
Abstract
Background
Thyroid cancer is the most common endocrine malignant tumor in children, and its incidence is increasing year by year. 1 The most common subtype of thyroid cancer in children is papillary thyroid carcinoma (PTC), which is prone to cervical lymph node metastasis earlier. Pediatric thyroid cancer is more aggressive, more prone to cervical lymph node metastasis, and has higher recurrence rate than adults. Total thyroidectomy is the first choice for most pediatric thyroid cancer, and therapeutic or prophylactic central lymph node dissection is frequently required at the same time. Hypoparathyroidism (HP) is the most common endocrine-related complication of this surgery. 2 Up to 20% of patients will develop HP after surgery, and hypocalcemia caused by HP can cause a series of clinical manifestations, such as perioral numbness, hand and foot paresthesias in mild cases, and life-threatening seizures, refractory heart failure, or laryngospasm in severe cases. Most of the HP after thyroidectomy is temporary, and as the level of parathyroid hormone gradually recovers, the intensity of calcium supplementation therapy needs to be adjusted accordingly. Once permanent HP occurs, the quality of life of children will be greatly affected. Therefore, the study of the recovery regularity and influencing factors of HP can provide reference for surgical strategy and postoperative treatment. There is no report on the recovery of HP after total thyroidectomy in children. The purpose of this study was to analyze the recovery pattern of parathyroid hormone (PTH) in children with hypoparathyroidism (HP) after total thyroidectomy. Additionally, we aimed to understand the factors influencing HP recovery and provide a reference for developing effective diagnosis and treatment strategies, thereby minimizing the adverse effects of HP on the quality of life of children undergoing thyroidectomy.
Materials and Methods
A retrospective study was conducted in pediatric thyroid cancer who were admitted to Beijing Children’s Hospital (BCH) affiliated to Capital Medical University from June 2016 to December 2020. All operations were performed by a consistent surgical team, led by a senior surgeon who performed the majority of the procedures. The team included assistant surgeons and other health care professionals who were present during each surgery to maintain uniformity in surgical technique and patient care. The study protocol was approved by the Medical Ethics Committee of BCH. The inclusion criteria were as follows: (1) PTC was pathologically diagnosed; (2) first surgery; (3) the operative approach was total thyroidectomy plus ipsilateral central neck dissection, and whether to perform contralateral central and lateral neck dissection was determined according to clinical evidence. (4) HP occurred on the first postoperative day (ie, PTH < 10 pg/mL). The exclusion criteria were as follows: (1) pathological diagnosis of thyroid adenoma or nodular goiter; (2) multiple surgical treatment; and (3) subtotal thyroidectomy or lobectomy. The primary outcome variable was the factors affecting postoperative HP, and the secondary endpoint was the recovery time of HP.
The enrolled children were operated in accordance with the principles of the “Expert consensus on thyroid nodules and differentiated thyroid cancer for Chinese children (2020).” 3 The operative approach was total thyroidectomy plus ipsilateral central neck dissection, and whether to perform contralateral central and lateral neck dissection was determined according to clinical evidence. Intraoperative identification of the parathyroid glands was primarily conducted by the operating surgeon and documented in the operative report. However, in cases where the identification of parathyroid tissue was uncertain or when there was concern about possible inadvertent removal of the parathyroid glands, intraoperative frozen section analysis was used to confirm the identity of the tissue. Postoperative PTH levels were routinely measured on the first day after surgery, and clinical data were collected, including age, gender, operation, TNM stage, location, intraoperative confirmation and protection of parathyroid gland, lymph node metastasis, and dissection. Calcium and vitamin D supplementation were initiated based on the postoperative PTH levels and clinical signs of hypocalcemia. For patients with PTH ≤1 pg/mL or clinical symptoms of hypocalcemia, calcium and active vitamin D (calcitriol) supplementation was provided. Tailored supplementation was given to patients with normal PTH levels and no symptoms. Patients with a PTH level of ≥10 pg/mL on postoperative day 1, with stable serum calcium levels, are considered for gradual discontinuation of supplementation. For patients with PTH levels <10 pg/mL, calcium and calcitriol are continued until both PTH and serum calcium levels normalize without symptoms of hypocalcemia.
