
Abstract
Spindle epithelial tumor with thymus-like differentiation of thyroid (SETTLE) is very rare neoplasm with 2 cellular forms, epithelial cell and spindle cell, and most reported cases have been in young people. An 11-year-old boy presented with painless swelling of the right neck lasting for more than 2 months. A tumor size measuring approximately 3 × 3 cm was resected, and intraoperative frozen pathology suggested a spindle cell tumor, which was confirmed as SETTLE by immunohistochemical staining and external hospital consultation. The immunohistochemical staining profile of the resected tumor tissue was as follows: cytokeratin (CK) (+), smooth muscle actin (weak+), vimentin (+), CK7 (focal+), B-cell lymphoma 2 (partial+), CD99 (−), calcitonin (+), galectin-3 (+), CK19 (+), and Ki-67 (10%+). Ultrasound at 1-year postoperative follow-up revealed no local recurrence of the lesion or lymph node metastasis in the thyroid gland. We summarized the disease characteristics of SETTLE among 6 cases reported to date and found that SETTLE is associated with a good prognosis and low postoperative recurrence rate. Thus, for this type of malignant thyroid tumor, diagnosis depends mainly on postoperative pathology and immunohistochemical staining and simple surgical resection is recommended.
Introduction
Spindle epithelial tumor with thymus-like differentiation of thyroid (SETTLE) is a very rare malignant tumor that is also known as a spindle cell tumor of the thyroid with mucocele, malignant teratoma, and thyroid thymoma in children. 1 It usually occurs in young adults or children. SETTLE is a lobulated tumor that is usually limited by the capsule of the fibrous septum. Morphologically, it consists primarily of spindle cells and epithelial cells. The epithelial cells can form tubules with mucocele cysts, small papillae, trabeculae or squamous nests. 1 Miyauchi et al 2 first reported this disease in 1985, referring to it as intrathyroid epithelial thymoma originating from the ectopic thymus tissue of the thyroid gland with main clinical manifestations of neck enlargement and hoarseness. According to specific clinical and pathological characteristics, Chan and Rosai 3 categorized intrathyroid epithelial thymoma into 4 types: ectopic hamartoma thymoma, ectopic cervical thymoma, SETTLE and thyroid carcinoma showing thymus-like differentiation (CASTLE). The first 2 tumor types are considered benign, and the latter 2 are considered malignant. Although CASTLE is also rare in clinical practice, nearly 100 cases have been reported to date, whereas far fewer cases of SETTLE have been documented. The present case report and literature review aim to contribute to the understanding of the characteristics, treatment, and prognosis of SETTLE.
Case Report
An 11-year-old boy was admitted for a suspected thyroid tumor after developing a large painless mass on the right thyroid that persisted for more than 2 months. Approximately 2 months before admission, a classmate of the patient accidentally discovered local swelling on the right side of the center of the patient’s neck. The mass measured approximately 3 × 4 cm, and no local redness, tenderness, ulceration, bleeding, local restraint, or discomfort upon neck movement was reported. The boy was taken to a local hospital, ultrasound of the neck showed a nodule in the right lobe of the thyroid classified as TI-RADS: 4a. Then ultrasound examination of the thyroid gland in the Affiliated Hospital of Jiangsu University revealed a mass measuring 34 × 17 mm mass beside the right lobe of the thyroid gland. Enhanced computed tomography (CT) of the neck showed: nodules in the right lobe of the thyroid (nature to be determined), a nodular shadow under the left lobe of the thyroid (ultrasound and other examinations needed to clarify its source and nature); multiple nodular lymph nodes in the bilateral neck (indicating possible reactive hyperplasia); and slight thickening of the anterior superior mediastinal tissue (mostly undegraded thymic tissue). On the same day, a puncture specimen from the right thyroid mass showed spindle cell proliferative, suggesting tumorigenicity and not excluding low-grade malignancy. Thus, complete excision of the mass was recommended. Thereafter, the patient’s family came to our hospital for further treatment.
