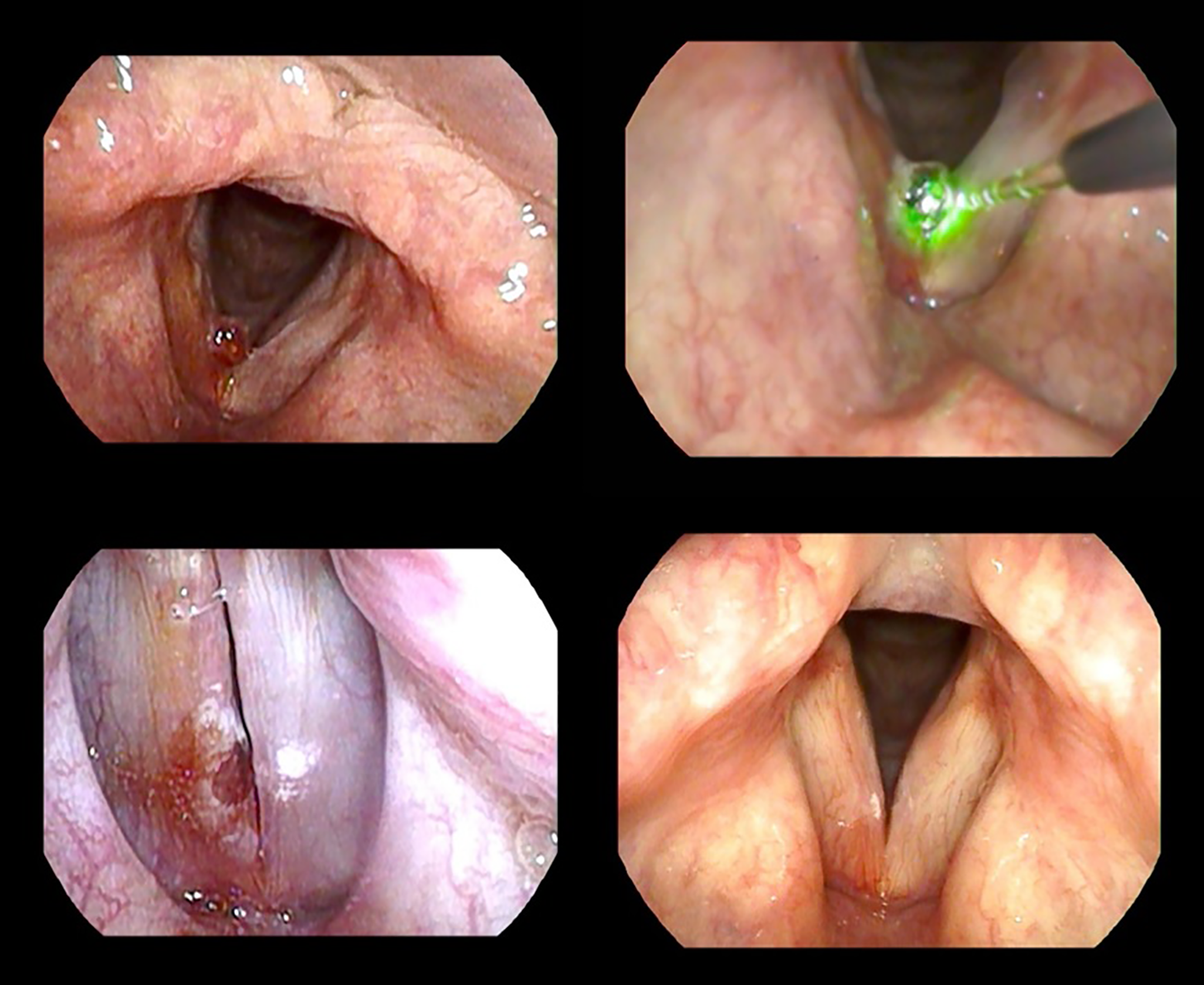
Right vocal cord hemorrhagic polyp (top left). Intraoperative blue laser excision (top right). Immediate postoperative appearances (bottom left). Two-month postoperative appearances (bottom right).