The recovery of parathyroid function was regularly followed up after discharge, and the recovery time of parathyroid function was recorded. The follow-up time was more than 1 year. Temporary HP was defined as PTH < 10 pg/mL (reference range 10-65 pg/mL), which returned to normal within half a year after surgery. 4
All statistical analyses of clinical data were performed using the SPSS software (version 20.0; Chicago, IL, USA), with the significant statistical threshold of 2-tailed P value <.05. Summary descriptive statistics were calculated for demographic and disease characteristics. A two-independent samples t-test was used to compare the continuous variables that met normality. Nonparametric test was used to compare the continuous variables that did not meet the normality. Categorical variables were compared by Pearson’s chi-squared (χ2) test and the Fisher exact test. Binary logistic regression analysis was used to evaluate the risk factors of HP.
Results
A total of 121 patients with thyroid cancer underwent total thyroidectomy and central compartment dissection, and 34 (28.1%) had postoperative HP. Eighteen patients (52.9%) had PTH >1 pg/ml on the first postoperative day. The clinicopathological characteristics are shown in Table 1. The average age of the patients was 10.34 ± 3.01 years (range: 3.32-15.33 years). The male-to-female ratio was 1:1.83. All 34 children underwent total thyroidectomy and cervical lymph node dissection, of which 32 cases (94.1%) underwent bilateral central neck lymph node dissection and 2 cases underwent unilateral central lymph node dissection. According to TNM stage, 4 cases (11.8%) were T1 to T2 stage and 30 cases (88.2%) were T3 to T4 stage. All 34 patients had central lymph node metastasis, including 11 cases (32.4%) with unilateral metastasis and 23 cases (67.7%) with bilateral metastasis. There were 30 cases (88.2%) with lateral cervical lymph node metastasis. Among the 34 patients, 7 (20.6%) had distant metastasis (all pulmonary metastasis).
