
Abstract
Introduction
Descending necrotizing mediastinitis (DNM) is a localized infection with odontogenic, otolaryngological, or parapharyngeal origin that spreads into the deep neck, descending along the parapharyngeal, carotid, prevertebral, or pretracheal space and further into the mediastinum.1,2 Owing to the proximity of the neck to vital structures, DNM is a highly morbid pathological process associated with a mortality rate of 16.5% to 74%.3,4 This disease can occur at any age, but the incidence rate increases and the prognosis worsens with increasing age.4,5 The main causes of DNM are odontogenic, pharyngeal, and other cervicofacial infections.6,7 The most effective diagnostic modality is computed tomography (CT) with contrast enhancement of the cervical and thoracic regions, which has 64% to 100% sensitivity and 45% to 82% specificity.8,9 Accurate imaging results can guide surgery and antibiotic use, as well as the evaluation of treatment outcomes. 10
DNM treatment requires a multidisciplinary approach, with concurrent surgical drainage of the abscess and antibiotic therapy required. 11 However, the optimal surgical route is still debated. Some clinicians favor transcervical incision combined with mediastinal drainage, with or without a transthoracic approach, whereas others prefer a transthoracic approach that includes percutaneous thoracostomy, thoracotomy, and thoracoscopic surgery, as well as video-assisted thoracic surgery (VATS).3,12 Further, few studies have analyzed the risk factors of mortality in DNM. Thus, this study aimed to clarify the risk factors and some clinical characteristics of mortality of DNM in our hospital.
Methods
The related general condition and common comorbidities of patients diagnosed with DNM between January 2008 and October 2022 at the West China Hospital of Sichuan University were evaluated [2022 (#1530)]. Since this was a retrospective data study, a waiver of informed consent was obtained.
The diagnostic criteria 13 for DNM were as follows: (1) severe cervical infection, (2) characteristic mediastinitis features on CT, (3) necrotizing mediastinal infection intraoperatively, and (4) an established relationship between oropharyngeal or neck infection and development of DNM. The exclusion criteria were (1) malignant tumors, (2) hematological diseases, and (3) a history of surgery or incision drainage for this infection in an external hospital. Baseline patient characteristics including age, Gender, body mass index (BMI), disease course, medical history, and common comorbidities were investigated.
Laboratory tests and CT were performed upon admission. Venous blood was drawn to measure inflammatory markers, such as white blood cell (WBC) count, neutrophil percentage, and C-reactive protein (CRP), as well as protein content, electrolytes, and other relevant parameters. The patients underwent contrast-enhanced CT scans, but those with renal failure and iodine allergy underwent conventional CT. The diagnosis was established based on CT findings and inflammatory markers. The degree of DNM diffusion was evaluated based on CT findings following the classification proposed by Endo et al 14 : type I, infection localized in the upper mediastinum above the carina; type IIA, infection extended to the lower anterior mediastinum; and type IIB, infection extended to the lower anterior and posterior portions of the mediastinum.
All patients underwent surgery on the day of admission. Surgical management consisted of cervical and mediastinal drainage performed either by a single ear, nose, and throat (ENT) surgeon or by ENT and thoracic surgeons. The surgical approach was individualized according to the preoperative Endo classification, with surgeons ensuring that each pus cavity was fully drained and that the necrotic tissue was sufficiently removed. Neck surgeries were primarily performed through a longitudinal incision at the anterior edge of the sternocleidomastoid muscle. Pus drainage and debridement of necrotic infected tissue of the anterior superior mediastinum were performed, as needed, through the neck incision. There were 3 options for mediastinal drainage, namely, transcervical mediastinum, VATS, and thoracotomy. Negative-pressure drainage was placed in all cervical and mediastinal abscess lacunae, and the incisions were closed using primary sutures.
