
Abstract
Keywords
Introduction
Liposarcomas are rare mesenchymal tumors that infrequently occur in the head and neck region, accounting for only 2% to 9% of malignant mesenchymal tumors in this area. 1 This rarity makes each case an essential contribution to the existing medical literature. The most affected sites within the head and neck are the neck, larynx, and pharynx. 1 These tumors primarily afflict middle-aged men, typically between the ages of 50 and 65. While the exact etiology of liposarcoma development remains unclear, certain factors, such as trauma, radiotherapy, and genetic predisposition, may elevate the risk of occurrence. 1
Generally, liposarcomas tend to be asymptomatic, but they can become problematic due to their slow enlargement. In some cases, patients may experience dyspnea if the tumor’s growth obstructs the airway. Liposarcomas typically manifest as firm, well-defined masses, with most not exceeding 10 cm in size; those larger than 10 cm are classified as giant tumors. 2
Treatment and prognosis for liposarcomas can vary depending on the histologic subtype. The World Health Organization classifies liposarcomas into several subtypes, including well-differentiated, myxoid, round-cell, dedifferentiated, and pleomorphic types. 3 Recent data have considered well-differentiated liposarcoma (WDL) and atypical lipoma as synonymous. 4 Among these subtypes, WDL is the least aggressive; however, approximately 10% of recurrent WDL cases may progress to dedifferentiated liposarcoma, a more aggressive and potentially fatal malignancy. 5 The preferred treatment for liposarcomas is surgical excision with wide margins. 6
In this case study, we present the case of a 55-year-old male with a giant soft tissue mass located in the right supraclavicular fossa. This report explores the rarity of giant liposarcomas occurring in this specific anatomical location.
Case Report
A 55-year-old male sought evaluation for an 18 cm × 18 cm × 17 cm nontender, mobile soft tissue mass in the right supraclavicular fossa. The mass, which had been present for a decade, extended from the superficial aspect of the pectoralis major muscle to the submandibular region.
He had trauma to the area approximately 20 years earlier but denied prior surgery. On physical examination, the mass was soft, compressible, and mobile, with an area of firmness inferiorly (Figure 1). The patient only complained of poor sleep and discomfort in lying flat, along with pain in the mornings and with activities. The patient was predominantly asymptomatic and denied fever, chills, nausea, vomiting, facial or eyelid weakness, or anhidrosis.

Gross appearance of the lesion on the right supraclavicular fossa extending from the submandibular region to the superficial aspect of pectoralis major muscle.
Computed tomography (CT) scan (Figure 2A and B) and magnetic resonance imaging (MRI; Figure 2C) revealed an 18 cm predominant fat density signal with intralesional septations and mild enhancement. Mild tracheal deviation and mass effect of the right inferior thyroid lobe were seen. Ultrasound-guided fine needle aspiration and core needle biopsies revealed fragments of adipose tissue with large mature adipocytes and an interspersed population of atypical and pleomorphic fusiform cells with high nuclear-to-chromatin ratio, nuclear hyperchromasia, and occasional multinucleation suggestive of an atypical lipomatous tumor (Figure 3); however, the distinction could not be made between a pleomorphic lipoma and WDL.
