
Abstract
Objectives:
Descending necrotizing mediastinitis (DNM) is a serious and progressive infection involving the neck and chest and with high mortality if not treated quickly and properly. The aim of this study is to share our practices for managing this condition.
Methods:
We retrospectively evaluated 9 patients diagnosed with DNM in our hospital between January 2006 and October 2019. Age, gender, origin of infection, length of hospital stay, microorganisms present, type of surgical treatment, and clinical outcomes were reviewed.
Results:
All patients underwent surgery to drain neck and mediastinal secretions and collections. Three (33.3%) patients were treated with transcervical drainage alone, and 6 (66.7%) patients were treated with combined transcervical and transthoracic drainage. Reoperations were reported in 3 (33.3%) cases. The average length of hospital stay was 22.78 ± 10.05 days (range: 9-40 days). The average length of intensive care unit stay was 6.44 ± 10.10 days (range: 0-25 days). There were no in-hospital deaths, and all patients were discharged home with good outcomes.
Conclusions:
To improve the prognosis of DNM, we suggest early and adequate debridement of all affected areas along with the proper use of antibiotics. A multidisciplinary approach involving both cardiothoracic and ENT surgeons is also required.
Keywords
Introduction
Descending necrotizing mediastinitis (DNM) is a serious and progressive infection involving the neck and chest with high mortality if not treated quickly and properly, 1 and thorough surgical debridement at the earliest opportunity is essential for good prognosis. Here, we review our 13-year experience of managing this condition in our hospital.
Patients and Methods
We retrospectively evaluated a total of 9 patients diagnosed with DNM in our hospital between January 2006 and October 2019. The following diagnostic criteria for DNM were established by Estrera et al 2 : (1) clinical manifestations of severe oropharyngeal or cervical infection, (2) demonstration of characteristic radiographic features of mediastinitis, (3) surgical or postmortem evidence of DNM, and (4) correlation between oropharyngeal/cervical infection and the development of DNM. Age, gender, origin of infection, length of hospital stay, microorganisms present, type of surgical treatment, and clinical outcomes were reviewed. The total follow-up duration was at least 3 months.
We evaluated all patients with preoperative computed tomography (CT) scan to establish the diagnosis. The type of DNM was classified according to the criteria of Endo et al 3 as type 1 = infection above the carina and type 2 = infection below the tracheal bifurcation, which is further subdivided into type 2A (lower anterior mediastinum) and type 2B (lower posterior mediastinum). All the work didn’t involve the use of animal or human subjects. And there is no identification of patients.
Data Analysis
Statistical analysis was performed using SPSS 22.0. Data were expressed as the mean ± standard deviation.
Results
All patients presented with typical symptoms, histories, and radiological findings. There were 6 (66.7%) male and 3 (33.3%) female patients, with a mean age of 44.33 ± 13.54 years (range: 23-64 years). Of these 9 patients, 3 (33.3%) patients were diagnosed with diabetes. Primary pathology was odontogenic (n = 3), parapharyngeal (n = 3), tonsillar infection (n = 2), and cervical infection (n = 1). Seven (77.8%) patients were type 1 and 2 (22.2%) patients were type 2.
Blood tests and microbiological assessment of secretions and tissues were performed in all patients. Broad-spectrum antibiotics were used in all patients immediately upon presentation at the hospital and subsequently adjusted according to the results of the cultures. Identified microorganisms were detected in 3 patients, including Gram-positive combined with anaerobic bacteria (n = 1), actinomyces (n = 1), and Stenotrophomonas maltophilia (n = 1). No microorganisms could be identified in the other 6 patients.
All patients underwent surgery to drain neck and mediastinal secretions and collections. Of these 9 patients, 3 (33.3%) patients were treated with transcervical drainage alone, and 6 (66.7%) patients were treated with combined transcervical and transthoracic drainage. Video-assisted thoracic surgery (VATS) was performed in 3 (50%) of these 6 patients. Reoperations were reported in 3 (33.3%) of the 9 cases. An indwelling thoracic drainage tube was used in all patients, and a washing tube was used in 3 of them. The cervical incision was left open followed by secondary closure in 1 patient (Figure 1) due to severe tissue necrosis. Only 2 (22.2%) patients underwent tracheotomy for airway compromise (presurgical, outside the hospital) and for long-term treatment after surgery. The average length of hospital stay was 22.78 ± 10.05 days (range: 9-40 days). The average length of intensive care unit stay was 6.44 ± 10.10 days (range: 0-25 days). There were no in-hospital deaths, and all patients were discharged home with good outcomes. The patients’ first seen time after hospital discharge ranged from 7 to 14 days. The clinical characteristics of the patients and the surgical approaches are summarized in Table 1. A typical case is shown in Figure 1.