Each abscess cavity was fitted with at least 2 thick drainage tubes. Unless irrigated, the tubes were connected to a negative-pressure drainage bottle for continuous drainage. During irrigation, one tube served as the inlet, and the other served as the outlet. Negative-pressure suction was applied for more than 24 hours until the pus was fully drained and cleaned, and daily iodophor disinfection and physiological saline flushing were performed. Tracheotomy was performed in the emergency operating room for patients with respiratory obstruction upon admission and at the intensive care unit (ICU) bedside for those without short-term tube drawing. Intraoperatively, pus and necrotic tissue samples were collected for bacterial culture. All the patients were treated with systemic intravenous antibiotics consisting of piperacillin sodium and tazobactam or sulbactam and metronidazole. Antibiotic use was adjusted based on pus, sputum, and blood cultures, as well as based on the attending physician’s preference. Postoperatively, regular enhanced CT or magnetic resonance imaging of the neck and chest was performed to assess recovery of the pus cavity. Repeated drainage and reoperation were performed for serious infections given the progressive nature of DNM.
Data on complications requiring hospital admission, duration of hospitalization, length of ICU stay, and mortality rate were collected. The collected data were transferred to standard spreadsheets and statistically analyzed using SPSS software (version 22.0; IBM SPSS, Armonk, NY, USA). Data are expressed as the mean ± standard deviation for continuous normally distributed variables or as percentages for categorical variables. Categorical data were compared using Fisher’s exact test or the chi-squared test for more than 2 variables. Continuous variables were compared using Student’s t-test for independent samples. Categorical variables were evaluated using the χ2 test or Fisher’s exact test, as appropriate, and Pearson’s product–moment correlation coefficient. Univariate analysis using a stepwise method and binary logistic regression were performed to identify significant variables. The significant variables were then subjected to multivariate analysis to determine independent predictors of mortality. All tests were 2 tailed, and P < .05 was considered significant.
