
Abstract
Skip metastasis in thyroid cancer occurs when there is lateral neck lymph node involvement of tumor without central neck lymph node involvement. Here, cancer spreads to the lateral neck while “skipping” more proximal central neck nodes. While this unusual pattern of spread has been previously described in adults with thyroid cancer, to our knowledge it has never been described in children. Here, we report a case of an adolescent female with medullary thyroid cancer with isolated lateral neck metastatic disease. In summary, a 15-year-old female with no medical conditions presented with an asymptomatic neck mass. A computed tomography (CT) scan of the neck showed a heterogenous nodule in the right thyroid lobe with both cystic and solid components which were also illustrated on ultrasound. There was no CT evidence of metastatic disease, but a thyroid and cervical neck ultrasound showed a <1 cm calcified nodule in right neck level II concerning for metastasis. Fine needle aspiration highlighted medullary thyroid cancer. The patient underwent total thyroidectomy with both central and right lateral neck dissection. Central neck dissection revealed no metastatic lymph nodes, while metastatic nodes were found with right lateral neck dissection, highlighting skip metastasis. The patient had an uneventful postoperative course and was well at 1-month follow-up with a strong voice and no dysphagia.
Introduction
Medullary thyroid carcinoma (MTC) is a subtype of thyroid cancer which arises from the parafollicular cells of the thyroid gland. It has an incidence in children of 0.03 per 100,000, with the majority of cases being hereditary. 1 Patients with MTC often present with cervical lymph node metastasis, with estimates ranging from 25% to 63%. 2 The sequence of regional lymphatic spread typically occurs in a stepwise fashion, spreading first to the central neck lymph nodes (CLN) followed by the ipsilateral lateral neck lymph nodes (LLN). Contralateral lateral neck metastasis may occur as well following this.
Skip metastasis occurs when there is evidence of LLN involvement without CLN involvement. This phenomenon has an incidence of 1.6% to 21.8% in adult patients with thyroid cancer and has been described in both papillary [papillary thyroid carcinoma (PTC)] and medullary (MTC) subtypes in adults. 3 However, it has not been described in children with thyroid cancer. Here, we report a case of a pediatric patient with MTC who presented with skip metastasis.
Case Presentation
An otherwise healthy 15-year-old female presented to her local hospital with a 1-month history of an asymptomatic neck mass. She had no past medical history and was not taking any medications. Family history was notable for a second-degree relative on the father’s side who had both thyroid and adrenal cancer in the past. However, no further information was known by the patient’s family regarding this.
Physical examination revealed a right-sided thyroid nodule, which was approximately 2 × 2 cm, with no overlying skin changes. There was no palpable cervical lymphadenopathy.
Laboratory tests revealed an elevated calcitonin (9597 pg/mL) but normal TSH (1.18 mcIU/mL), free T4 (1.0 ng/dL), thyroid peroxidase (<3 IU/mL), and thyroid-stimulating immunoglobulins (<89% basal activity). A computed tomography (CT) scan of the neck showed a 2 × 2 × 3 cm heterogenous nodule with both cystic and solid components in the right thyroid lobe with coarse internal calcifications, which was also illustrated on ultrasound (Figure 1). There was no CT evidence of metastatic disease in the neck, but a thyroid and cervical neck ultrasound showed a <1 cm calcified nodule in right neck level II concerning for metastasis. Fine needle aspiration of the thyroid mass revealed MTC.
