
Abstract
Importance
Phonosurgical treatments with photoangiolytic lasers, including blue light lasers, are increasingly common, yet effects on vocal fold oscillation patterns post-surgery are not fully understood.
Objective
The primary objective was to investigate changing oscillation patterns and recovery time of vocal fold oscillation after blue light laser phonosurgery in patients with unilateral vocal fold pathology.
Design
Prospective observational study following the STROBE guidelines, reporting pre- and post-intervention outcomes.
Setting
The study was conducted in a clinical phonosurgical department specializing in vocal fold pathology.
Participants
Eight patients with unilateral vocal fold pathology were included. Eligibility was determined based on the necessity for phonosurgery.
Intervention or Exposures
Each patient underwent phonosurgical treatment using a blue light laser. Vocal fold function was assessed preoperatively, 2 hours after surgery, 24 hours post-surgery, and 3 weeks following surgery. For the assessment, the subjects phonated on the vowel /i/ at a comfortable pitch and loudness.
Main Outcome Measures
High-speed videolaryngoscopy, electroglottography, and audio recordings were used to assess changes in vocal fold oscillations. Main metrics included amplitude symmetry index, jitter, cepstral peak prominence, and Open Quotients.
Results
Two hours after surgery, an impairment in vocal fold oscillations on the treated side was observed, with a decrease in amplitude symmetry and an increase in electroglottographic jitter. Cepstral peak prominence was reduced, suggesting early effects on vocal fold vibration quality. By 24 hours and 3 weeks post-surgery, most parameters returned to preoperative values. However, the Open Quotient remained lower than pre-surgery levels at the 3-week follow-up, indicating a lasting change in glottal function.
Conclusions
Vocal fold oscillation recovers relatively quickly after blue light laser treatment, generally returning to baseline within 24 hours.
Relevance
This study highlights the temporary nature of vocal fold impairments following blue light laser surgery, providing insights for patient recovery expectations and voice rest recommendations.
Clinical Trial
German Clinical Trials Register, number DRKS00035411 https://www.drks.de/DRKS00035411.
Key Message
Blue light laser phonosurgery causes short-term vocal fold oscillation impairment, with noticeable changes observed 2 hours post-surgery, including reduced amplitude symmetry and vocal quality.
Most vocal function metrics return to baseline within 24 hours, indicating a relatively quick recovery in vocal fold oscillation.
A lasting decrease in Open Quotient at 3 weeks suggests subtle long-term changes, which may inform post-surgical voice management and patient counseling.
Introduction
Vocal fold oscillations are considered a crucial factor for the production of the voice source, that is, the sound produced at the glottis, which later will be modified by vocal tract resonances.1 -3 In this respect, it has been shown that the oscillatory amplitude is increased for a rise of the sound pressure level (SPL) or loudness,4,5 and that the number of oscillations determines the number of air pulses that defines the fundamental frequency (ƒo).1 -3 Such dependencies vary with respect to vocal fold thickness. 6 Furthermore, the closing of vocal folds during the glottal cycle determines the Maximum Area Declination Rate which—besides the transglottic pressure difference and vocal tract/voice source interactions—has a strong effect on the Maximum Flow Declination Rate and on the peak closing of the oscillatory amplitude relative to length. 4 Both are not only relevant for the regulation of the SPL but also for intensities of overtone structures of the voice source.1,7
Impairment of vocal fold oscillations can result in dysphonia. 8 This might be related to vocal fold mass lesions, problems in the regulation of vocal fold stiffness due to muscle tension and/or vocal fold adduction, or changes of morphology. Also, the entrainment of both vocal fold oscillatory systems 9 may play an important role with respect to voice source generation and, consequently, dysphonia.