After 11 days, our hospital performed total thyroidectomy on the right side and isthmus under general anesthesia as well as lymph node dissection in the central region. Intraoperatively, a tumor approximately 3 × 3 cm in size was seen in the upper part of the right lobe of the thyroid (Figure 1). The thyroid capsule was intact, and the boundary with surrounding tissues was clear. No obvious adhesion was found, and the left thyroid did not touch the nodule and tumor. Several lymph nodes were seen in the central region, with soft and clear boundaries. Thorough resection of the right lobe thyroid and isthmus was performed, and the central lymph nodes were removed. Based on the postoperative pathology of the tumor from the right lobe of the thyroid, multiple experts at the Shanghai Clinical Pathology Reading Conference reviewed the hematoxylin and eosin staining as well as immunohistochemical staining and agreed that the primary lesion was a spindle cell tumor accompanied by 8 positive lymph nodes and no tumor metastasis. The results of immunohistochemical staining were: (2021IM0759) CK (+), smooth muscle action (weak+), desmin (−), vimentin (+), myogenin (−), myoblast determination protein 1 (−), S100 (−), synuclein (−), glycoprotein hormone, alpha polypeptide (CgA) (−), carcinoembryonic antigen (CEA) (−), CK7 (focal+), B-cell lymphoma 2 (partial+), CD99 (−), calcitonin (+), thyroglobulin (−), thyroid transcription factor-1 (−), galectin-3 (+), CK19 (+), and Ki-67 (10%+). The final