Results
Overall, 181 patients with a mean (SD) age of 52.08 ± 16.67 years (range, 8 months-84 years) were evaluated. The mortality rate was 21.55% (39/181). A comparison of patient characteristics between those who died and survived is shown in Table 1. The patients who died were older than those who survived (P = .007). Gender, BMI, disease course, hypertension, diabetes, and immune system diseases were not significantly associated with death (Table 1). Five main pathogeneses were identified: odontogenic infection (exocytosis and rotten teeth), pharyngolaryngeal infection (peritonsillar abscess, tonsillitis, and epiglottitis), foreign bodies in the throat and esophageal inlet, congenital malformations (pyriform sinus fistula and branchial cleft anomalies), and maxillofacial trauma and infection. Odontogenic and pharyngolaryngeal infections were the primary pathogenic mechanisms; however, no correlation was found between this pathogenesis and death.
Patient Characteristics.
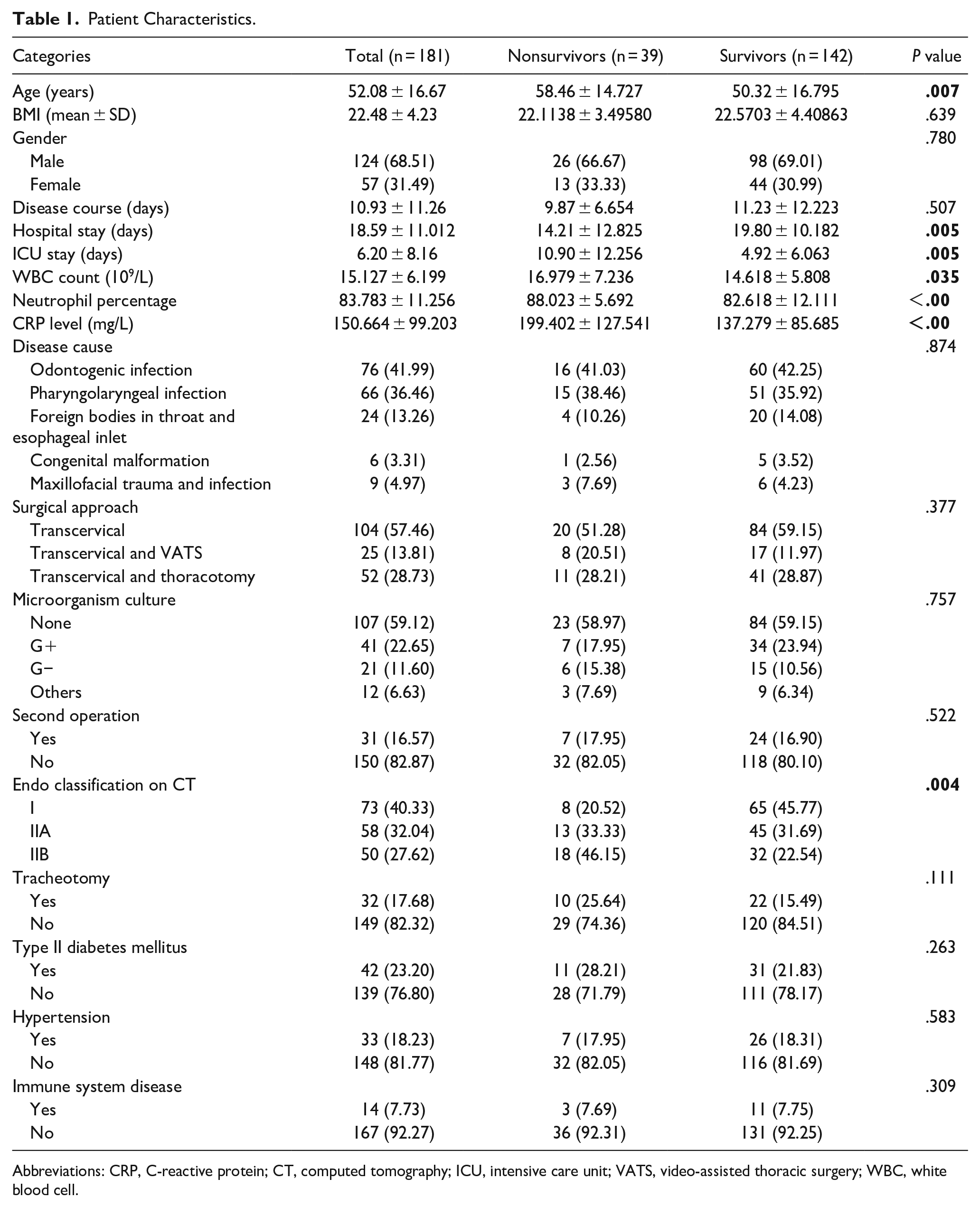
Abbreviations: CRP, C-reactive protein; CT, computed tomography; ICU, intensive care unit; VATS, video-assisted thoracic surgery; WBC, white blood cell.
The WBC count, neutrophil percentage, and CRP levels at admission were significantly higher in the patients who died. The mortality rate was higher in patients with Endo type IIB disease than in those with Endo types I and IIA. The mortality rate was also higher in patients with Endo type IIA disease than in those with Endo type I disease. Three types of surgery were performed: transcervical drainage (57.46%), transcervical drainage with VATS (13.81%), and transcervical drainage with thoracotomy (28.73%). Overall, 28 patients (15.47%, 28/181) underwent a second surgery to drain the pus cavity. In total, 3 patients (1.66%, 3/181) underwent a second surgery with hemostasis for postoperative bleeding. The survival rates were not significantly different between patients who underwent 1 operation and 2 operations or tracheotomy.