Besides the classical treatment of vocal fold lesions using phonomicrosurgery under general anesthesia, or removal under local anesthesia, there is a rise in doctor’s office-based surgeries using photoangiolytic lasers, mostly under local anesthesia. First, potassium-titanyl-phosphate (KTP) lasers have been used with a wavelength of 532 nm. More recently, blue light lasers, such as TruBlue lasers, have been introduced to the market. In contrast to KTP, the laser spectrum is altered to 445 nm. Such lasers focus on the absorption of energy by hemoglobin. The outcome of a blue laser treatment is dependent on many factors, such as fiber to epithelium distance, pulse width, and energy levels.10,11 In contrast to CO2 lasers, photoangiolytic lasers exhibit less thermal expansion and incision depth 12 in model experiments. Although the effect on hemoglobin could also potentially induce necrosis with a consecutive effect on the different layers, to the best of the authors’ knowledge, this has not yet been documented in the literature for photoangiolytic treatments. Such photoangiolytic lasers have been used for the treatment of vascular vocal fold lesions, such as ectasis, papillomatosis, other premalignant or malignant lesions,13 -16 and non-vascular vocal fold lesions, such as scar, laryngeal stenosis, laryngeal web, or Reinke’s edema.17 -21 The safety of blue light lasers is comparable to other surgical modalities. 17 Furthermore, it has been found that the use of blue lasers results in lower rates of early postoperative hemorrhage and revision surgery. 17 In comparison to KTP, treatment with blue lasers resulted in lower severity of postoperative edemas and hemorrhages in vascularized mass lesions, 13 as well as significantly lower degrees of scarring of the vocal fold tissue. 22
After surgery using cold instruments, it is considered that wound healing starts to take place immediately after the damage. 23 In particular, the components of protein and proteoglycan synthesis, as well as wound contraction, can last for weeks or months. 23 The wound healing is dependent on the extent and depth of damage. 24 Therefore, vocal fold oscillations are impaired immediately after surgery. It is a matter of discussion whether there should be vocal rest, use of a relaxed voice with low loudness and pitch, or use of a normal voice during the wound healing process.24,25 Furthermore, the length of time for this healing process is also under discussion.26,27
In contrast to the removal of mass lesions, the use of photoangiolytic lasers only has an effect on hemoglobin and in cases where no contact of the laser to the epithelium is present, there should be no damage to the epithelium. Even in cases where there could be heat due to direct contact with the epithelium, the trauma of the vocal fold layer structure could be less in comparison to phonomicrosurgery, due to the superficial effect. 12 However, the vocal fold oscillatory characteristics after photoangiolytic surgery are not known.
This study analyses vocal fold oscillatory characteristics in the short time domain after unilateral photoangiolytic surgical intervention using the blue light laser. Vocal outcome was characterized by measures reflecting oscillation characteristics such as Open Quotients, symmetry (amplitude symmetry index and phonovibrograms) and periodicity by means of the cepstral peak prominence (CPP). It is hypothesized that, immediately after intervention, the oscillatory component is diminished but shows an early recovery.
Material and Methods
After obtaining approval from the Medical Ethics Committee of the University of Munich (Nr.18/769) and the Freiburg University Ethical Committee (number 380/12), 10 patients, initially, who gave their informed written consent were enrolled in the study. For the diagnosis of leukoplakia and papillomatosis before an office-based blue light laser treatment, there was a biopsy under general anesthesia for the respective subjects. Only unilateral mass lesions were included in the study to offer a comparison to a healthy vocal fold. From the initially included 10 patients, two had to be excluded due to unexpected bilateral surgery. Table 1 displays the clinical diagnosis, age, and treatment dosage for the remaining 8 patients. The surgeries were executed by a single experienced phono-surgeon. The HSV recordings and data processing were performed by different investigators, the latter blinded to the clinical case.
The Patients Age, Treatment Dosage, and Clinical Diagnosis.