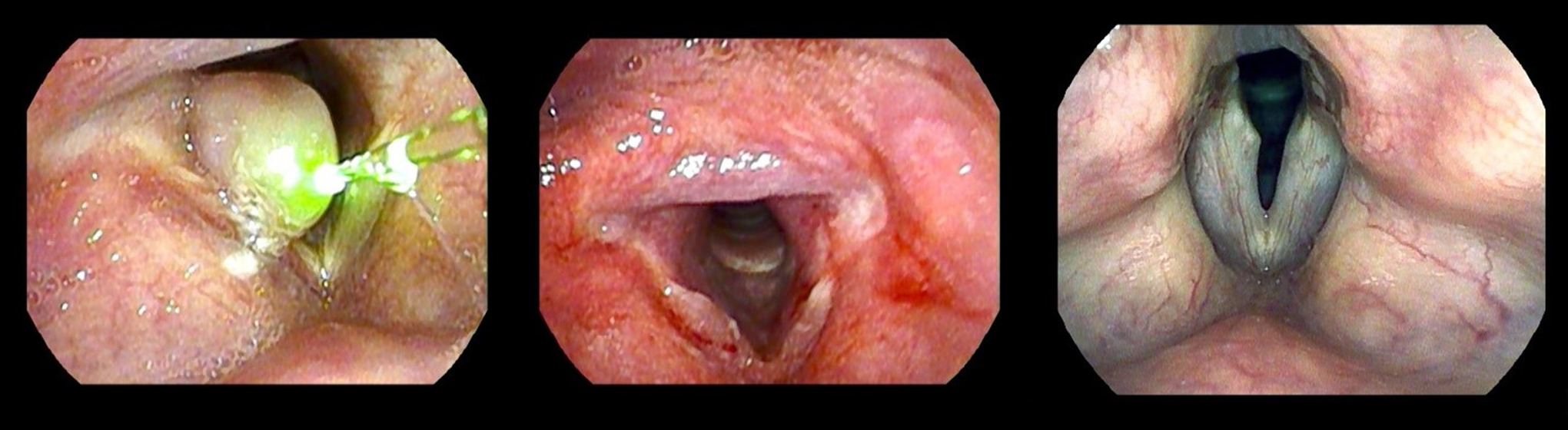
Large right vocal cord granuloma (left). Immediate appearances following blue laser-assisted excision (middle). Two-month postexcision appearances (right).
Methods
We present a retrospective case series of patients who underwent office-based 445 nm blue laser laryngology procedures between January 1, 2018, and July 31, 2020. In addition to recording basic patient demographics and the nature of procedure, we collected data on perioperative nose and throat pain/discomfort scores (0-10, 10 being most severe) and maximum perioperative heart rate and blood pressure. For patients undergoing treatment of RRP or benign laryngeal lesions causing dysphonia, we collected preoperative and postoperative Voice Handicap Index (VHI-10) scores, the latter completed on initial 2- to 6-week follow-up. A paired t test of statistical significance was applied to these data, with a P value of <.05 considered statistically significant. We finally recorded the rate and nature of complications.
This study was registered and conducted in accordance with the ethical regulations of our audit approval body (registration number 11319). Prior to surgery, written informed consent was obtained from all individual participants with no patient identifiable information presented in this article.
Results
Over the specified period, 29 (12 females and 17 males) patients underwent 36 office blue laser TNFLS procedures. Surgery was carried out at 2 institutions by the senior author Y.K., and the case mix is summarized in Figure 6. In all, 48% (14/29) of patients underwent treatment of RRP. Of these patients, 50% (7/14) required repeat procedures within the study time frame. Thirty-one percent (9/29) underwent blue laser treatment of benign lesions, including telangiectasia, contact granuloma, and vocal fold hemorrhagic polyps. Fourteen percent (4/29) of patients underwent laser-assisted diagnostic biopsy procedures for suspected malignancy. Seven percent (2/29) underwent debulking of symptomatic post intensive care unit subglottic and tracheal granulations. One of the patients in this latter group was referred following COVID-19 pneumonitis-related critical illness, and a number of further such cases are pending urgent review.