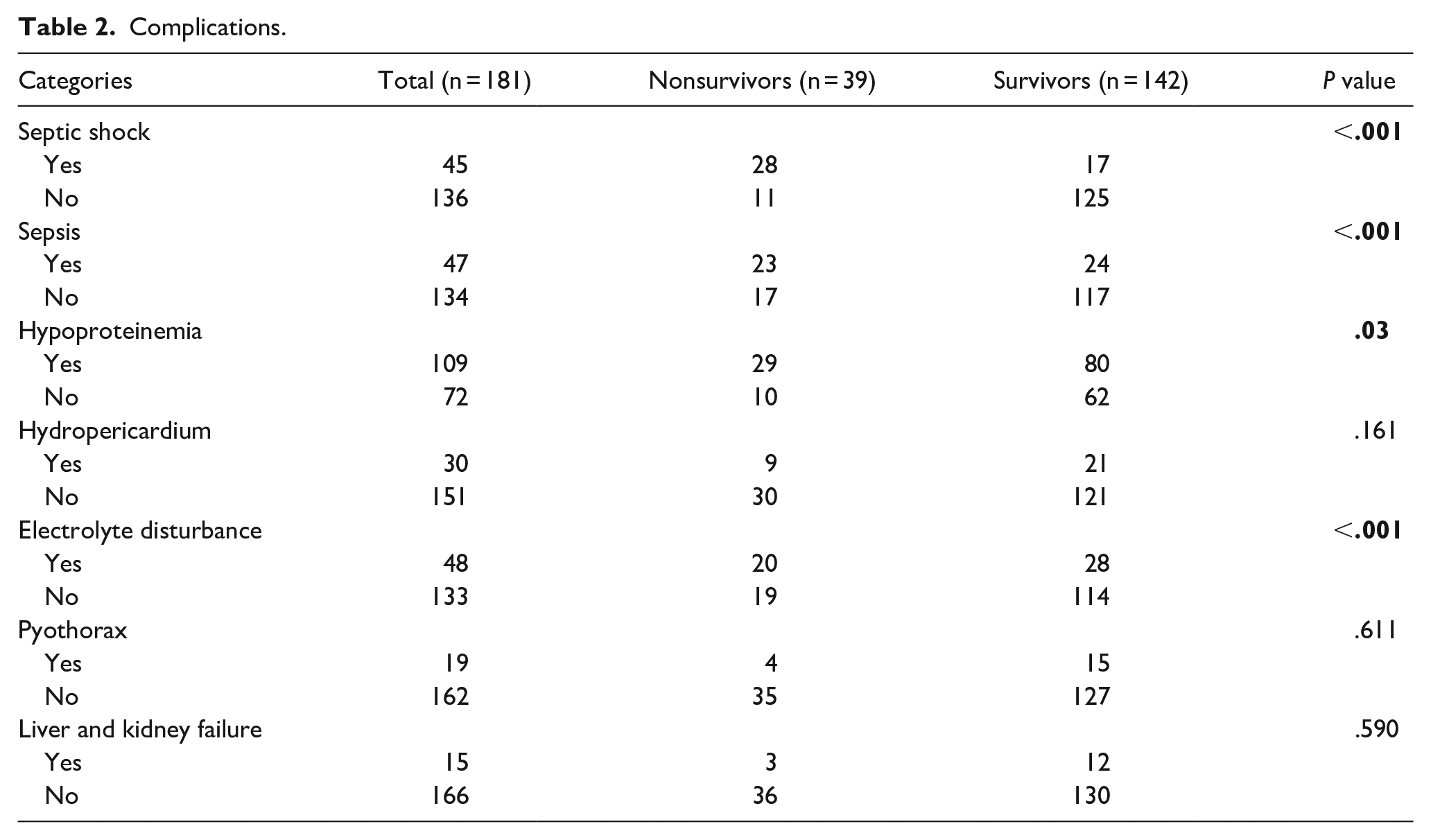
Microorganisms were detected in only 74 (40.88%) of the 181 pus specimens, and 19 (25.68%) patients had 2 or more types of bacterial infections. The most common pathogenic strain in the entire cohort was Gram-positive (G+) (41 patients), but no anaerobic bacteria or fungi were identified. Patients with septic shock, sepsis, hypoalbuminemia, or electrolyte disorders had significantly higher mortality rates than did survivors (Table 2). Age (≥55 years old), Endo classification type IIB on CT, septic shock, and CRP level at admission independently increased the risk of mortality. The risk of mortality increased 2.208 times each year (Table 3).
Complications.
Multivariate Binary Logistic Regression Analysis of the Independent Risk Factors of Mortality.