Surgery
All patients underwent surgical treatment using the TruBlue blue light laser (A.R.C. lasers, Nuremberg, Germany). Vocal fold images of all patients before surgery, 24 hours after surgery, and 3 weeks after surgery are shown in Figure 1. Prior to surgery, local nasal and oral anesthesia was administered using lidocaine (Xylocain©, AstraZeneca, Germany) spray. The laser fiber was inserted transnasally into the flexible chip-on-the-tip endoscope (Olympus ENF, CV190, Hamburg, Germany) with close contact between the two. The surgical success was shown by the blanching/destruction of the mass lesion. Due to differences of the fiber-to-tissue distances, there were variances of the total energy applied, Table 1. All surgical procedures took less than 10 minutes. Following surgery, patients were advised to rest their voices for the first 2 hours, and, subsequently, to use their voices only if necessary and at reduced loudness and pitch for at least 24 hours after surgery. As an instruction the patients were recommended to speak in “a bored manner with the aim that the listener could fall asleep.”
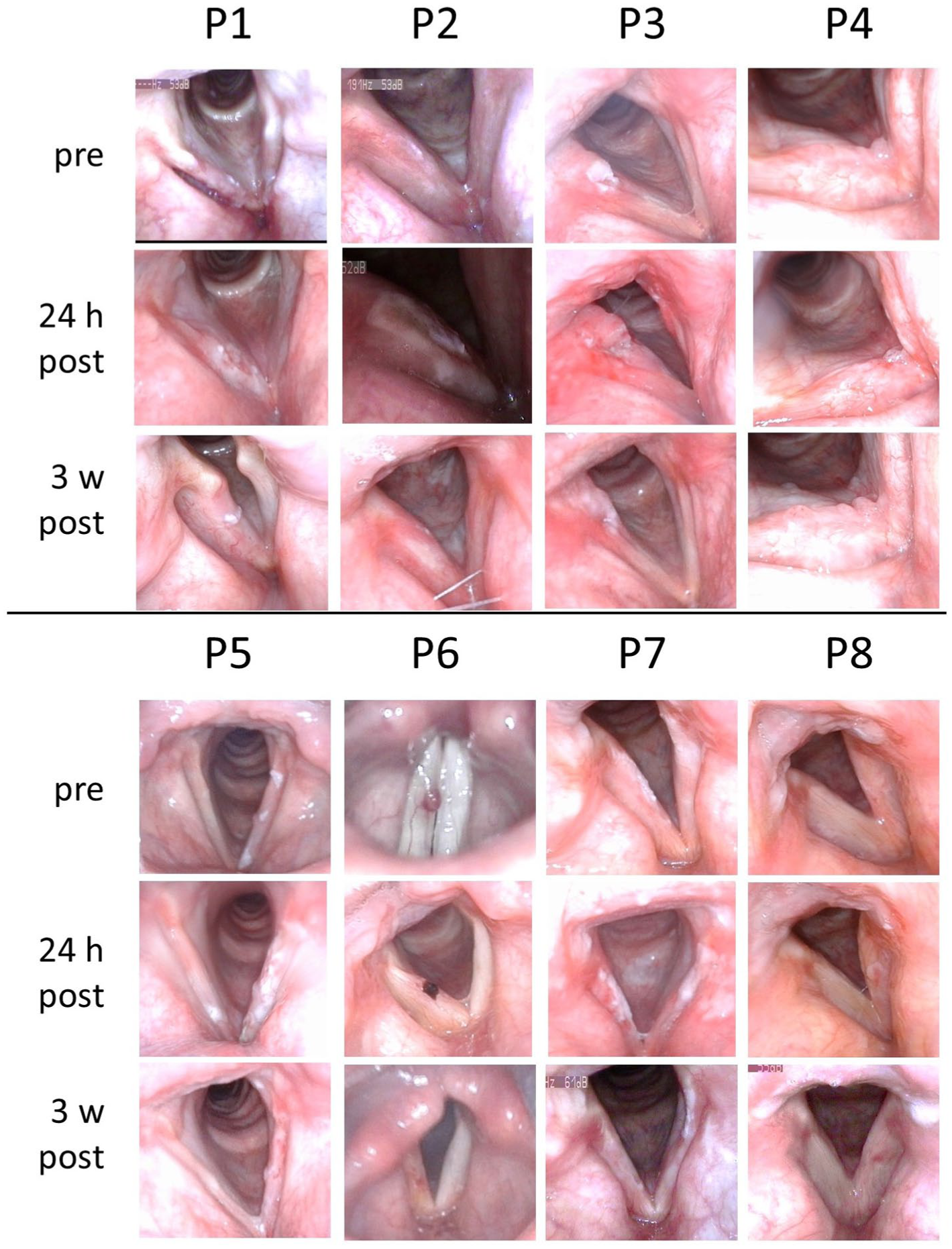
Preoperative, 24-hour-postoperative, and 3-week-postoperative images.