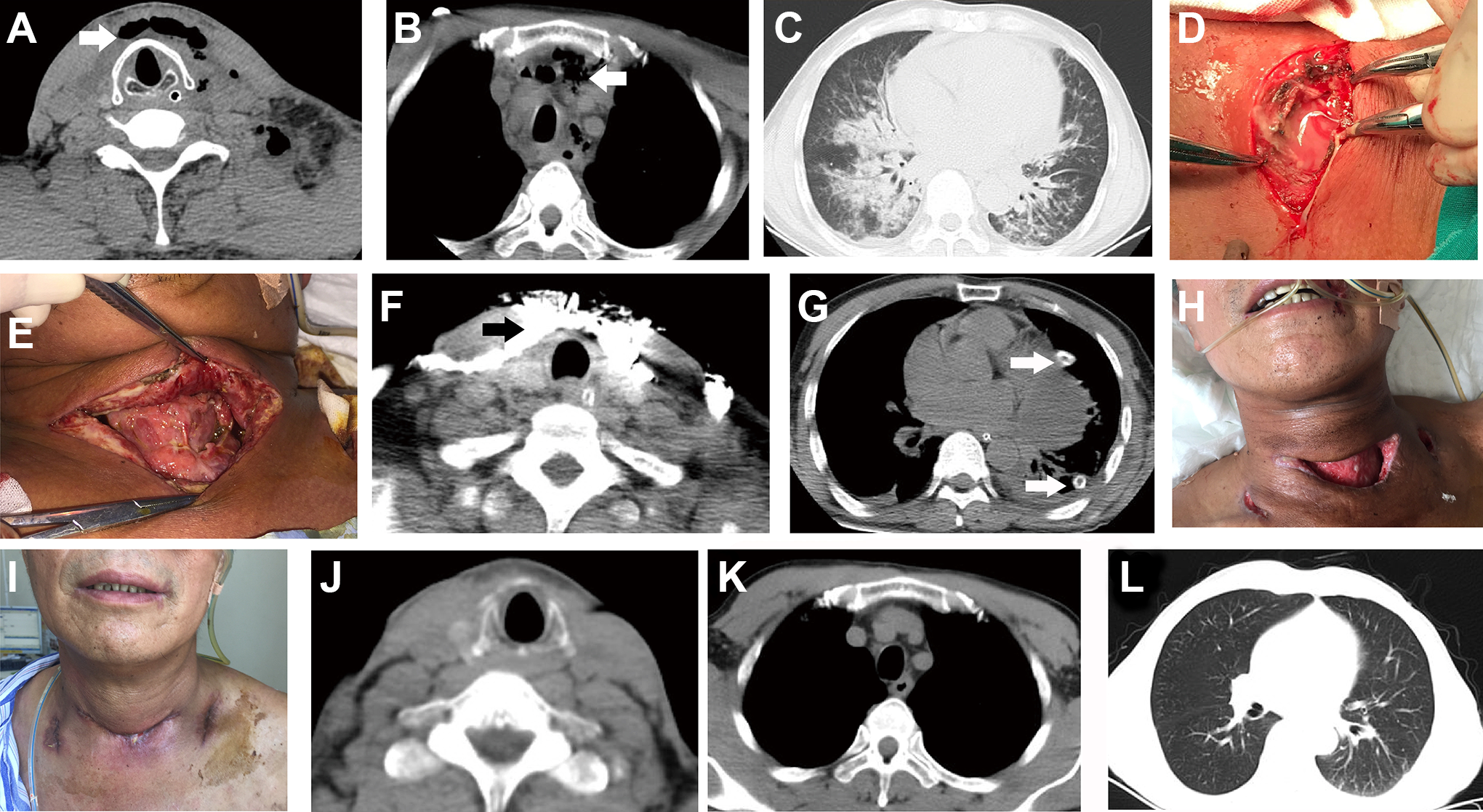
A-C, Axial computed tomography (CT) of the neck and chest before surgery. Air was observed in the neck and mediastinum (A and B, white arrow), and pulmonary infection was observed (C). D, Intraoperative view of necrotic tissue within the neck. E, The cervical incision was left open for 9 days. F, Iodoform gauze (black arrow) within the cervical incision. G, The use of an indwelling thoracic drainage tube (white arrow). H, Infection of the cervical incision was controlled. I, Secondary closure of the cervical incision. J-L, Axial CT of the neck and chest after surgery. The radiological findings were obviously improved.