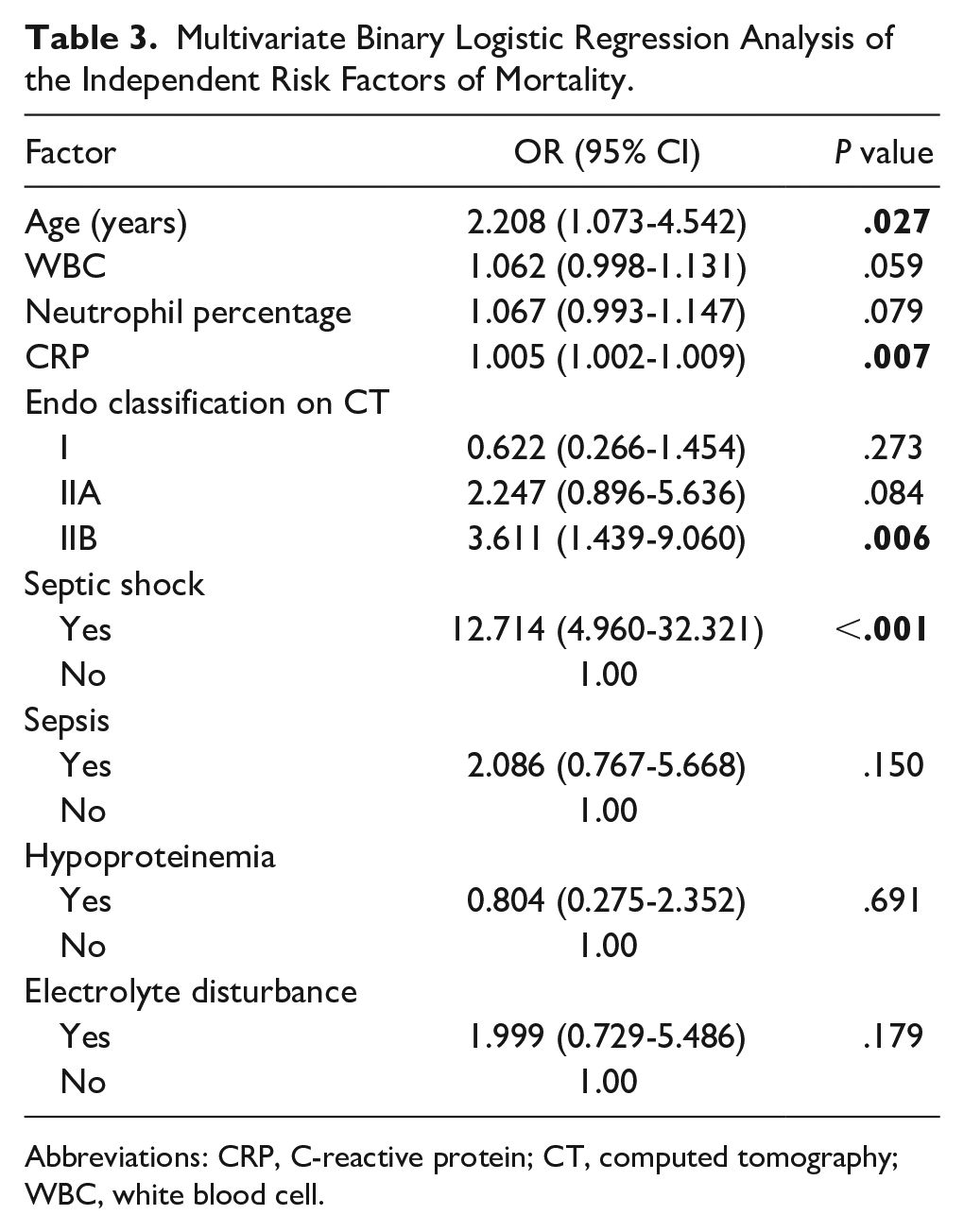
Abbreviations: CRP, C-reactive protein; CT, computed tomography; WBC, white blood cell.
Discussion
Our study found that the most important clinical characteristic of DNM is high mortality, reaching 21.55%. Then we found that age, Endo classification type IIB, septic shock, and high CRP level on admission were independent risk factors of mortality.