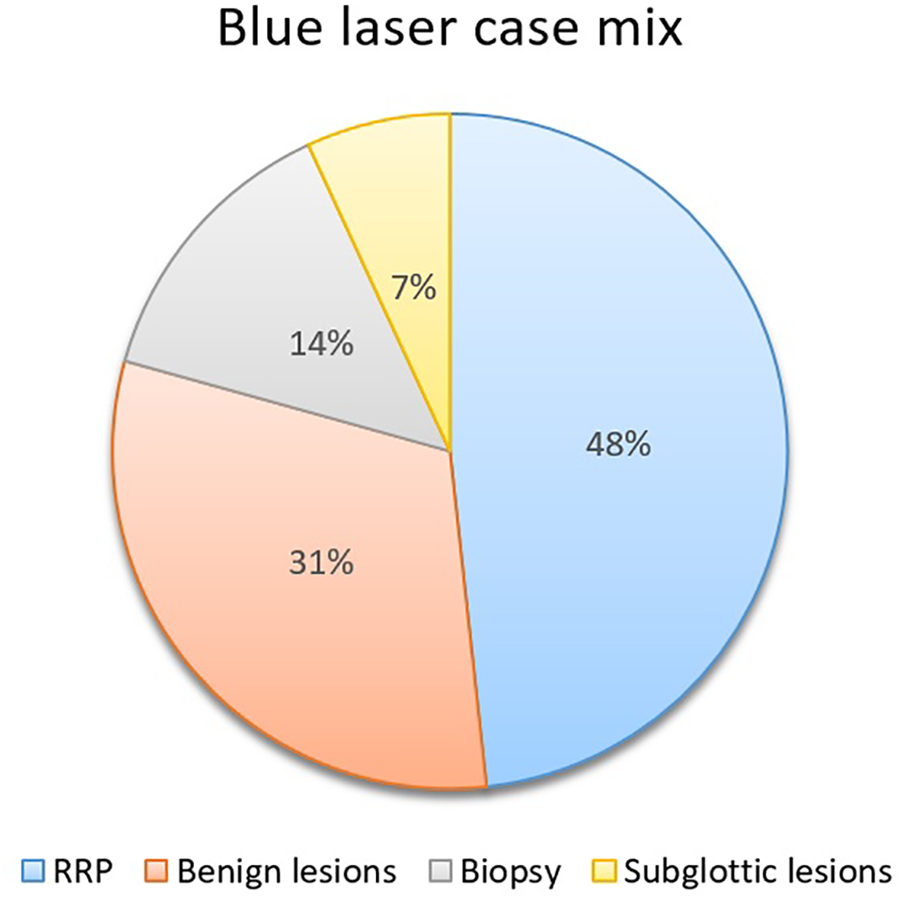
Summary of blue laser case mix.
Patient demographics, pain scores, maximum perioperative blood pressure, heart rate, and complications are summarized in Table 1. The procedure was well tolerated, and in no instances, it was necessary to abandon TNFLS prematurely. Complication rate was low at 3% (1/36), with a single instance of early recurrent vocal cord hemorrhage following treatment of telangiectasia and hemorrhagic polyp. It is unclear whether this complication arose from TNFLS directly, as the affected area was distinct from the operative site. The patient made a complete spontaneous recovery over 2 months.
