
Abstract
Angiofibrolipomas are rare, benign soft tissue tumors composed of mature fat cells, blood vessels, and fibrous connective tissue. Typically occurring in subcutaneous locations, this case report presents a unique instance of an angiofibrolipoma arising in the pharynx. According to our review of the literature, it is the second reported case in the pharynx and the sixth in the head and neck region. A 58-year-old woman presented with a 1 year history of globus sensation and an incidentally-discovered extra-oral polyp. Endoscopic examination revealed the polyp originating from the upper esophagus and extending into the pharynx. Magnetic resonance imaging confirmed the nature and extent of the lesion. The polyp was successfully removed via endoscopic resection, and histopathological analysis confirmed the diagnosis of angiofibrolipoma. This case highlights the rarity of pharyngeal angiofibrolipomas and underscores the importance of endoscopic evaluation for patients presenting with ambiguous pharyngeal symptoms. While surgical resection is generally recommended for such tumors, endoscopic removal can be a safe and effective option for smaller pedunculated lesions.
Introduction
Lipomas, the most prevalent mesenchymal neoplasms of soft tissue among adults, are benign tumors comprised of mature white fat cells. 1 These growths are typically encapsulated by a thin fibrous layer, distinguishing them from the surrounding tissues. 1 Lipomas can develop anywhere in the body where adipose tissue is present, with the subcutaneous layer just beneath the skin being the most frequent site.1,2 About 13% of lipomas are found in the head and neck region. In the oral cavity, lipomas account for 0.5% to 5% of all benign growths and may occur in areas such as the major salivary glands, buccal mucosa, lips, tongue, palate, vestibule, and floor of the mouth. 3 Clinically, lipomas present as slow-growing, well-defined, movable, and painless nodules. These lesions predominantly affect individuals over the age of 40. 3 The World Health Organization classifies adipocytic tumors such as lipomas based on clinical and histopathological characteristics into several subtypes, including classic lipoma, angiolipoma, chondroid lipoma, myolipoma, and spindle cell/pleomorphic lipoma.1,4 Histological variations of lipomas are further categorized as fibrolipomas, angiolipomas, angiofibrolipomas, angiomyolipomas, and infiltrating angiolipomas. This classification hinges on the proportion and interaction of fat cells, muscle fibers, blood vessels, and connective tissues within the tumor. 4 Angiofibrolipomas consist of a mixture of mature adipocytes, vascular components, and collagen-rich connective tissue. Representing the rarest subtype, angiofibrolipomas usually appear as solitary, well-defined subcutaneous masses located on the back, neck, or shoulders. 5 Histologically, these tumors, though not encapsulated, are clearly distinct from surrounding tissues. 5 They exhibit low-to-moderate cellular density and typically do not display aggressive clinical behavior. 5 In this report, we present a rare case of angiofibrolipoma in the pharynx, which is the second case documented at this site according to our literature review.
Case Presentation
A 58-year-old woman presented to ENT clinic with globus sensation for a 1 year duration and incidental extra-mouth emerging polyp after vomiting. There was no otalgia, weight loss, or anemia. No history of smoking or radiation. Esophagoscope revealed the polyp originating from the upper right level of the upper esophagus sphincter and occupying approximately the upper two-thirds of the esophagus (Figure 1). MRI with gadolinium showed the nature and extent of the lesion (Figure 2). Then, the patient was prepared for endoscopic resection of the lesion. Rigid esophagoscopy has been used to visualize and exteriorize the distal end of the polyp to the pharynx. by using rigid hypopharyngoscopy, bipolar cautary cut the rout of the polyp (Figure 3). NGT has been inserted and the patient discharged at the same day. Oral naturation was returned after continuing the NGT for 5 days. The histological examination showed angiofibrolipoma (Figure 4).