Task and Recordings
Four recordings were made: one before surgery, and one each at 2 hours, 24 hours (±2 hours), and 3 weeks after surgery. Although wound healing with associated migration of neutrophils could have a later peak after surgical tissue injury, the time interval of 24 hours was chosen since it lies within the time frame for recommended voice rest and was used to evaluate the vocal folds at a time when near maximal surgical trauma and post-inflammatory effects would be expected. The final recording took place 3 weeks after surgery because—as pointed out in the introduction—Blue Laser treatment is associated with a shorter time interval for wound healing. For the recordings, all patients phonated on the vowel /i/ at a comfortable pitch and loudness. During the phonation, analogous to previous research,28 -31 the patients were recorded using transnasal high-speed-videolaryngoscopy (HSV), electroglottography (EGG), and acoustic recording simultaneously. HSV recordings were performed using transnasal endoscopy with a Fastcam SA-X2 (Photron, Tokyo, Japan) and a flexible endoscope (ENF GP; Fa. Olympus, Hamburg, Germany) at a frame rate of 20,000 fps and a spatial resolution of 386 × 320 pixels. Audio signals were recorded with a DPA IMK SC 4061 (DPA microphones, Alleroed, Denmark), and EGG signals were captured with an EG2-PCX2 from Glottal Enterprises (Syracuse, NY, USA). No anesthetic medication was applied during the experiment. The HSV videos were post-processed by means of rotation, Fast-Fourier-Treatment, and cropping, as described previously.29,30 The calculation of the glottal area waveform (GAW) and phonovibrograms (PVG) from the HSV images was performed based on Lohscheller et al. 32
Measures
The Glottal Analysis Tools program 33 was used to segment the HSV data, estimating the time-varying lateral deflection of the vocal fold edges along the anterior-posterior glottal dimension. 34 From the GAW and PVG, as well as the electroglottographical and audio signals, the parameters introduced below were calculated using the Multi Signal Analyzer (Division of Phoniatrics, University Hospital Erlangen, Erlangen, Germany). 35 For the detection of the GAW’s Open Quotient (OQGAW), a tolerance threshold of 5% was chosen. Consequently, all GAW values greater than 5% from baseline (ie, pixel number of the fully open glottis) were considered to indicate an open glottis, while GAW ≤5% indicated a closed glottis. The amplitude symmetry index (ASI) serves as a side-independent measure for vocal fold oscillation symmetry, with values ranging mostly between 1 (full symmetry) and 0 (one vocal fold without movement), being calculated from the size ratio of the halves of the maximum glottal area. The glottis gap index (GGI) indicates if a gap remains during the actual closed phase of the glottis. The EGG Open Quotient (OQEGG = Contact QuotientEGG − 1) was calculated according to the method proposed by Howard. 36 The ƒo was calculated from the EGG signal. From the audio signal, the SPL, indicated in dB(A), was estimated after calibration with a sound level meter (Tecpel 331, Taipei, Taiwan) using the Sopran software (Svante Granqvist, Karolinska, Stockholm, Sweden). Although the jitter could be, in general, considered problematic for the detection of a vocal outcome after treatment, 37 it was assumed that this measure could be used in order to reflect type 1 versus type 2 or type 3 voice signals according to Titze. 38 Thus, it was calculated from all three signals as a mechanical perturbation measure. In order to account for potentially non-quasi-periodic signals (ie, type 2 and type 3 signals), the CPP 39 was calculated for all three voice signals.