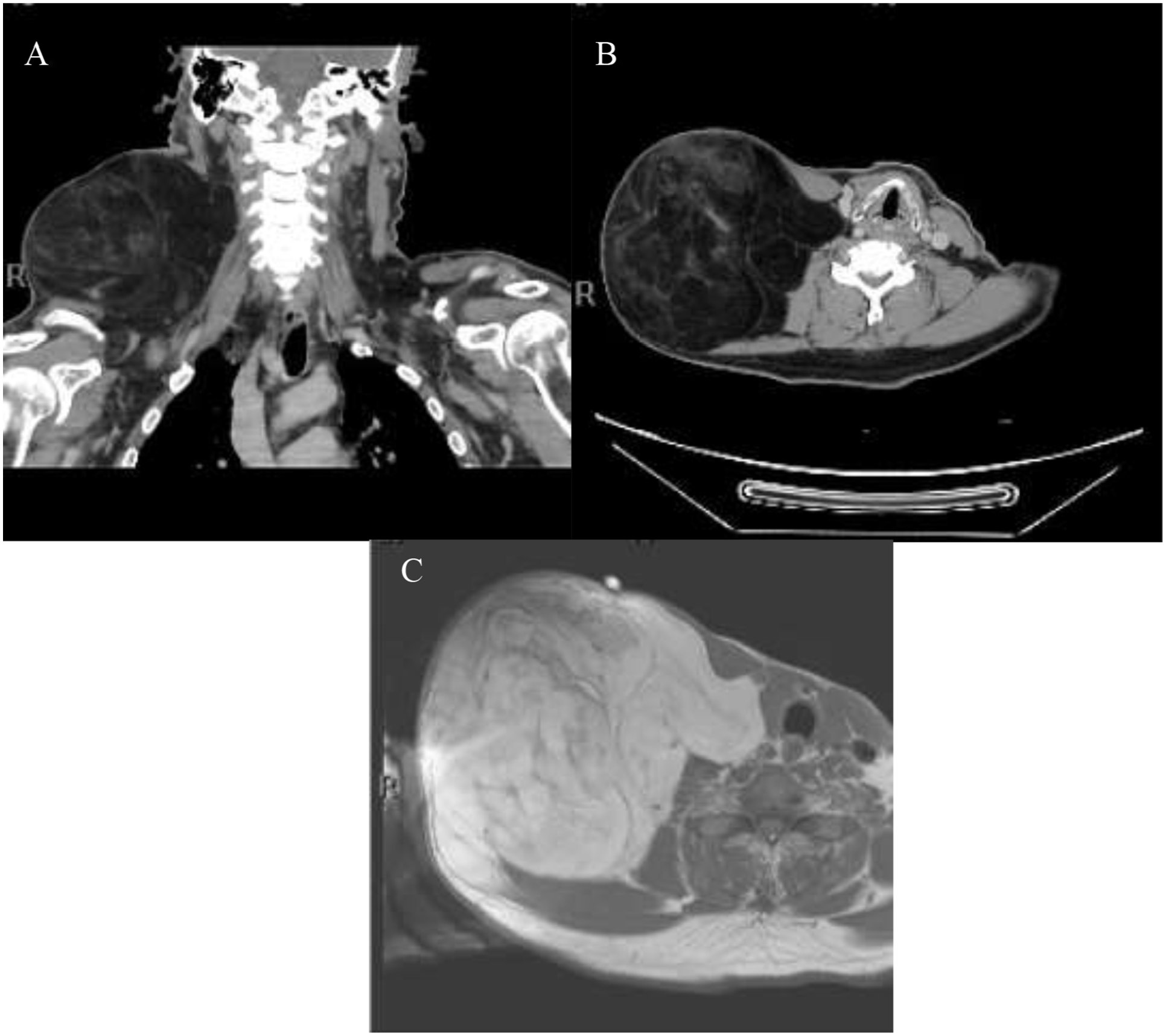
(A) Coronal and (B) axial neck CT scans showing giant heterogenous lesion extending from right supraclavicular region to just below parotid gland. (C) Axial neck MRI showing large predominantly fat signal intensity at the right supraclavicular area with septations and mild enhancements. CT, computed tomography; MRI, magnetic resonance imaging.
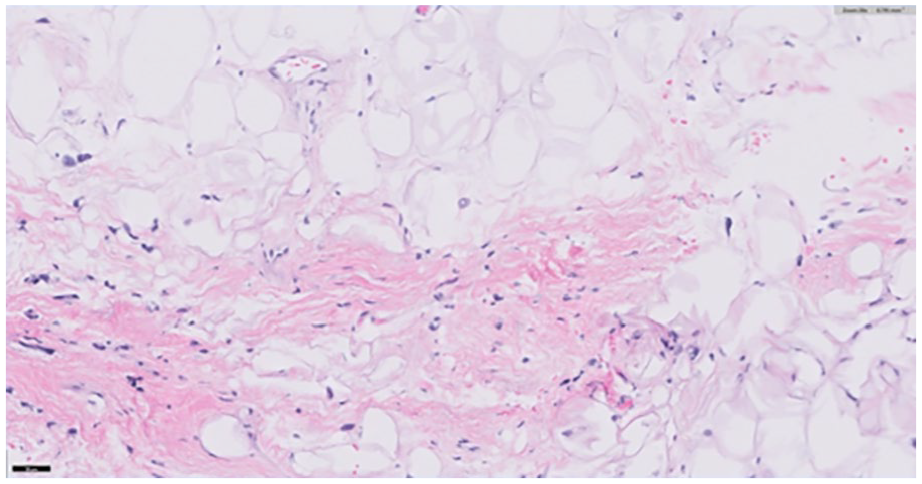
Fine needle aspiration of the lesion revealed lipomatous lesion with atypical cells in the fibrous septa.