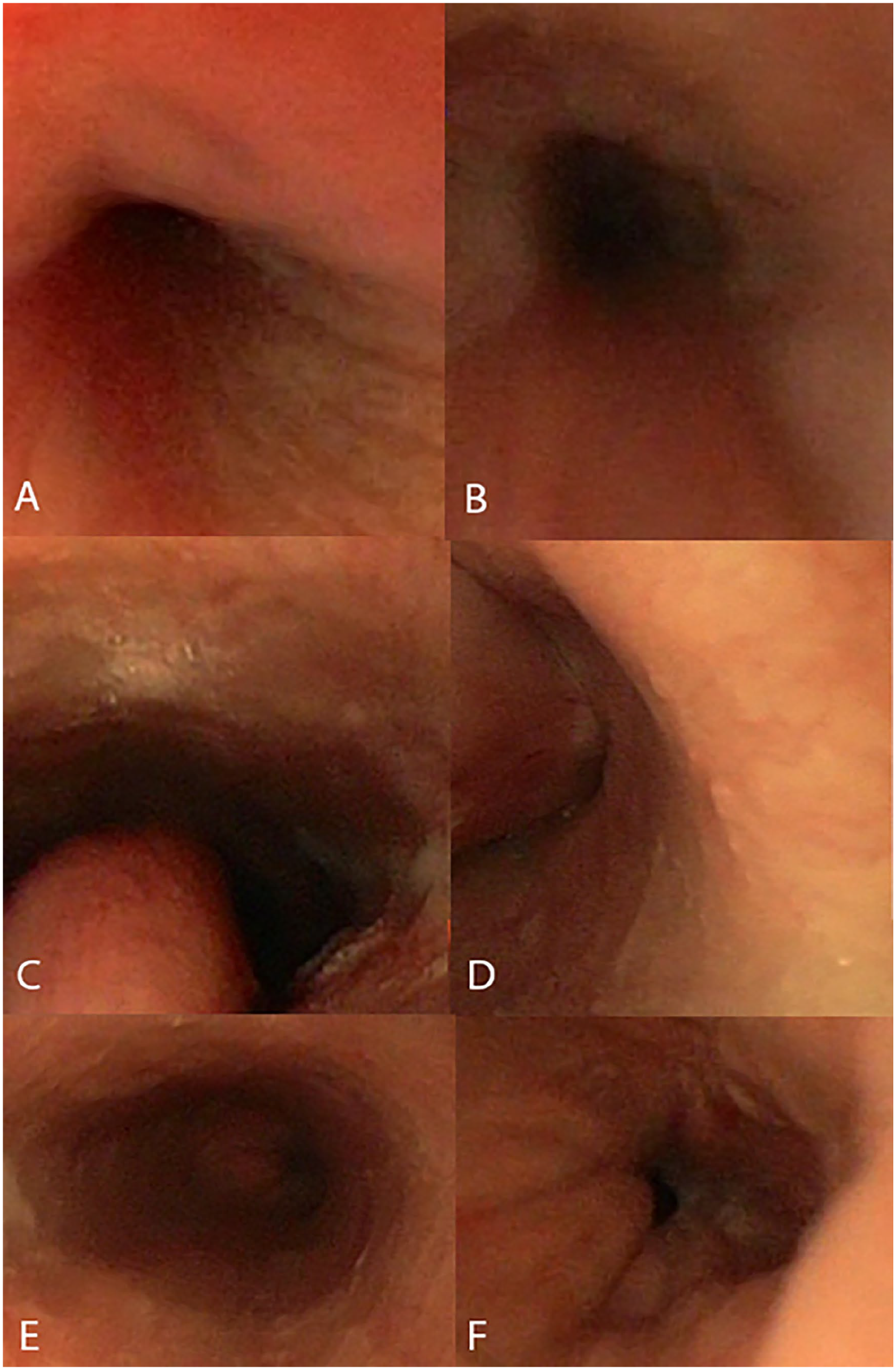
Esophagoscopy showing (A) and (B) the upper esophagus sphincter, (C) and (D) the intra-esophagus polyp, and (E) and (F) the lower esophagus sphincter.