Clinical Characteristics of Patients and the Surgical Approaches.
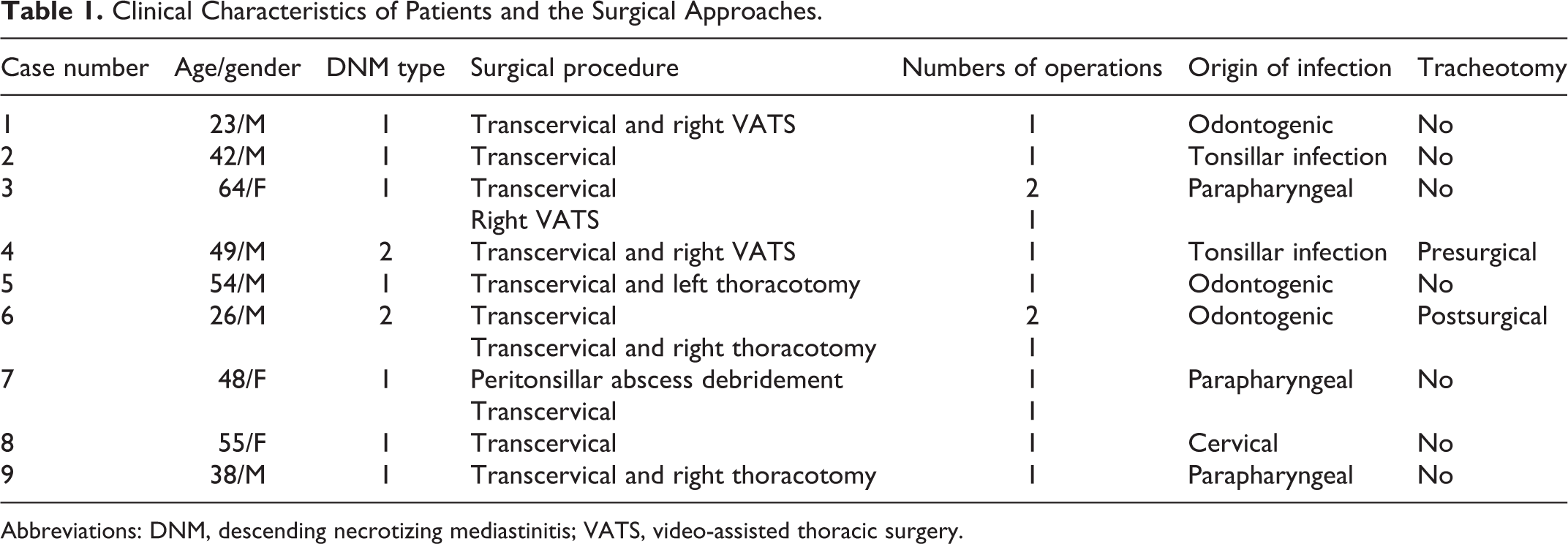
Abbreviations: DNM, descending necrotizing mediastinitis; VATS, video-assisted thoracic surgery.
Discussion
Descending necrotizing mediastinitis is an uncommon but life-threatening disease caused by odontogenic, pharyngeal, or cervical infection spreading into the mediastinum through the anatomical cervical fascial planes, including the retropharyngeal, pretracheal, and paraesophageal planes.
The most frequent cause of DNM is odontogenic infection (60%-70%), 4 and other causes include parapharyngeal or peritonsillar abscess, epiglottitis, thyroiditis, trauma, and iatrogenic injury such as tracheal rupture caused by endotracheal intubation. 2 Risk factors for DNM include poor dentition, diabetes, AIDS, and excessive alcohol consumption. 5 In our study, odontogenic infection and parapharyngeal infection were the most common origins (n = 3 for both), and 3 of the 9 (33.3%) patients had diabetes.
Clinical presentation is often mild and nonspecific, thus almost always leading to late diagnosis. Typical symptoms related to initial cervical or odontogenic infection include fever, pain, dysphagia, neck edema, and dyspnea. However, infection can spread rapidly into the mediastinum if treatment measures are insufficient, leading to chest discomfort, respiratory distress, sepsis, and eventually death. Early recognition, diagnosis, and treatment are associated with good prognosis.