DNM is a potentially life-threatening infection, but effective antibiotic therapy and timely abscess drainage can prevent and cure the infection. However, there is still a significant risk of mortality. Although the mortality rate had significantly decreased, 15 in the current study, the rate was still high at 21.55% despite timely surgery and antibiotic therapy. This rate is consistent with that previously reported (16.5%-74%).3,4 DNM can occur as early as 1 year of age 16 ; in this study, the youngest patient was aged 8 months. Further, DNM can occur in any age group, including infants. In this study, the deceased patients were older than those who survived. Aging has led to an increase in the incidence of severe disease and mortality worldwide. Older age is also a predisposing factor for mediastinal extension of DNM. 5 Age >55 or 60 years is a high-risk factor for death in DNM. 15 The current study found that the risk of death increased by 2.208% per 1-year increase in age.
DNM more commonly affects men, 17 and the pathogenic risk factors include hypertension, type 2 diabetes mellitus, obesity, and immune system diseases. 18 However, we found that these risk factors were not directly associated with mortality but rather contributed to the occurrence and exacerbation of neck infections. Physicians should actively control blood sugar and blood pressure to prevent further aggravation of the infection. We found that 3 inflammatory markers, namely, WBC count, neutrophil percentage, and CRP, were higher in patients who died. Additionally, high CRP levels were associated with increased patient mortality. Elevated CRP levels have been reported to predict all-cause mortality, even after adjusting for other risk factors. 19 Notably, increased CRP levels indicate poor prognosis. 20
With respect to patient complications at admission, septic shock, sepsis, hypoproteinemia, and electrolyte disorders were associated with mortality. Particularly, septic shock was a risk factor for mortality after excluding confounders, and septic shock was the major cause of mortality in our cohort. The pathophysiology of septic shock is complex.19,21 Oxidative stress is one of the most important mechanisms underlying the progression of septic shock to multiple-organ failure. 22 Cui et al found that septic shock and multiple complications were associated with poor prognosis, which could be attributed to delayed presentation, late diagnosis, improper antibiotic agents, or inadequate drainage and debridement. 19 Septic shock occurs during the disease process and is a high-risk factor for mortality. However, the heterogeneity of septic shock hinders the generation of reproducible data regarding mortality risk, with rates ranging between 15% and 56%. 23 A retrospective study using a national critical care database reported a higher hospital sepsis mortality rate of 55.5% in patients with septic shock (vs 31.8% in the overall population). 24
Although studies have predominantly focused on dental infections, especially severe cases with mediastinal infections or necrotizing fasciitis, there is also evidence of higher proportions of tonsillar or salivary infection origins.12,18,25 With respect to etiology, odontogenic and pharyngolaryngeal infections were the main causes of DNM in the current study, consistent with the findings of several studies. Foreign bodies in the throat and esophageal inlet were also important causes of DNM, accounting for 13.26% of the infections. This variation in pathogenesis suggests regional or demographic differences. However, the cause of DNM is not related to patient death. 22 In general, the origin of an infection is related to its pattern of spread through the fascial spaces. Different etiologies are associated with different bacterial infections. However, the use of powerful broad-spectrum antibiotics and guidance regarding bacterial culture can effectively address the vast majority of pathogenic bacteria. 26
The relatively high proportion of patients with no bacterial growth in culture is in accordance with previous findings. 22 The proportion of G+ aerobic organisms was significantly higher than that of other aerobic organisms in this study. Oral-, pharyngeal-, and foreign body-origin pathogens were the most common causative pathogens, whereas anaerobic bacteria were less frequently found. Bacteria were detected in only 40.89% of the current patients, and all bacteria detected were aerobic. There are several reasons for this. In addition to regional or demographic differences, some patients may have been receiving oral or intravenous antibiotics before admission, which could have resulted in a low detection rate of positive bacterial culture. Moreover, during sample collection, a syringe was used to extract pus from the abscess cavity, cut the necrotic tissues in the opened abscess cavity, and place them in a culture dish. A complete and closed specimen collection method to identify pathogenic bacteria in abscesses needs to be developed. Notably, we did not identify any specific pathogens or pathogenic strains that correlated with a higher risk of mortality. Given the diversity of infection sources and the high rate of negative bacterial culture, the use of broad-spectrum antibiotics is essential.