Statistical Evaluation
Due to the small sample size, comparative statistics were considered problematic and results are presented in boxplots as descriptive statistics.
Results
There were no surgery-related complications during the experiment. As shown in Figure 1, treatment was a success for most of the surgical interventions. In subject P4, however, there was a recurrence of the papillomatosis 3 weeks after surgery. Because this could influence the outcomes, especially regarding the 3-week measurement, separate data of P4 and the remaining subjects are provided in the Supplemental Material. Aside from that, subject P5 exhibited a pronounced effect from the blue laser treatment. However, there was blanching 2 hours after surgery, followed by a subepithelial hemorrhage 24 hours after surgery. After 3 weeks, no mass lesion was present anymore.
There was a slight decrease of both, SPL and fo 2 hour-postoperatively (Figure 2). After 24 hours and 3 weeks, however, the values were in the range of the presurgical evaluation.

Sound pressure level (SPL) and fundamental frequency (fo) of all participants for all time-points.
Both OQGAW and OQEGG were decreased 2 hours after surgery and remained lower than the presurgical value, also 24 hours and 3 weeks after surgery (Figure 3).

Open Quotients (OQ) from electroglottography (EGG) and glottal area waveform (GAW) of all participants for all time-points.
Also, 2 hour-postoperatively, there was a rise in the jitter of audio and EGG signals. For these parameters, there was a tendency for change in direction to the presurgical values already 24 hour-postoperatively. After 3 weeks, there was no great difference compared to the presurgical values anymore (Figure 4). This agreed with the CPP values of audio and EGG signals, which showed an improvement after 3 weeks. The jitter and CPP of the GAW did not show strong changes over the observed period.

Boxplots of jitter and cepstral peak prominence (CPP) of audio, electroglottography (EGG), and glottal area waveform (GAW) of all patients for all time-points.
The GGI was changed for only 2 subjects by a very small amount (Figure 5).

GGI and ASI of all participants for all time-points. Note regarding GGI that, except for P2 and P4, all participants stay close to or on zero and are therefore not labeled. GGI, glottis gap index; ASI, amplitude symmetry index.