diagnosis of SETTLE was confirmed by the Department of Pathology of Shanghai Fudan University Affiliated Cancer Hospital (Figure 1). (A, B) Images of the resected tumor. (C) Hematoxylin and eosin staining (magnification, ×40) of the tumor tissue showing fusiform cellular arrangement, loose clusters, dysplasia, hyperchromatic nuclei, and obvious nucleoli. (D) Immunohistochemical staining of the tumor tissue for CK19 (+) (magnification, ×40).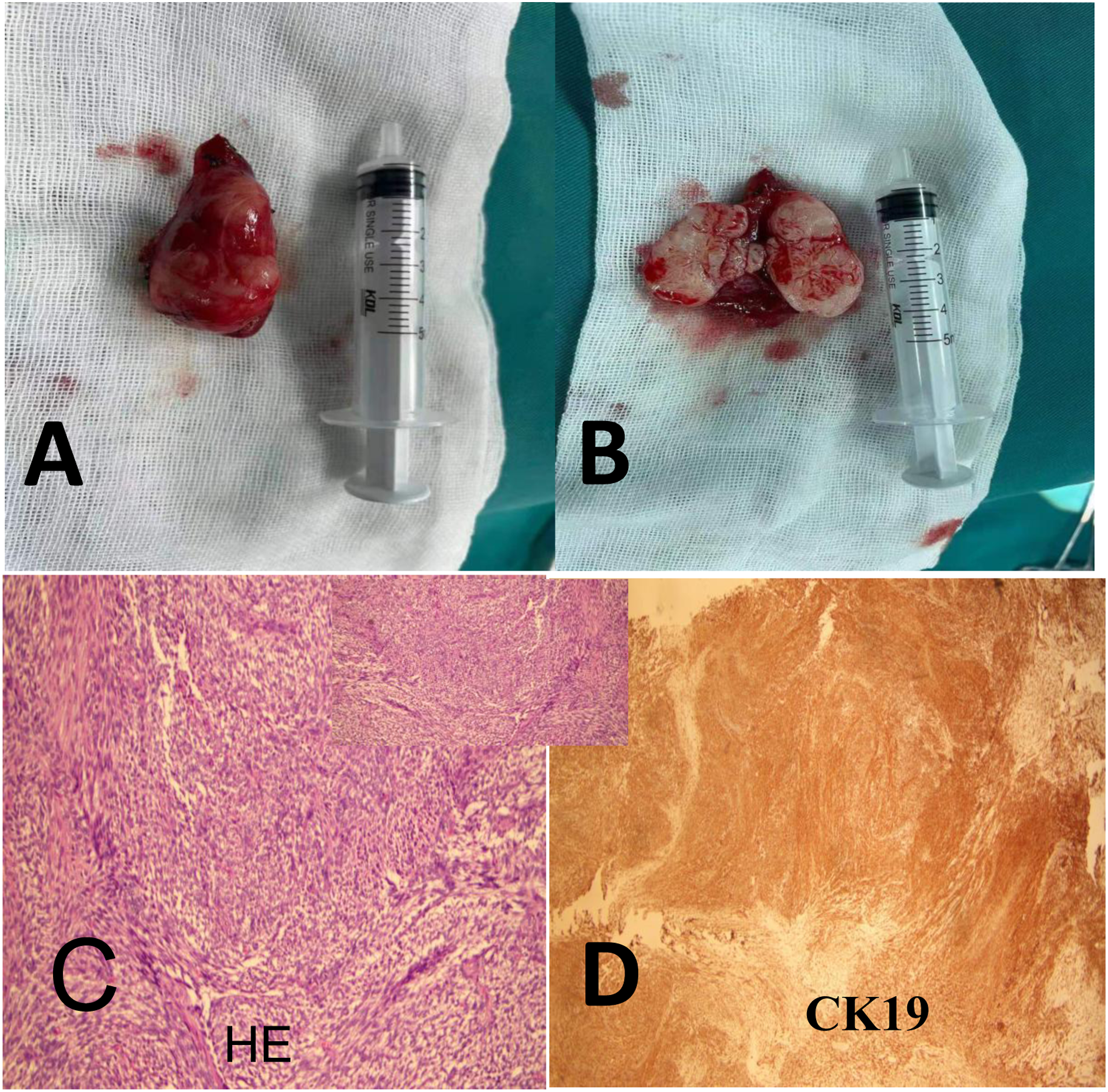
At follow-up more than 1 year after surgery, the patient had normal thyroid function and electrolyte levels and reported no discomfort. Ultrasound revealed no local recurrence of the lesion or lymph node metastasis in the thyroid gland.
Literature Review
Characteristics of SETTLE Cases Reported in the Literature.
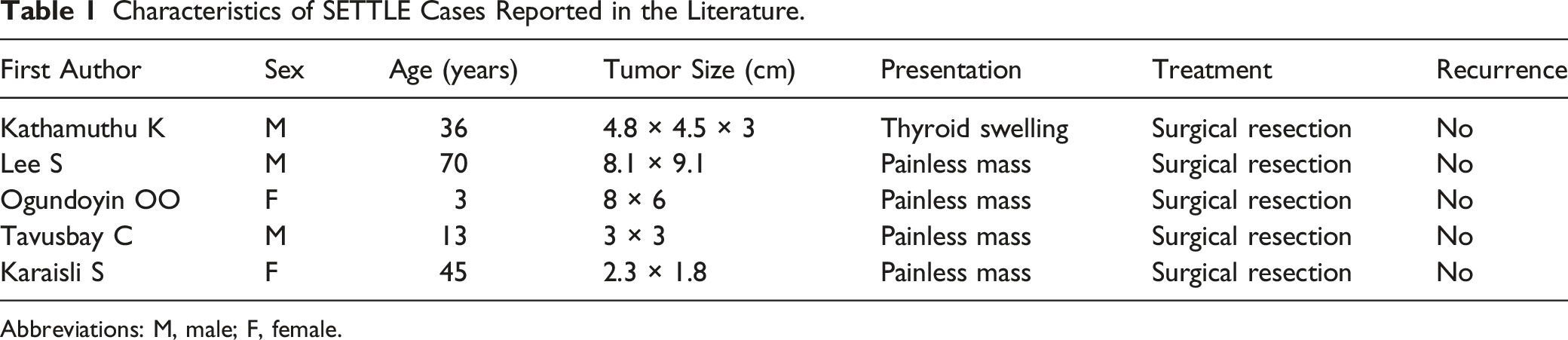
Abbreviations: M, male; F, female.
Discussion
To date, few reports on SETTLE have been published. The present case along with the 5 cases identified in our literature review shared the characteristics of a painless mass on the thyroid, and all cases were treated with surgical resection only, with none experiencing recurrence. Together these cases indicate that SETTLE is associated with a good prognosis and low postoperative recurrence rate. The patients in the previously reported cases were between 3 and 70 years old, and from these cases together with the present case, we did not observe an increased incidence rate of SETTLE among children compared with adults.