Demographic, Clinical, and Pathological Characteristics of 34 Patients.
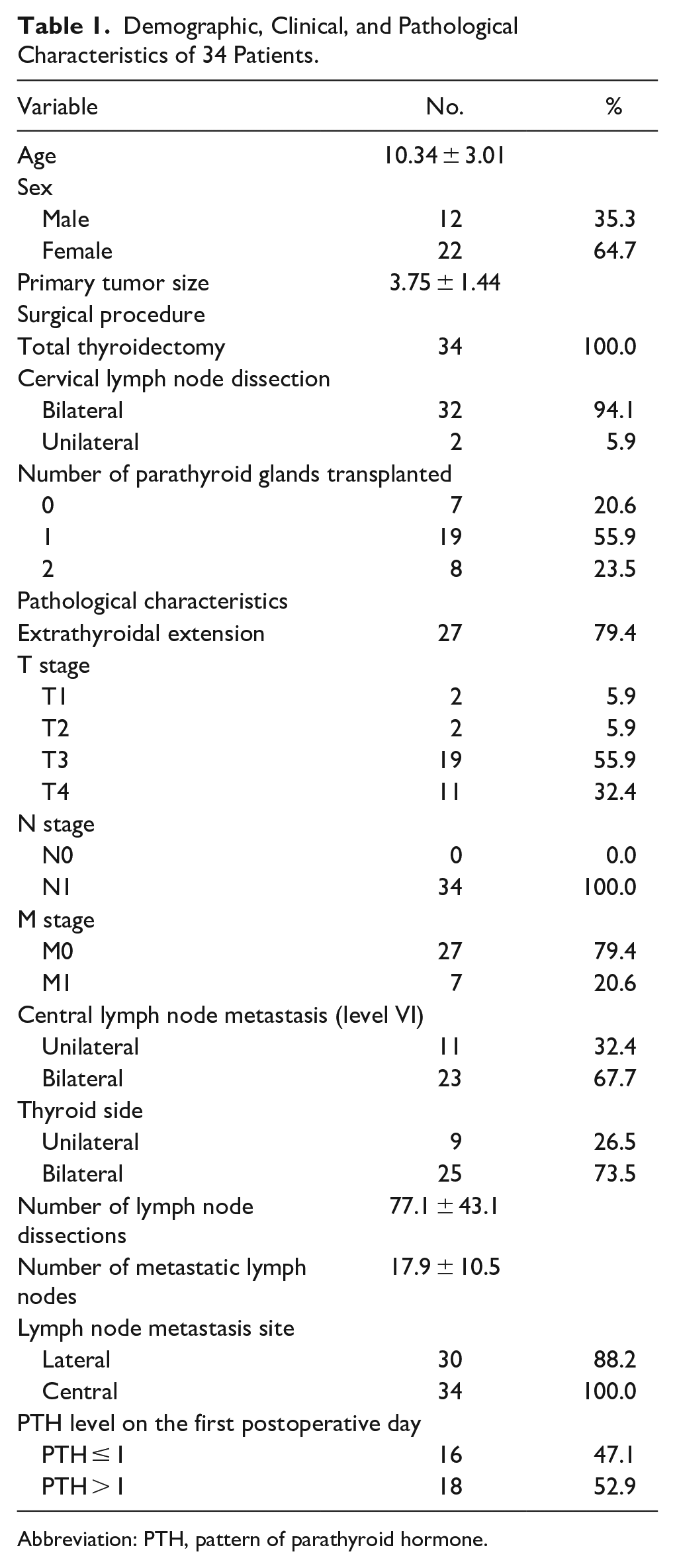
Abbreviation: PTH, pattern of parathyroid hormone.
In terms of postoperative PTH recovery, 18 cases (52.9%) returned to normal within 1 month after surgery, 25 cases (73.5%) returned to normal within 6 months after surgery, and 30 cases (88.2%) returned to normal within 1 year after surgery. Two cases returned to normal at 14th month and at 2nd year after surgery, respectively. In 2 cases, PTH still did not return to normal at the last follow-up time (2nd year and 5th year after surgery, respectively). The TNM stage of these 2 patients were T4N1bM0 and T4N1bM1, respectively. They both had extensive extrathyroidal invasion and multiple metastases of bilateral lymph nodes and underwent total thyroidectomy and bilateral cervical lymph node dissection, both PTH < 1 pg/mL on the first postoperative day.
The results of univariate analysis showed that PTH ≤ 1 on the first postoperative day and bilateral central lymph node metastasis (level VI) were statistically different in postoperative PTH recovery time (P < .05), which were risk factors affecting postoperative parathyroid function recovery. However, there were no significant differences in age, gender, tumor diameter, bilateral lymph node dissection, the number of transplanted parathyroid glands, the number of parathyroid glands in situ, extrathyroidal extension, T stage, M stage, the number of lymph node dissection, and lateral cervical lymph node metastasis between the temporary HP group and the non-temporary HP group (P > .05) (Table 2). In multivariate analyses, the first postoperative day PTH ≤ 1 was independent risk factor for postoperative HP recovery (OR = 0.092, 95% CI: 0.009 to 0.966, P = .047; Table 3).
Comparison of Clinical Characteristics of HP Recovery Time Between≤ 6 months and >6 months Groups.