The ASI values were around 0.8 in pre and 3-week-postoperative measurements, where a value of 1 would mean a completely symmetrical oscillation. Concerning the side differences of treated versus untreated vocal fold, both the PVGs and ASI indicate that there were impairments of oscillation 2 hour-post-surgery (Figures 5 and 6). Remarkably, only 2 subjects (P2, P4) showed major impairments. At 24 hours post-surgery, oscillatory movement was already close to the untreated side.
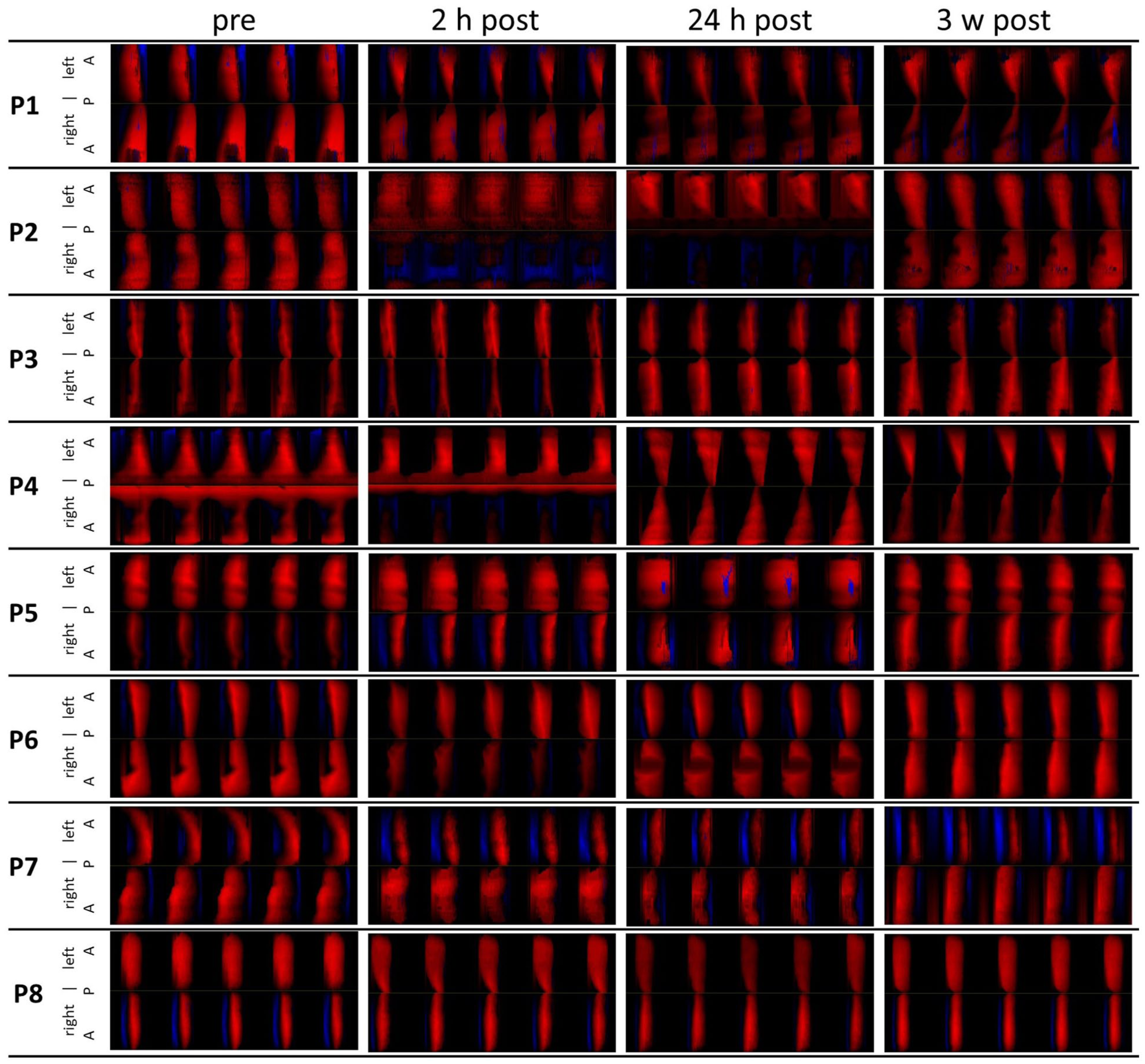
Phonovibrograms of 5 glottal cycles of each patient from each time-point.
Discussion
This investigation analyses the changes of vocal fold oscillation patterns over the short time span of 3 weeks after surgical intervention with a photoangiolytic blue light laser. In general, vocal fold oscillation turned out to recover early after such interventions, that is, within 24 hours after surgery.
Vocal fold oscillation is a crucial factor for voice production; its impairment is frequently associated with dysphonia. After phonomicrosurgery, some surgeons recommend vocal rest in order to avoid compromising wound healing, and the growth of scar tissue. However, as pointed out in the introduction, both the general need for vocal rest and the duration of said rest are under discussion. In contrast to classical surgical techniques, such as cold steel or CO2-lasers, it could be expected that photoangiolytic lasers, such as the blue light laser, might have a smaller influence on oscillation patterns due to the small depth and, in cases of close but not direct contact, maintenance of an intact epithelium. The data presented in this study match this hypothesis. Interestingly, directly after intervention, that is, 2-hour-post, there was a strong impairment on the surgically treated vocal fold observed in two of the patients. The reason for this impairment remains unclear. The doses for both subjects were in the mid-range, as shown in Table 1. However, it should be kept in mind that the dose specified does not reflect the tissue dose, which is also dependent on the distance of the laser fiber to the tissue. Furthermore, subject P4 had a papillomatosis. It is possible that stiffness due to blue laser treatment could be different depending on the type of pathology. However, small impairments of the oscillatory characteristics were also observed for the other subjects. This might be a direct effect of the treatment. Due to the laser characteristics, the energy of the laser is absorbed primarily by hemoglobin. One effect is a thrombosis of the treated vessels, visible by the whitening effect (blanching) on the vocal folds. Another effect could be the emergence of some heat due to the energy transfer in this region. Both could produce some tissue stiffness diminishing vocal fold oscillation.