Computed tomography scanning is the gold standard for early detection and diagnosis of DNM. It can assess the extent of infection, establish the diagnosis, and aid with surgical treatment. 6 -8 The type of DNM can also be classified according to CT scanning, as mentioned before. However, 2 patients in our study showed infections within both lower anterior mediastinum (type 2A) and posterior mediastinum (type 2B). So, we think it may be more suitable to subdivide type II into type 2A, 2B, and 2C. A postoperative control CT scan of the neck and thorax at 48 to 72 hours or in the case of clinical deterioration is recommended to determine the necessity of reoperation.
Descending necrotizing mediastinitis is mainly a mixed anaerobic and aerobic polymicrobial infection, and Streptococcus anginosus, Staphylococcus aureus, Prevotella, and Fusobacterium necrophorum are among the most commonly observed organisms. 5,9 In patients with diabetes, Gram-negative bacteria such as Klebsiella can also be identified. 10 Broad-spectrum antibiotics that cover Gram-positive and anaerobic bacteria as well as Gram-negative bacteria (in diabetic patients) are crucial to limit the further spread of infection. Antibiotic therapy should be adjusted according to the results of microbiological assessment. In our study, identified microorganisms were detected only in 3 patients, and no microorganisms could be identified in the other 6 patients. This might be due to the use of antibiotics prior to culture.
Antibiotic therapy alone is insufficient for the treatment of DNM, which has a high mortality (55%-86%), 11 and early surgical intervention by ENT and cardiothoracic surgeons is essential. The surgical approach is determined according to the type of DNM, and there is consensus that drainage of both the original and the mediastinum infection is necessary. In our study, 3 patients underwent reoperations because only peritonsillar, submandibular, or parapharyngeal abscess drainage was performed during their primary surgery. For patients with type 1 DNM, a transcervical incision with extension to the bilateral sternocleidomastoid muscles is recommended because this can provide excellent exposure for judicious debridement and drainage within the neck. The anterior mediastinum can also be accessed using this approach. 9,12 In cases of advanced disease (type 2) with higher mortality, a more aggressive surgical approach via thoracotomy (especially for type 2B) combined with transcervical debridement is recommended. 9,11 Right posterolateral thoracotomy provides better access compared to the left thoracotomy, and it is well tolerated in most patients and can afford excellent access to the thoracic cavity. However, left thoracotomy is also reliable if the left side is severely affected. In some cases of superior mediastinitis (type 2A), a subxiphoid incision is also reliable. 13,14 Drainage of the superior mediastinum by sternotomy has also been reported, but this is unfavorable due to the high risk of osteomyelitis.
Some reports also recommend the use of VATS, which has shown similar results to open approaches and can also be used in children. 10,11,14 However, this allows only narrow access to the mediastinum, limiting the ability of the surgeon to excise all of the affected necrotic tissue. Thus, it should only be used in select cases. In our study, VATS was performed in 3 (50%) patients (type 1, n = 2 and type 2, n = 1) because it offered a minimally invasive approach to the drainage of mediastinal and pleural collections. No complications or deaths occurred in these 3 patients. An indwelling cervical, thoracic, or mediastinal drainage tube should be used in all patients, and a double-lumen tube can be used for washing.
In patients with airway compromise or in those needing long-term treatment, tracheotomy is recommended. However, its routine use is controversial because cervical infection contamination may occur. 14 Only 2 of the 9 cases in our study received a tracheotomy. One case (case 4) was given tracheostomy before hospitalization, because of dyspnea. The decannulation was performed 3 weeks after drainage. The other case (case 6) was given tracheostomy 10 days after drainage, because of prolonged endotracheal intubation. And the decannulation was performed 17 days after tracheostomy. The 2 cases were discharged well without any dyspnea or secondary bacterial pneumonia.
Conclusion
Descending necrotizing mediastinitis is an acute and life-threatening disease, and CT scanning is the gold standard for early diagnosis and can also guide the selection of surgical approach. However, in our opinion, it may be more suitable to subdivide type II into type 2A, 2B, and 2C. In our study, all patients were discharged from our hospital, and no deaths occurred. We suggest early and adequate debridement of all affected areas, as well as the proper use of antibiotics. A multidisciplinary approach involving both cardiothoracic and ENT surgeons and intensive postoperative care is also required. Video-assisted thoracic surgery is promising in certain cases, and the cervical incision can be left open followed by secondary closure in some cases. Routine tracheotomy is not necessary in all patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.