Unlike for SETTLE, the current literature includes many reports of a similar thyroid tumor type, CASTLE, that involve thymus-like differentiation in the thyroid gland. Accurate diagnosis of SETTLE or CASTLE requires differentiation from primary or secondary thyroid tumors. Careful preoperative examination is important for the diagnosis of this disease, including neck ultrasound, neck CT, neck magnetic resonance imaging, and fine needle aspiration cytology. 9 Ultrasound findings for the more common CASTLE include a solid hypoechoic mass with typical uneven echo, and plain scan CT generally shows a soft tissue mass with an unclear boundary and no calcification that appears enhanced upon administration of contrast agent. A previous study reported that CASTLE appears as a “cold nodule” on CT. 10 On MRI, CASTLE shows uniform intensity on T1-weighted imaging and slightly higher intensity on T2-weighted imaging. 11 Fine needle aspiration cytology plays an important role in the diagnosis of all types of thyroid cancer. However, a disadvantage is that cytology cannot distinguish thyroid cancer with thymus-like differentiation from poorly differentiated thyroid cancer, such as squamous carcinoma or undifferentiated thyroid cancer. The final diagnosis of CASTLE depends on postoperative pathology and immunohistochemistry. Typical immunohistochemical results include positive staining for CD5, CD117, CK19, epithelial membrane antigen, and tumor protein 63 and negative staining for calcitonin, thyroglobulin, and thyroid transcription factor-1. 10 Two reports emphasized that positive staining for CD5, an established marker of thymic cancer, has important diagnostic significance.3,9
Due to the small number of SETTLE cases reported so far, there is no consensus regarding its treatment. For CASTLE, radical resection of the tumor and selective neck dissection are the main treatment methods currently and have been shown to provide local control and long-term survival. 12 For patients without cervical lymph node metastasis, simple surgical resection is not associated with tumor recurrence. For patients with cervical lymph node metastasis, surgical resection combined with postoperative intensity-modulated radiotherapy was shown to provide satisfactory local-regional control for CASTLE with acceptable toxicity, reducing the recurrence rate from 100% to 57%. 13 It has also been reported that palliative conservative treatment and follow-up are an option for patients who experience relapse and have difficulty undergoing surgery again.9,14 Dang et al 9 reported a case of CASTLE in a 60-year-old woman who underwent total thyroidectomy and experienced relapse after 5 years. Upon relapse, the disease was in a late stage and not suitable for surgical resection. The patient refused radiotherapy, and without intervention, her condition remained stable after 15 months of follow-up. Dualim et al 14 reported a case of CASTLE in which the thyroid tumor was compressing the airway, and although no adjuvant therapy such as radiotherapy and chemotherapy was administered after surgical resection, the patient did not feel unwell during continuous follow-up.
We can first learn from the treatment methods used for CASTLE in determining appropriate treatments for SETTLE. Then as more SETTLE cases are reported, patient information collected during the treatment process can be analyzed, with specific attention given to the postoperative treatment of patients, to explore future treatment standards for SETTLE.
Conclusions
SETTLE and CASTLE are malignant tumors of the thyroid gland belonging to the intraepithelial thymoma type of thyroid cancer. In the current literature, more than 100 cases of CASTLE have been reported, whereas very few SETTLE cases have been reported and none in China. The patient in the present case was 11 years old, which is a relatively young age of onset among the reviewed cases. The primary symptom in this case was neck swelling. No cervical lymph node metastasis was found during surgery, and the patient did not receive postoperative radiotherapy. The patient’s condition remained stable 1 year after the operation. We will continue to follow up this case to determine the prognosis of the patients and provide updated information for this case.
Footnotes
Acknowledgment
We thank Medjaden Inc. for scientific editing of this manuscript.
Declaration of Conflicting Interests
The author(s) declare there are no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclose receipt of the following financial support for the research, authorship, and/or publication of this article: the Subject Construction Project of Pu dong Health Committee of Shanghai (Grant No. PWZy2020-06), Research Grant for Health Science and Technology of Pudong Health Bureau of Shanghai (PW2019D-4), and Key Specialty Construction Project of Health Bureau of Shanghai (ZK2019C06).
Informed Consent
The patient’s parents provided written informed consent for the publication of their son’s anonymized information in this article.
Data Availability
All data generated or analyzed during this research are included in this published article. Data supporting the findings of this study are available from the corresponding author upon reasonable request.