Concerning the periodicity of vocal fold oscillations, there were contradictory data with respect to the EGG and GAW signals. The observed rise of EGG-derived jitter and lowering of the CPP could well be associated with the structural and functional changes of the oscillation following blue laser treatment. With this in mind, it could be hypothesized that the entrainment of both vocal folds’ oscillations might be altered, influencing stability. However, the jitter and CPP of the GAW were almost unchanged. It should be noted here that the 2 signals represent different aspects. While the EGG signal measures impedance changes of the three-dimensional oscillatory process, laryngoscopic images represent the waveform of a two-dimensional view of the glottis from above. Furthermore, it has been shown that the one-dimensional GAW alone is not sufficient to differentiate between healthy or dysphonic voices. 40 With respect to the GAW-derived CPP, it could be interpreted that periodicity is not significantly influenced. In this respect, the CPP values were generally above reported dysphonia cutoff values, 39 hinting at the generally good coping with the organic conditions and/or influences of blue light laser treatment by the patients.
Furthermore, the patients already showed rather good presurgical left-right symmetry of vocal fold oscillations. However, it remains unclear why, 3-weeks-postoperatively, the oscillation amplitude symmetry is only back at the presurgical level without a further rise of the ASI, despite the lesions having been removed. Regarding the OQs, it must be mentioned that in most subjects the pre-values were located in the region of 0.5 to 0.6, which indicates that the mass lesions did not mechanically impair the oscillation to a great amount. This might explain why the improvement after 3 weeks does not go beyond the pre-values. In addition, previous studies have shown that changes of OQGAW might be small. In a study on varying loudness in patients with vocal fold mass lesions, the median difference between lowest and highest irregularity—as measured by the sample entropy—was only in the range of 0.1. 31 In another study applying a vocal loading of 10 minutes phonation above 80 dB measured at 30 cm from the mouth, the median difference of OQGAW was also lower than 0.1, thus failing statistical significance in the pre/post comparison. 41 Also in this context, subject P4 exhibited a papilloma recurrence in the 3 weeks measurement. However, as can be seen in the Supplemental Material, the values for most measures do not differ by a great amount from the other subjects. Because the oscillation patterns in the phonovibrograms were not impaired by a detectable organic reason, it could also be speculated that the unchanged central nervous regulation might be a cause for the lack of improvement. If so, it should be analyzed in future studies if voice therapy would be able to further improve vocal oscillation symmetry. Generally, it must be emphasized that this study considers the recovery of vocal fold oscillation after blue light laser treatment and not necessarily dysphonia development before and after treatment. It is recommended to include much more voice-related outcome measures for future investigations of blue light laser treatments.
Twenty-four hours after surgery, almost all measured parameters were close to the preoperative data. Although a recommendation of vocal rest could be meaningful in the first 24 hours after surgery, such rest appears not to be sufficiently reasonable afterwards. However, voice rest recommendations should not only be made based on these empirical measurements, but also consider relevant individual factors such as profession, possibilities of voice abstinence, habits, psyche, compliance, etc.
Furthermore, it has to be noted that the wound healing processes after blue light laser treatment have, to the best of our knowledge, not yet been addressed on a molecular level. Thus, it is unclarified if there is any further risk to the tissue, despite the restoration of oscillation after this time interval.
Limitations
There are a number of further potential limitations associated with this study.