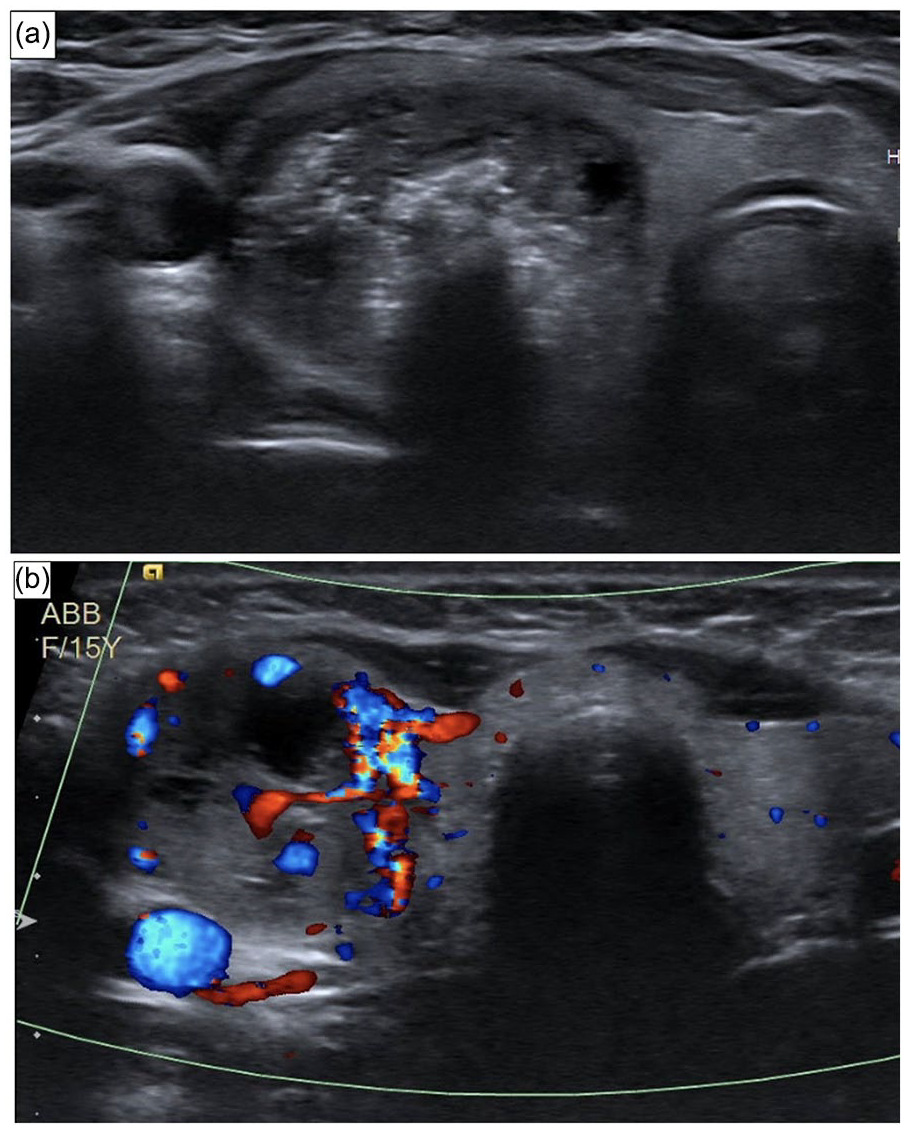
(a) Plain and (b) Doppler ultrasound images illustrating the right thyroid mass.
Genetic testing revealed a pathological variant of the RET gene (Cys634Sert mutation), consistent with a predisposition to RET-related conditions such as multiple endocrine neoplasia 2a (MEN2a). Further CT scans of the chest and abdomen revealed no evidence of metastasis. The patient and her family were counseled on treatment options and elected to proceed with surgical management.
In the operating room, the patient underwent total thyroidectomy with both central and right lateral neck dissection (levels II-IV) due to her elevated calcitonin levels and ultrasound findings of a metastatic lymph node in right level II. Pathology showed T2N1b MTC with negative margins, with the largest focus measuring 3.3 cm. There was no evidence of tumor necrosis, angioinvasion, lymphatic invasion, or extrathyroidal extension. Central neck dissection yielded 5 lymph nodes that were all negative for malignancy; right level II neck dissection yielded 18 lymph nodes, 1 of which was involved by MTC; right level III neck dissection yielded 6 lymph nodes, 2 of which were involved with MTC; right level IV neck dissection yielded 7 lymph nodes that were all negative for malignancy.
The patient had an uneventful postoperative course with normal parathyroid hormone and calcium. She was evaluated in clinic 1 month after surgery and was found to be well with strong voice, no dysphagia, and only taking levothyroxine medication. Postoperative labs were notable for normalized calcitonin (5.5 pg/mL). No adjuvant therapy was indicated. She continues to be followed for her new diagnosis of MEN2a.