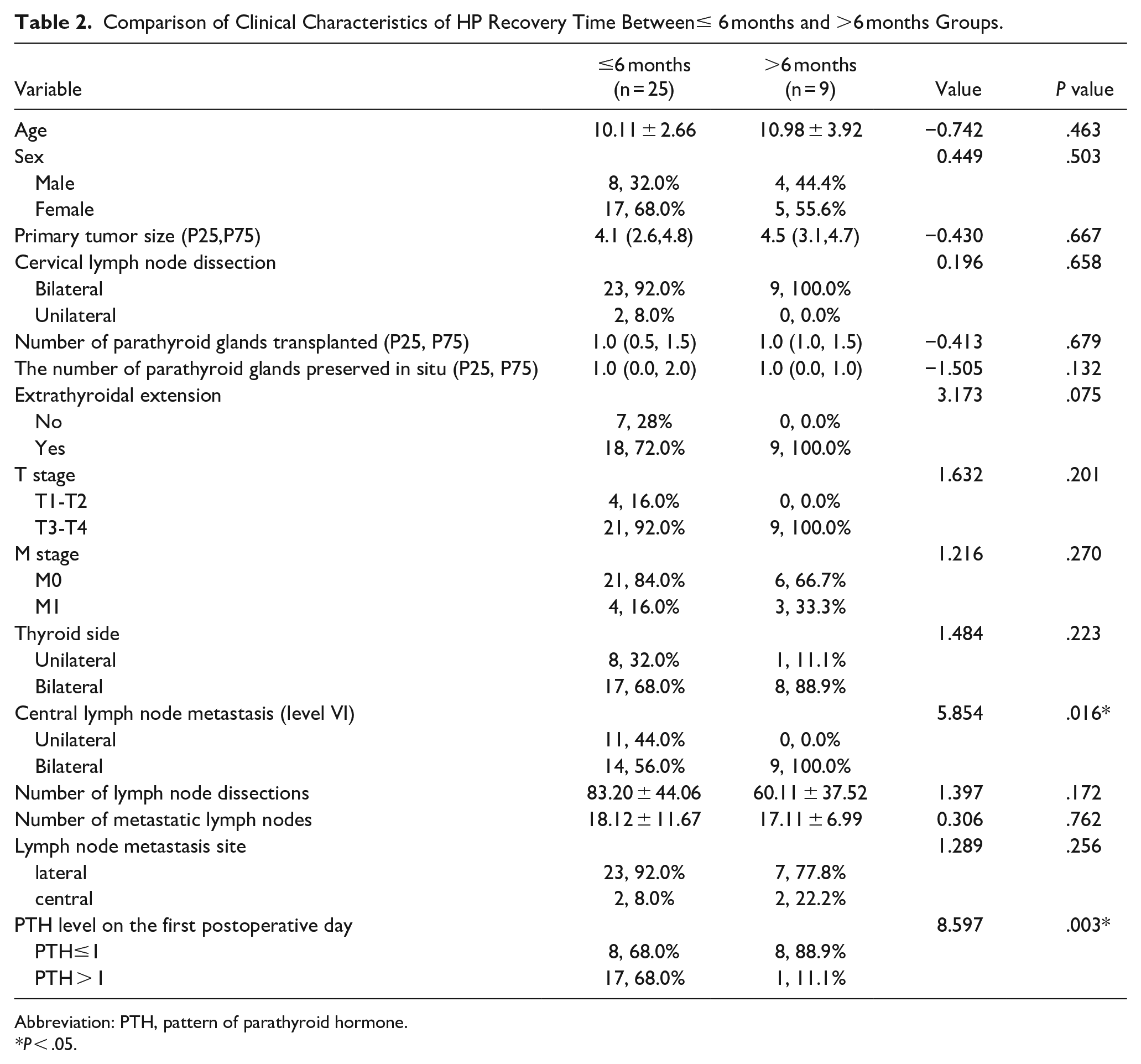
Abbreviation: PTH, pattern of parathyroid hormone.
P < .05.
Multivariate Logistic Regression Analyses of HP Recovery.