Empirical antimicrobial therapy should be used to treat causative microorganisms, whereas surgery and supportive measures should be used to reduce the inoculum of pathogens by providing adequate drainage and debridement. One report linked increased morbidity to delayed surgical therapy. 27 Planned surgical revisions with drainage are an integral part of the treatment, and active surgical treatment and drainage of abscesses on the day of admission are necessary. However, the surgical route for patients with mediastinal involvement is still debated. Some authors favor transcervical incision, with others recommending a transthoracic approach.27-29 Transcervical mediastinal drainage is the first-line treatment option for patients with limited disease in the upper mediastinum. For patients with infections in the lower anterior mediastinum, an additional subxiphoid approach is suggested. 30 A transcervical incision with VATS mediastinal drainage is an excellent combination approach for patients with infections in the posterior mediastinum and pleural space. 13
Traditionally, extensive surgery has been associated with a higher risk of death 31 because more extensive infections typically require more aggressive surgical interventions. A wider operative field increases the risk of complications, such as bleeding, massive tissue injury, osteomyelitis, and dehiscence of the sternum. 13 However, the current study found that the surgical method and secondary abscess incision and drainage were not correlated with mortality. Patients treated with multiple large surgical incisions may have poor prognoses.32,33 However, we found no correlation between the surgical method and the probability of secondary injury or mortality. Chen et al reported that thoracotomy was the preferred access method for treating Endo type IIA and IIB DNM. They believed that this method provided the best view of the mediastinum and allowed the best debridement and drainage. 13 It was faster and facilitated adhesiolysis and palpation during dissection and debridement of the mediastinum. In the current study, the mortality rate did not differ by operation type (transcervical mediastinal drainage, transcervical surgery and VATS, and transcervical surgery and thoracotomy).
This study has several limitations. First, as a retrospective study, data on antibiotic use in patients prior to admission from outside hospitals were incomplete, preventing a thorough analysis of antibiotic treatment. Additionally, the extended time span of the study may have introduced variability in mortality rates and risk factors, as advances in medical technology and updates in pharmaceutical treatments likely influenced patient outcomes over the years. These factors may have affected the consistency and comparability of results across the study period.
Conclusion
Old age and high CRP level at admission increased the risk of mortality in DNM. Endo type IIB classification and septic shock were associated with poor prognosis. Abscesses tend to spread more widely in older patients. Early and proactive treatment of neck, throat, and dental infections should be strongly encouraged to prevent DNM progression. Aggressive surgical debridement of deep cervical spaces and the mediastinum and intravenous broad-spectrum antibiotic therapy are mandatory. Our findings underscore the importance of early identification and aggressive management of high-risk patients, particularly older individuals and those with elevated CRP levels or septic shock. Recognizing these risk factors can help clinicians stratify patients more effectively and guide treatment decisions. Furthermore, understanding the prognostic value of Endo classification type IIB on CT could lead to improved diagnostic protocols and targeted therapeutic interventions, potentially reducing mortality rates in DNM. These insights may also encourage further research into early biomarkers and novel therapies for this high-mortality condition.
Footnotes
Acknowledgements
We thank our coworkers and the Information Center for their support in writing this article.
Author Contributions
M.C.: writing the first draft of the manuscript, data collection, organizing, and assigning tasks. L.L.: data analysis and interpretation of results, literature search. N.S.: study design, development of the original protocol, revision of the manuscript, and funding support. Y.Z.: design of the study, development of the original protocol, and revision of the manuscript. H.Y.: original screening of papers and data extraction. Z.J.: analysis and interpretation of the data. J.Z.: development of the original protocol and funding support. All the authors have read and agreed to the published version of the manuscript.
Data Availability Statement
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by characteristics of upper respiratory tract flora in children with obstructive sleep apnea-2023 Chengdu Medical research project (grant number 2023152, Min Chen) and 1·3·5 project for disciplines of excellence–Clinical Research Fund, West China Hospital, Sichuan University.
Ethical Considerations
This study was approved by the Ethics Committee of West China Hospital.
Consent to Participate
The need for informed consent was waived owing to the retrospective nature of the study.
Consent for Publication
Not applicable.