Patient Demographics and Intraoperative Details.a
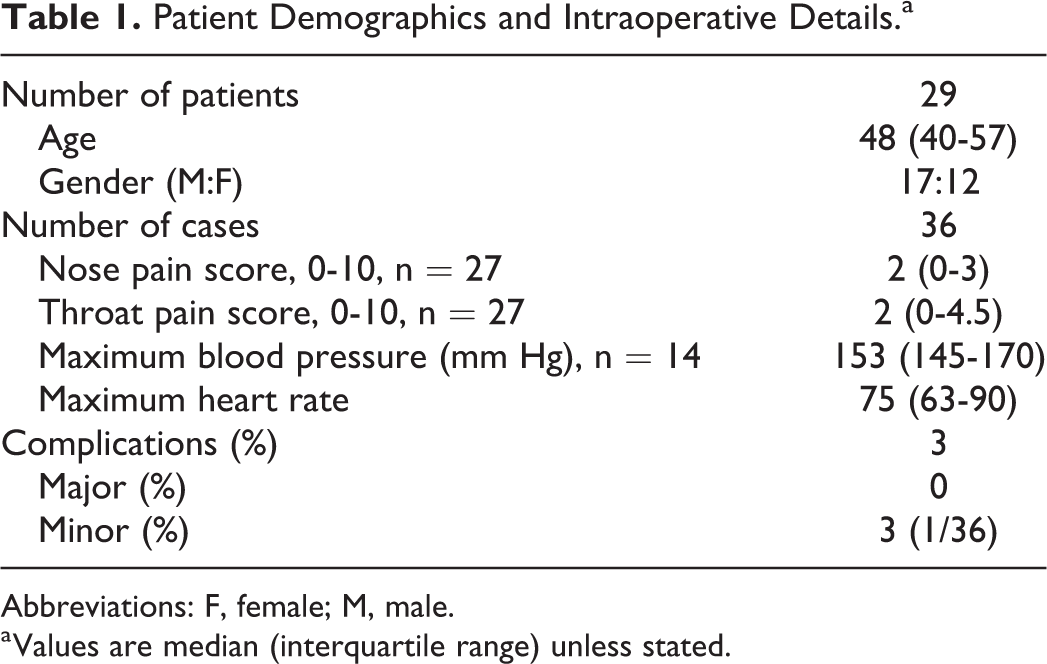
Abbreviations: F, female; M, male.
a Values are median (interquartile range) unless stated.
Pre- and posttreatment VHI-10 scores for RRP and benign lesions are summarized in Table 2; 100% (23/23) of patients undergoing treatment for RRP and benign lesions causing dysphonia reported an improvement in their voice in follow-up clinic, and there was a statistically significant improvement in VHI-10 scores postoperatively, in spite of the limited case numbers. In 100% of patients who underwent diagnostic biopsies (4/4), resultant histology was deemed sufficient to guiding further management.
Preoperative and Postoperative VHI-10 Outcomes of TNFLS in RRP and Benign Glottis Lesions.a
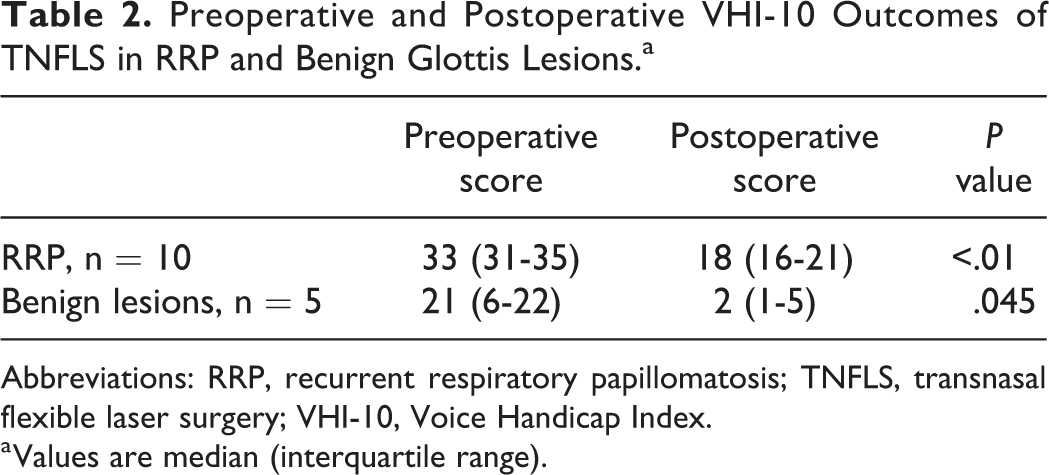
Abbreviations: RRP, recurrent respiratory papillomatosis; TNFLS, transnasal flexible laser surgery; VHI-10, Voice Handicap Index.
a Values are median (interquartile range).