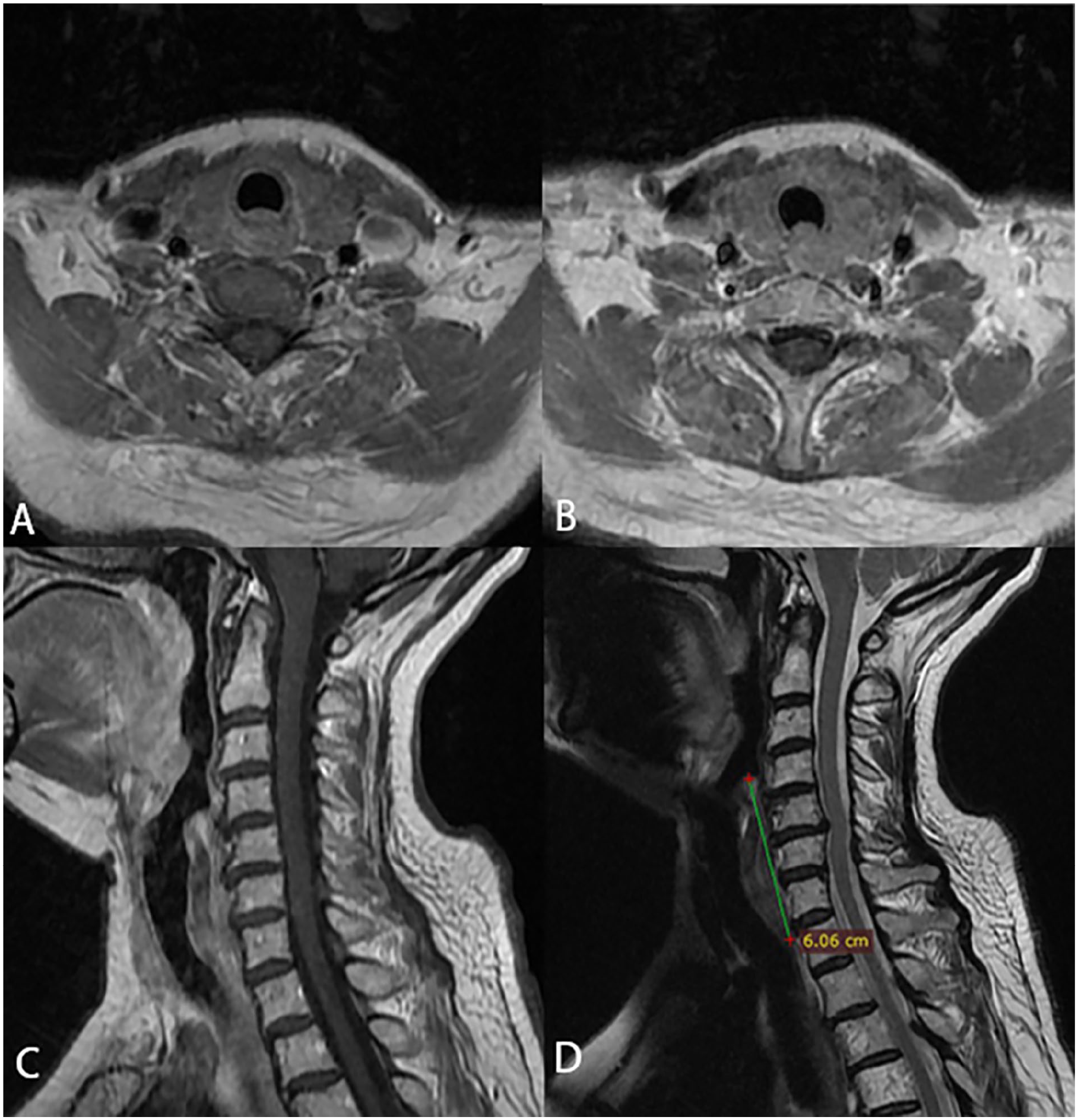
MRI to the head and neck (A) axial postgadoliniumT1-wighted image and (B) a more inferior level show a soft tissue mass filling the upper esophagus, (C) sagittal postgadolinium T1-wighted image demonstrates a homogeneous enhancement with rim-enhancing low-to-intermediate signal intensity lesion, and (D) T2-wieghted image manifests a low-to-intermediate signal intensity lesion involving the upper esophagus and measures 6.06 cm. There is a bright focal signal intensity on T1 and T2 images at the superior section of the lesion.