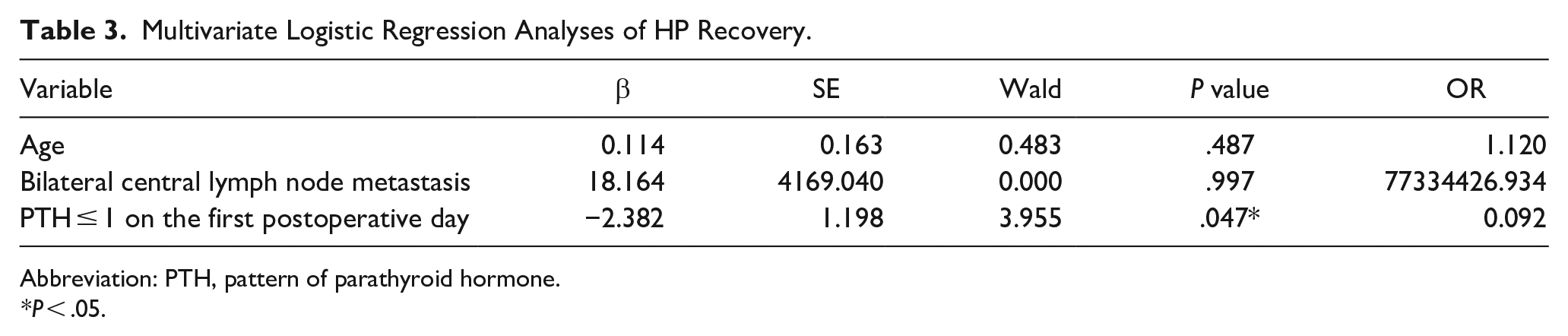
Abbreviation: PTH, pattern of parathyroid hormone.
P < .05.
Discussion
HP is a common complication of thyroid surgery. Postoperative PTH levels may be undetectable or lower than normal, necessitating exogenous calcium and vitamin D supplementation. If permanent HP occurs, lifelong medication is required. However, large doses of calcium and active vitamin D may lead to hypercalciuria, renal calculus, nephrocalcinosis, and ectopic calcification, all of which can significantly affect quality of life. Therefore, protecting the parathyroid glands during surgery is particularly important. Complications associated with thyroid surgery are higher in pediatric patients than in adults. 5 Previous studies6-9 have reported that the incidence of temporary HP after surgery in children is 13% to 47%, and the incidence of permanent HP is 0.9% to 8%. Notably, complications are more prevalent in children under 6 years old, with the highest incidence occurring in children under 1 year.10,11 In our cohort, the incidence of postoperative HP was 28.1%, which falls within the ranges reported in the current literature on pediatric thyroid surgery. Several factors contributed to the incidence of HP in our study. First, the average age of patients was 10.34 years, with a minimum age of 4 years. Young children have a fine anatomical structure, making structural identification more challenging. The parathyroid glands are small, light color, and immature, and it is difficult to distinguish from the surrounding fatty lymph nodes and other tissues. Second, due to the higher rate of lymph node metastasis, most patients (94.1%) required bilateral cervical lymph node dissection, increasing the likelihood of tumor fusion into a hard mass that occupies the position of the parathyroid gland. Additionally, 88.3% of patients presented with T3 to T4 stage thyroid cancer, indicating more aggressive local invasion and a higher clinical stage. Thyroid cancer is more likely to break through the capsule and grow diffusely, so the difficulty of surgery is significantly increased. These factors complicate the surgical procedure, increasing the difficulty of identification and the preservation of the parathyroid glands.
The main causes of postoperative HP are unintentional parathyroidectomy, parathyroid autotransplantation, glandular vascular dissection, and parathyroid vein drainage obstruction, resulting in a decrease in functional parathyroid parenchyma. 12 Therefore, careful identification, reducing miscuts, and protection of blood supply are the key points during surgery to prevent postoperative HP. The retention of parathyroid in situ is particularly important for maintaining postoperative calcium homeostasis.
Central lymph node dissection is one of the important factors that affect the recovery of PTH after total thyroidectomy.13-16 Considering that central lymph node dissection may lead to intraoperative parathyroid damage or blood supply disorder, all children in this study underwent central lymph node dissection, resulting in a higher proportion of postoperative HP than adults. In addition, this study also found that bilateral central lymph node metastasis is a risk factor for postoperative parathyroid recovery, primarily due to the fact that central lymph node metastasis leads to more extensive lesions, making the structure less recognizable, thus complicating the surgery and making it difficult to find the parathyroid gland during the procedure.