Discussion
Laser surgery of the larynx has revolutionized clinical practice, with CO2 laser delivered via micromanipulator under suspension microlaryngoscopy and general anesthesia now considered the gold standard for many theater-based procedures, attributable to instrument precision, excellent tissue cutting properties, and reduced intraoperative bleeding risk. 21 With the recent development of high-resolution chip-on-tip laryngoscopes with working channels, the role of office TNFLS in RRP and a range of laryngotracheal pathology are now also widely accepted. 22
Established advantages of office TNFLS include avoidance of morbidity associated with (often repeated) general anesthetic, access to areas technically challenging under rigid endoscopy, 23 and significant savings for both institutions and patients. 24 Office TNFLS is well tolerated, 25,26 with low complication rates of 4% to 8% reported, a majority of which are minor and self-limiting. 12,27
At present, photoangiolytic lasers such as KTP and PDL predominate in office-based TNFLS. The selective absorption of these wavelengths by oxyhemoglobin allows for angiolysis of superficial and subepithelial vessels with minimal absorption by surrounding superficial tissues and low bleeding risk. 28 Photoangiolytic lasers enable noncontact laser pulse application via very small glass fibers (300 or 400 nm), which is convenient for office-based procedures. 9 CO2 laser has recently been piloted in office TNFLS, and with its selective absorption by water giving it powerful cutting abilities, this has opened up the possibility of more extensive office-based resection. 23 Limiting factors at present include the cost of custom flexible glass fibers, 29 absence of technology approval in certain regions, 8 and ongoing concern regarding poorer hemostasis in the context of an unprotected airway in the office setting. 30
Hess et al 9 first described the uses and properties of the 445 nm blue laser in 2018. In laboratory studies and general anesthetic case reports, blue laser demonstrated both cutting and photoangiolytic qualities, thus combining key desirable properties of both CO2 and KTP laser. 9 Recent animal-based studies have demonstrated reduced postoperative fibrosis and scarring in blue laser compared with KTP. 10 The device is the size of a shoe box, shock proof, and lightweight (<3 kg), which makes it extremely easy to transfer between office and theater (Figure 7).
Our data present the first systematic report on outcomes of office blue laser TNFLS, strengthening existing experimental evidence that the procedure is safe and effective in the treatment of RRP and benign lesions of the larynx, with a statistically significant difference in preoperative and postoperative VHI-10 scores demonstrated in both conditions.