Excision was achieved en bloc through neck and supraclavicular fossa dissection. A level II to IV neck dissection was performed to separate the mass from the carotid sheath. All critical structures were preserved, including the spinal accessory nerve contribution to the trapezius muscle. Lymph nodes from neck levels 2A, 3, 4, and 5 were excised.
Pathology
A final pathologic evaluation of this large lipomatous tumor revealed atypical cells in the background of adipose tissue and fibrous septa (Figure 4A and B), which support the diagnosis of atypical lipomatous tumor or well-differentiated liposarcoma. Tissue was sent for MDM2:CEP2 gene identification by fluorescence in situ hybridization. MDM2 is commonly identified in WDL/atypical lipomatous tumor. Although the sample did not meet the threshold for MDM2 amplification to be identified, there was significant nuclear pleomorphism with atypical nuclei demonstrating a higher MDM2:CEP2 ratio. Given the size of the tumor and the interspersed nuclei with higher MDM2:CEP2 ratios, a diagnosis of WDL was made. Excised lymph nodes were all negative for metastasis.
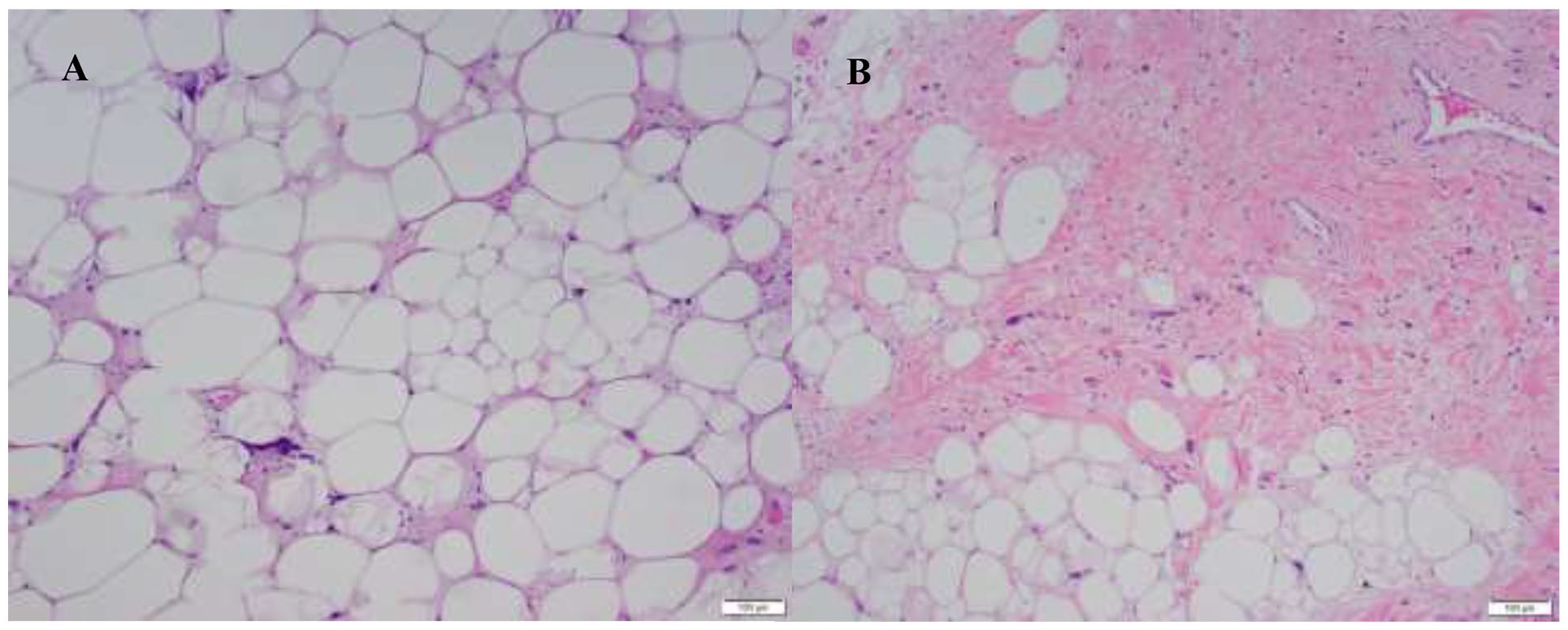
(A) Resection specimen revealed lobulated lipomatous tumor with adipocytes at different sizes with occasional atypical cells with the morphology of lipoblasts. (B) Atypical cells are much more numerous along the fibrous septa, a common feature of well-differentiated liposarcoma.