At present, it is recognized that parathyroid autotransplantation after parathyroid missection is of great significance for the prevention of postoperative hypocalcemia and HP, 17 and the immediate survival rate of parathyroid autotransplantation can be as high as 90%. Therefore, the guidelines recommend that if it cannot be preserved in situ, immediate autotransplantation of the parathyroid gland should be routinely performed,17,18 and transplantation of the parathyroid gland into the sternocleidomastoid muscle should be considered to reduce the incidence of permanent HP. However, some reports found that parathyroid autotransplantation had no effect on the recovery of parathyroid function. A. Siges-Serra et al. 14 found that parathyroid autotransplantation did not protect against permanent HP. The results of this study showed that there was no significant difference between the number of transplanted parathyroid glands and the recovery time of parathyroid glands (P > .05), which was consistent with our report. Validation is required in a large sample cohort to understand the role of parathyroid autotransplantation in the reduction of HP.
PTH assay is a reliable early predictor, as it may allow earlier identification of patients requiring treatment for postthyroidectomy hypocalcemia and should be routinely monitored after thyroid surgery. Some studies19-22 have found that PTH levels on the first day after total thyroidectomy can be used to predict postoperative HP, and its predictive value is high. The main reason is that the higher the PTH level on the first day after surgery, the lesser the parathyroid gland damage during surgery, the better the protection of blood supply, and the easier it is for parathyroid function to recover. The results of our study, through multivariate analysis, found that PTH ≤ 1 on the first day after surgery was an independent risk factor for postoperative HP recovery, which further confirmed the results. Moreover, it is crucial to consider vitamin D deficiency in these patients, as it significantly impacts PTH levels. Current guidelines define vitamin D deficiency as a serum PTH level above +2 standard deviations in children. Our current research did not specifically assess vitamin D status, which is a limitation of this study. Future research should focus on evaluating the impact of vitamin D deficiency on postoperative recovery of parathyroid function, particularly in children with elevated PTH levels.
Sitges-Serra et al. 14 found that 29.6% of children with parathyroid function recovered within 1 month, while 18.1% of patients developed protracted persistent hypoparathyroidism, and their study also found that parathyroid function recovered within 1 year in 78% of patients with protracted persistent HP. They suggested that medical “parathyroid splinting” with high doses of calcium and vitamin D to keep serum calcium in the normal to high range might be a better therapeutic strategy for patients with postoperative hypocalcemia. In our study, PTH returned to normal in 88.2% of patients within 1 year after surgery. However, there is no consensus on the duration of permanent HP. European guidelines define permanent hypoparathyroidism as low serum iPTH concentrations and/or the need for replacement therapy for 6 months after surgery, 23 while the American Association of Clinical Endocrinologists extends the period to 1 year. 24 There are limited empirical data on the follow-up time required to determine permanent parathyroid function after thyroidectomy. Some studies have reported25,26 that in patients with permanent HP after total thyroidectomy, there are still some patients with gradual recovery of parathyroid function, which was also found in our study. There were 2 patients with total thyroidectomy who returned PTH to normal range after 1 year in our study, primarily because the delayed recovery of parathyroid function may be due to the slow formation of neovascularization on the surface of residual parathyroid gland, so the diagnosis of permanent HP should also be cautious. The diagnosis of permanent HP implies lifelong medical care, increases the economic burden, and affects the quality of life of the child.
Conclusions
Children with thyroid cancer are in the period of growth and development, with a long survival time, and the influence of HP is more serious and long-term, which should be widely concerned. Due to the wide range of invasion and high rate of lymph node metastasis in pediatric thyroid cancer, it is difficult to identify the parathyroid glands, and more meticulous protection is needed. The recovery time of HP is closely related to the level of PTH≤1 on the first postoperative day. It is necessary to be cautious about the diagnosis of permanent HP in children because HP may recover after 1 year.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Beijing-Tianjin-Hebei Integration Project (No. J200004) and National Natural Science Foundation of China (No. 82271184).
Statement of Ethics
The study was conducted in accordance with the principles of the Declaration of Helsinki, and the study protocol was approved by the ethics committee of Beijing Children's Hospital (reference number: 2019-k-400). We obtained written parental consent for the minors before the study was begun.