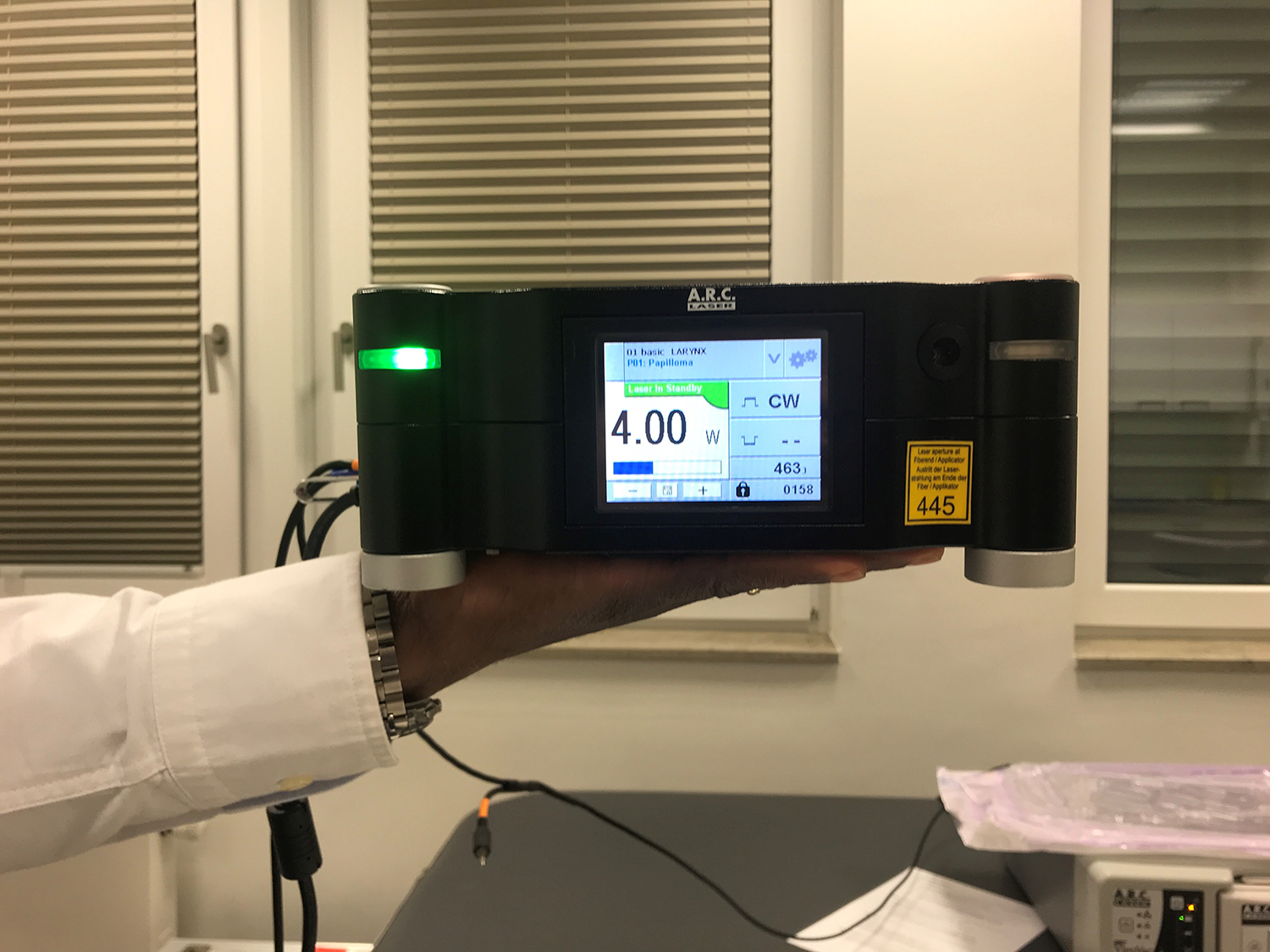
The blue laser is both shock resistant and lightweight.
Limitations
As the first and only case series on office blue laser TNFLS, further research, ideally comparing blue laser with more established office-based lasers such as KTP, will be necessary to corroborate our data and refine our understanding of the technology. The authors are aware of one such ongoing randomized controlled trial. 31
Similarly, to further understand the cutting qualities of blue laser, research comparing efficacy and safety against CO2 laser in the theater-based setting under general anesthesia is required, prior to consideration of any more extensive office-based surgeries in select cases.
Finally, although we have demonstrated efficacy in the treatment of RRP and benign lesions, and in facilitating adequate biopsy, the outcomes of airway granuloma cases remain incomplete and will require further clinical research, including preoperative and postoperative patient-reported outcome measures, such as the Airway-Dyspnea-Voice-Swallow scale. 32
A Note on TNFLS in Addressing the Sequelae of Coronavirus-Related Critical Illness
The authors have observed since June 2020 a dramatic increase in patients presenting with laryngotracheal sequelae of intubation, mechanical ventilation, and tracheostomy, directly attributable to the first wave of the coronavirus pandemic. 33 These have included patients with symptomatic subglottic and tracheal granulations, vocal cord contact granulomas, posterior glottic scars, inflammatory glottic cysts, and bilateral vocal cord immobility. Many such cases will benefit from office- and theater-based laser surgery in the future, and it is now more timely than ever to establish the efficacy, safety, and scope of TNFLS, through meticulous, ethically approved research.
Conclusion
Office blue laser TNFLS is safe and effective in treating a wide range of laryngeal pathologies, with similar treatment outcomes when compared with KTP. Key advantages of blue laser include its portability and its unique combination of photoangiolytic and cutting qualities, although this latter quality requires further demonstration in the theater setting before its potential can be fully realized in the office. Future high-quality research should aim to establish its efficacy and safety in comparison to office-based KTP and theater-based CO2 laser usage.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.