First, due to the extensive analysis method, only a very small number of subjects could be included. A higher number of subjects could reveal statistically meaningful data. Furthermore, the patients included suffered from different entities of vocal fold mass lesions and extents. It seems reasonable to believe that larger mass lesions and stronger vascular lesions might show stronger impairment of vocal fold oscillations. Also in this context, there was a variance of total energy exposure during the treatment. This was presumably mainly caused by differences in the fiber-to-tissue distances. It has been shown before that a larger distance is associated with a higher total energy. 11 Unfortunately, such exact distance can only be measured by laser triangulation, not yet permitted for clinical use. The analysis of the distance’s effect on the outcome measures remains open for future investigations. Furthermore, the presented data were related to phonation in comfortable pitch and loudness. However, it cannot be excluded that there would be a variance for standardized pitch and loudness. Also in this context, the data refer to the /i/ vowel, which is associated with a relatively upright epiglottis and the best visibility of the vocal folds. Due to vowel-dependent vocal tract/voice source interactions, 28 other vowels might show different results. Furthermore, the application of transnasal laryngoscopy could have influenced the participants’ phonation. In particular, the endoscope could have opened the velopharyngeal port, which could have a stabilizing effect on vocal fold oscillation patterns, as has been shown regarding the tenors passaggio. 42 However, because the treatment and changes in stiffness should affect only the vocal fold, such an error should be considered as systematic. Furthermore, the test subjects were instructed for reduced vocal use with a reduced vocal dose for the time span of 2 to 24 hours after surgery. In contrast to the first 2 hours after surgery, where the patients completely rested their voices on-site, there was no chance of checking the compliance afterwards. Therefore, it cannot be excluded that the speaking practice differed among subjects. For the reevaluation, the time interval of 24 hours after surgery was chosen due to the time interval for the usual recommendation of voice reduction. However, it cannot be excluded that the peak of inflammatory effects occurs later than this time interval. Thus, in future studies, different time intervals should be tested. Also, the estimation of vocal fold amplitudes is limited, since laser-triangulation for absolute distance values was not applicable 43 and values for distances depend on the angle of the endoscope. Although it was attempted to provide constant conditions, there could be small differences between the endoscopies. Finally, it must be pointed out that this study only focuses on the basic oscillation ability of the vocal folds and not multidimensional voice evaluation.37,44 Such studies should be performed in future with much larger collectives of patients.
Conclusions
Phonosurgical treatments using the blue light laser result in impairments of vocal fold oscillations for a brief time interval, with recovery to a large extent seen within 24 hours of surgery. Therefore, extensive vocal rest, or reduction of vocal dose, should be recommended for the first hours after surgery, but not necessarily for 24 hours after surgery while taking into account other factors relevant for voice recovery.
Supplemental Material
sj-pdf-1-ohn-10.1177_19160216251409743 – Supplemental material for Vocal Folds’ Oscillatory Characteristics After Photoangiolytic Laser Treatment Using the Blue Light Laser—A Pilot Study
Supplemental material, sj-pdf-1-ohn-10.1177_19160216251409743 for Vocal Folds’ Oscillatory Characteristics After Photoangiolytic Laser Treatment Using the Blue Light Laser—A Pilot Study by Matthias Echternach, Michael Döllinger, Bernhard Richter and Marie Köberlein in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Acknowledgements
We would like to thank Kevin Gagnon for his assistance with the English language and for proofreading the manuscript.
Author Contributions
ME: Conceptualization, Funding acquisition, Investigation, Writing—original draft. MD: Methodology, Software, Writing—review & editing. BR: Conceptualization, Funding acquisition, Writing—review & editing. MK: Formal Analysis, Data curation, Visualization, Writing—original draft.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Matthias Echternach’s work (DFG, grant 409/1-4 and Ec409/5-1) and Michael Döllinger’s contributions (DFG, grant DO1247/21-1) were supported by Deutsche Forschungsgemeinschaft.
Ethical Considerations
Medical Ethics Committee of the University of Munich (Nr.18/769) and Freiburg University Ethical Committee (number 380/12).
Consent to Participate
Informed written consent was given by all participants.
Consent for Publication
Informed written consent was given by all participants.
Data Availability Statement
Data sets generated during the presented study are available from the corresponding author on reasonable request.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.