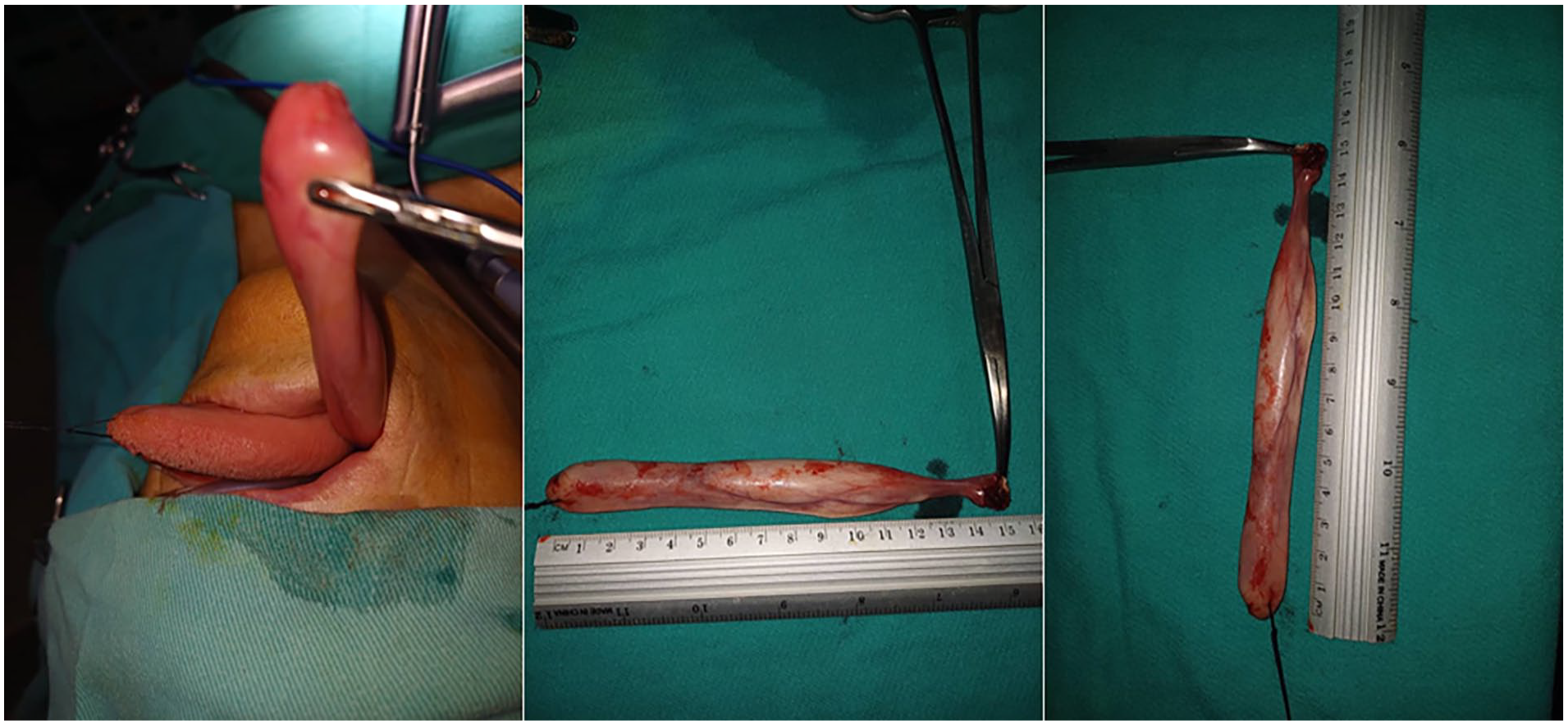
Intraoperative polyp measures 15 cm.