Discussion
In this report, we describe a pediatric patient with thyroid cancer who presented with skip metastasis. While this phenomenon has been reported in adult patients with thyroid cancer, to our knowledge, it has not been described in pediatric patients. Pediatric thyroid cancer is a rare disease with an annual incidence of 1.14 per 100,000. 4 A majority of cases are PTC, with an incidence of around 1 per 100,000, while MTC is much rarer, with an incidence of 0.03 per 100,000.1,4 As a result, skip metastasis in a pediatric patient with MTC represents a rare phenomenon in a rare group.
Skip metastasis refers to lateral lymph node involvement on the side of the tumor without central lymph node involvement. In our patient, CT imaging of the neck revealed no evidence of metastatic disease, although there was concern for involved lateral neck metastasis in level II of the right neck seen on ultrasound. Notably, our patient had a highly elevated calcitonin. The American Thyroid Association guidelines recommend performing elective neck dissection if calcitonin is elevated. 5 As such, although there was ultrasound evidence of a metastatic node in this case, we would have performed a neck dissection regardless due to her significantly elevated calcitonin. Pathological examination of specimens following thyroidectomy and neck dissection revealed the presence of metastatic nodes in levels II and III with no central node involvement.
The decision to perform elective or prophylactic neck dissection in MTC is controversial. Some studies in adults have shown no decrease in overall survival in those who do not undergo elective neck dissection, but some note a trend in the rate of lateral neck recurrence and need for reoperation, suggesting that there is possibly a high-risk group, including younger patients with familial disease, who are more likely to benefit from a more aggressive approach to treating the lateral neck.6-8 By contrast, prophylactic neck dissection is not recommended in patients with PTC with no clinical evidence of nodal disease. 9 Of note, both MTC and PTC have been shown to behave similarly in their mechanism of metastatic spread, disseminating primarily through the lymphatic system and displaying early metastatic involvement of local neck nodes. 10 Data from adult populations have shown similar rates of skip metastasis in both PTC and MTC, 11 with no significant differences in the characteristics of skip metastases between these subtypes.
Cadaveric studies have provided possible mechanisms for skip metastases.12,13 These studies identified additional lymphatic vessels that travel with branches of the superior thyroid artery, bypassing the central lymph nodes directly to the lateral cervical lymph nodes. However, in our patient, the thyroid carcinoma was located in the midportion of the right thyroid lobe. Nevertheless, shared lymphatic drainage from this region proceeding along the superior pathway could have contributed to the skip metastasis. Our patient also did not have other potential risk factors for skip metastasis, such as a primary tumor size of < 1 cm. 14
It has been suggested that the phenomenon of skipped metastasis could be due to sampling error, leading to false negative results on pathological analysis.15,16 However, this has been suggested mainly in the context of esophageal and gastric cancer, where it is anatomically more difficult to fully clear lymph node compartments. In thyroid cancer, compartment-directed lymph node dissection is more amenable, allowing fuller inspection and clearance of lymph nodes at each neck level. As a result, it has been suggested that sampling error here is less likely to account for skip metastasis. 17 Further studies including larger case series will be useful in calculating the prevalence of this phenomenon in pediatric patients.
Conclusion
This study highlights the occurrence of skip metastasis in a pediatric patient with MTC. While this phenomenon has been characterized in adult patients with MTC, it has seldom been reported in pediatric patients. Surgeons should keep in mind the possibility of this phenomenon when evaluating pediatric patients with MTC.
Footnotes
Acknowledgements
None.
Author Contributions
All listed authors made:
• Substantial contributions to the conception or design of the work; AND
• Drafting the work or revising it critically for important intellectual content; AND
• Final approval of the version to be published; AND
• Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data Availability Statement
Data are available for scientific researchers upon reasonable request through the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. IRB review was exempt from our institution.
Informed Consent/Patient Consent
Written informed consent from the patient’s legally authorized representative was obtained for the patient’s anonymized information to be published in this article.
Trial Registration Number/Date
Not applicable.
Grant Number
Not applicable.