Discussion
The final diagnosis of this case was a giant WDL in the supraclavicular fossa region. WDL represents 40% of liposarcomas but rarely occurs in the head and neck region. Most WDL occurs in the retroperitoneum, subcutaneous tissue, deep soft tissue of the extremities, paratesticular area, and mediastinum. 7 WDL is the most common type of sarcoma in adults, and it has 2 main variants, the adipocytic and sclerosing.5,6 The adipocytic is the subtype found in our case and is characterized by its gross resemblance to mature adipose tissue. WDL tends to be locally aggressive, attributed mainly to its slow growth and the potential to disturb surrounding tissues.
While it may reoccur if excision is incomplete, it has a low tendency to metastasize, with 5 and 10 year survival rates of 100% and 82.1% posttreatment, respectively.5,8
To confirm the diagnosis of WDL, imaging alone is unreliable in differentiating the liposarcomas types. However, since WDL is primarily composed of fatty tissue, radiologically, it is expected to appear like fat. However, on CT, a liposarcoma will also have homogeneous attenuation with nodular soft tissue within the fatty mass; it may have a poor definition of the adjacent structures and thick septa (>2 mm). 9 In addition, on MRI, WDL has an almost entirely fat signal but will have thick septa (>2 mm), and some enhancement of local infiltration. 9
So, although imaging modalities may guide the diagnosis, histologic examination is necessary to make the diagnosis. Grossly, WDL may look like a benign lipoma; however, under the microscope, WDL significantly varies in the adipose cell size. There is also focal nuclear atypia, which may be hyperchromatic. 6 These atypical cells are more often seen perivascular or within the fibrous septa. In terms of the actual pathology, WDL cells have several immunologic markers. Neoplastic cells of WDL show positive reactions with S100 (mature adipocytic component), MDM2, and CDK4. In addition, MDM2 amplification is frequent and specific for WDL.5,10 In our case, the high expression of the MDM2 supported the diagnosis of WDL.
Regarding the preferred treatment, wide excision of all the tumors is recommended to avoid recurrence and possible dedifferentiation. 6 Radiation has been used on tumors inadequately removed from difficult anatomical locations such as the supraclavicular fossa. For example, the earliest 3 case studies of liposarcoma in the supraclavicular fossa are seen in the study by Kindblom et al, 11 in which the surgeries had incomplete resection of the mass, which resulted in reoccurrence and adjuvant radiotherapy treatment. Two of the cases had high morbidity, as 1 had their clavicle removed without complete resection, and the other had an interthoracoscapular amputation to achieve complete resection after failed radiation therapies, leaving both patients disabled with limited limb mobility. The last case of Kindblom et al 11 had incomplete removal due to its involvement to the pleura. We later see in the literature that complete removal of the tumor in the supraclavicular fossa gave favorable results and did not show recurrence.12-14 However, previous studies have reported smaller dimensions of liposarcomas. Specifically, they were 7 cm in 1 case, 12 12 cm in another, 13 and at most 5 cm in the last, 14 making our case unique in terms of tumor size.
Our patient had an 18 cm × 18 cm × 17 cm giant WDL liposarcoma in the supraclavicular fossa, and we have shown that even in the largest WDL liposarcoma seen in the literature thus far, complete and radical excision is still achievable. Two years after surgery, the patient did not show any signs of recurrences or distal metastasis.
Footnotes
Acknowledgements
We would like to thank the Otolaryngology Department and Pathology Department of University of Texas Medical Branch for their support. All authors contributed to the writing of the final manuscript.
Author Contributions
The following manuscript has been approved after being reviewed by the authors in a representation of honest work. The guidelines of the ENT journal have been reviewed and implemented in our manuscript. All authors aided in manuscript writing, and manuscript revisions.
Data Availability
The authors confirm that the data supporting the findings of this study are available within the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Informed consent for patient information to be published in this article was not obtained because identifying information, such as names and places, have been anonymized to ensure participant safety and privacy.