Gross description: a moderately-firm white polypoid piece measuring 9.5 cm × 2.5 cm. Histological study reveals regular squamous epithelium lining this formation. The stalk is composed of variably-sized blood vessels associated with fibroblastic and adipose stroma showing mature adepocytes. No atypia and no mitotic figures. Esophago-pharyngeal polypoid formation revealing angiofibrolipoma. No malignancy.
Discussion
Despite their benign nature, angiofibrolipomas present a complex pathology due to their rarity and unique histological composition. The literature suggests that the development of angiofibrolipomas may be influenced by the interplay of mesenchymal elements, particularly vascular and fibrous tissues, with adipocytes. In the case of head and neck tumors, such as the one presented here, the rarity of these lesions adds complexity to both diagnosis and treatment decisions. The potential for misdiagnosis with more common soft tissue masses, such as simple lipomas or even malignant liposarcomas, necessitates thorough imaging and histopathological examination. Benign lipomas, which are commonly found in soft tissues, can undergo changes due to the incorporation of various mesenchymal components. 5 The most frequently-encountered combination involves fibrous connective tissue, leading to the development of a fibrolipoma. 5 Among the rarest forms of lipomas is the angiofibrolipoma, a subtype that was first characterized by Kershisnik and colleagues in 1986. 6 The underlying cause of angiofibrolipoma, like that of many other tumors, remains unidentified. While some studies suggest that hamartomas have a polyclonal origin, which contrasts with the monoclonal nature typical of true neoplasms, there is still debate in the literature about classifying angiofibrolipoma as a hamartoma. 7 Some studies suggest that angiofibrolipomas may be hamartomas, benign malformations of tissue that contain cells from multiple tissues. This theory is supported by the polyclonal nature of these tumors, which differs from the monoclonal nature of true neoplasms. Alternatively, angiofibrolipomas could be considered neoplastic, arising from abnormal cell proliferation. This view is supported by their ability to grow and expand, as well as their potential for recurrence in rare cases. 6 Furthermore, lipomatous tumors originating from the hypopharyngeal are considered exceedingly uncommon.
In the medical literature, more than a dozen instances of angiofibrolipoma have been documented across various anatomical sites. Within the realm of otolaryngology, only 6 cases have been identified: 1 in the external auditory canal, 8 2 involving the palatal tonsils,9,10 1 in the larynx, 11 and 2 in the pharynx 12 (including the case presented here). Both cases of angiofibrolipoma in the pharynx (our case and the other case) originated from the lower part of the pharynx (hypopharynx). Both were excised endoscopically without any complications during or after surgery, and there has been no subsequent evidence of recurrence. As we observed, both cases originated from the hypopharynx at a level higher than the upper esophageal sphincter. This could possibly be explained by the presence of a relatively high percentage of fat in this region as a potential factor.
For angiofibrolipomas located in the throat, a radical surgical resection is generally recommended. Tumors that are large and have a broad base often necessitate an external surgical approach. Conversely, smaller tumors with a slender pedicle can typically be excised transorally, which is linked to a reduced risk of complications. 12 In the case presented, an endoscopic procedure, known for being both straightforward and safe, also proved to be effective. When considering the diagnosis of an angiofibrolipoma in the head and neck region, it is crucial to differentiate it from other benign and malignant lesions. While both angiofibrolipomas and lipomas are benign tumors composed primarily of fat cells, angiofibrolipomas contain additional vascular and connective tissue components. Imaging studies, such as MRI or CT scans, can help differentiate these 2 entities based on their unique characteristics. Liposarcomas, malignant tumors that can resemble lipomas, often exhibit more aggressive features such as rapid growth, pain, and other symptoms. Histological examination is essential for definitive diagnosis. Hemangiomas are benign vascular tumors that can occur in the head and neck region. While they may resemble angiofibrolipomas, hemangiomas typically consist primarily of blood vessels without a significant component of adipose tissue. Imaging studies and histological examination can help distinguish between these 2 entities. Schwannomas are benign tumors derived from Schwann cells, which surround nerve fibers. They can occur in the head and neck region, particularly in the cranial nerve pathways. Imaging studies and histological examination can help differentiate schwannomas from angiofibrolipomas. 11
In head and neck cases, including those arising in the pharyngeal region, MRI is essential to determine the extent of the tumor and its relationship with surrounding structures. MRI, particularly with gadolinium contrast, allows for detailed characterization and circumscription of these tumors, which can be crucial in planning the surgical approach. As demonstrated in this case, a minimally-invasive endoscopic resection was both safe and effective. Preoperative CT scans are useful in distinguishing between a lipomatous process and a laryngocele by analyzing the tumor’s density. However, accurately differentiating between a lipoma and a liposarcoma using CT imaging alone presents a significant challenge. 13 In the presented case, histopathological analysis was essential to confirm the diagnosis of angiofibrolipoma. Although the tumor was identified as benign, consistent and extended postoperative monitoring was advised due to the potential risk of recurrence or malignant transformation. Large pedunculated tumors originating in the pharynx can go unnoticed for an extended period. Often, the only sign of their presence is mild difficulty swallowing. Prompt identification of such tumors is crucial, as it allows for timely intervention and helps avert potentially-fatal complications such as choking. The management of angiofibrolipomas in the head and neck region depends on the clinical course of the tumor as well as the patient tolerance of the tumor. In general, surgical resection is the preferred treatment option. 12 However, the choice of surgical approach may vary depending on the specific characteristics of the tumor and the patient’s anatomy. For smaller, well-defined tumors, endoscopic resection may be a suitable option, as demonstrated in the presented case. This approach can often be performed with minimal morbidity and a low risk of recurrence. However, larger or more complex tumors may require open surgical excision. 4 Postoperative follow-up is important to monitor for recurrence, which is rare but possible. Regular clinical examinations and imaging studies can help detect any signs of recurrence or other complications. Histopathological confirmation remains the gold standard for diagnosis. The presence of mature adipocytes intermixed with collagenous stroma and well-formed blood vessels, as described in this case, clearly points toward angiofibrolipoma. Such findings are essential to differentiate these tumors from other lipomatous lesions with a more aggressive course, such as spindle cell lipomas or atypical lipomatous tumors .
Further research is needed to elucidate the exact etiology and pathogenesis of angiofibrolipomas. Additionally, studies investigating the long-term outcomes of different treatment approaches, including endoscopic resection and open surgery, would be valuable. This information could help guide clinical decision-making and improve patient care.
Conclusion
This case report presents a rare occurrence of an angiofibrolipoma arising in the pharynx, a site not commonly associated with this benign soft tissue tumor. Despite the rarity of this presentation, the endoscopic management of the lesion highlights an appropriate treatment approach for this tumor. In addition to indicating the importance of nonspecific pharyngeal symptoms; surgical resection remains the gold standard for angiofibrolipomas, and endoscopic removal can be a safe and effective option for smaller pedunculated tumors, as demonstrated in this case. Continued follow-up is essential to monitor for potential recurrence or malignant transformation, even in benign cases.
Footnotes
Data Availability Statements
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethics approval for reporting individual cases. Written informed consent was obtained from the patient for publication of this article.