
Abstract
Introduction
Lymphadenopathy is the term used to describe the clinical signs of lymph node swelling. 1 Lymphadenopathy is benign and self-limiting in most patients. 2 Possible causes include infectious, immunologic, neoplastic, and metabolic diseases. 3 Depending on the patient's clinical presentation, lymphadenopathy location, and underlying risk factors, detection of this etiology may involve blood tests, imaging, and biopsy. 2
Serum C-reactive protein (CRP) is a positive acute-phase reactant synthesized by the liver. The level of CRP increases in the blood within hours in response to inflammation and infection. CRP is often used to monitor infection and inflammation. It can also be used for diagnosis, treatment follow-up, and mortality prediction, especially in inflammatory cases. 4
Albumin is a negative acute-phase reactant synthesized by the liver, and its level in the blood decreases during inflammation. Previous studies have shown that albumin is associated with inflammation severity, disease prognosis, and mortality. The CAR is a new prognostic marker based on inflammation that helps determine the severity of inflammation and mortality. 5
The CAR has been previously studied in many inflammatory diseases and cancer types, and this ratio has been found to be associated with disease. However, no study to date has investigated the effect of the CAR in patients with neck lymphadenopathy.
Materials and Methods
We retrospectively reviewed the information of 223 patients who applied to our clinic with neck lymphadenopathy complaints between 2013 and 2020. A detailed anamnesis was performed for patients with neck lymphadenopathy. The patient's age, the length of time the mass had been present, and other accompanying complaints (fever, weight loss, fatigue, hoarseness, difficulty swallowing, nasal congestion, nosebleeds, hemoptysis) were questioned. The medications that the patient used that could cause lymphadenopathy were questioned. Complete ear, nose, and throat examinations and head and neck examinations were then performed. The physical examination evaluated the location, size, number, mobility, adhesion, whether it was painful, and whether there was redness and increased temperature in the mass. The nasal cavity, nasopharynx, oropharynx, hypopharynx, and larynx structures were examined endoscopically. In order to detect possible infection and blood dyscrasia, CRP, white blood cells, red blood cells, and platelet values were examined. Epstein-Barr Virus (EBV), Cytomegalovirus (CMV), Toxoplasma, Francisella tularensis, and tuberculin skin tests were performed in patients with suspected infection and matching symptoms. All patients were evaluated routinely using neck ultrasonography.
As a result of all examinations and tests, patients whose cause of lymphadenopathy was determined were followed up and treated by us for pathologies requiring Ear-Nose-Throat expertise. Patients who were to be followed up and treated at other clinics were referred to other clinics (infectious diseases clinic, radiation oncology clinic, medical oncology clinic, internal medicine clinic). Empirical antibiotic treatment (amoxicillin-clavulanate 1000 mg 2 × 1) was administered ten days to patients whose source could not be identified during examinations. The antibiotherapy response was evaluated clinically and ultrasonographically. In the third week, fine needle aspiration biopsy (FNAB) was performed on lymph nodes that did not decrease in size clinically and ultrasonographically. Patients who responded to antibiotic treatment were followed up. Of these patients, those with lymphadenopathy whose cause was determined (tumor or infection) and those whose cause could not be determined but responded to empirical antibiotic treatment were excluded from the study. Excisional biopsy was planned for patients whose lymphadenopathy could not be determined, those who did not respond to antibiotic treatment, those who were pathological according to ultrasound findings, those who had nondiagnostic FNAB results, and those who were suspected of lymphoma. Patients with lymphadenopathy with a short axis >1 cm, unresponsive to antibiotic treatment, nondiagnostic FNAB results, or suspected lymphoma were included in the study.
Patients diagnosed with FNAB, those who responded to antibiotic treatment, those with cardiovascular risk factors, those with malnutrition or weight loss, and those previously diagnosed with cancer or lymphoproliferative disease were excluded from the study.
In viral or bacterial infections, the CRP/CAR ratio may vary depending on the time the blood test is performed. In particular, in the early stages of infection, a higher CRP/CAR is expected. Therefore, in our study, viral infections were excluded in all cases and CRP values after antibiotic treatment were used.
The diagnostic algorithm of patients with neck lymphadenopathy is shown in Figure 1.
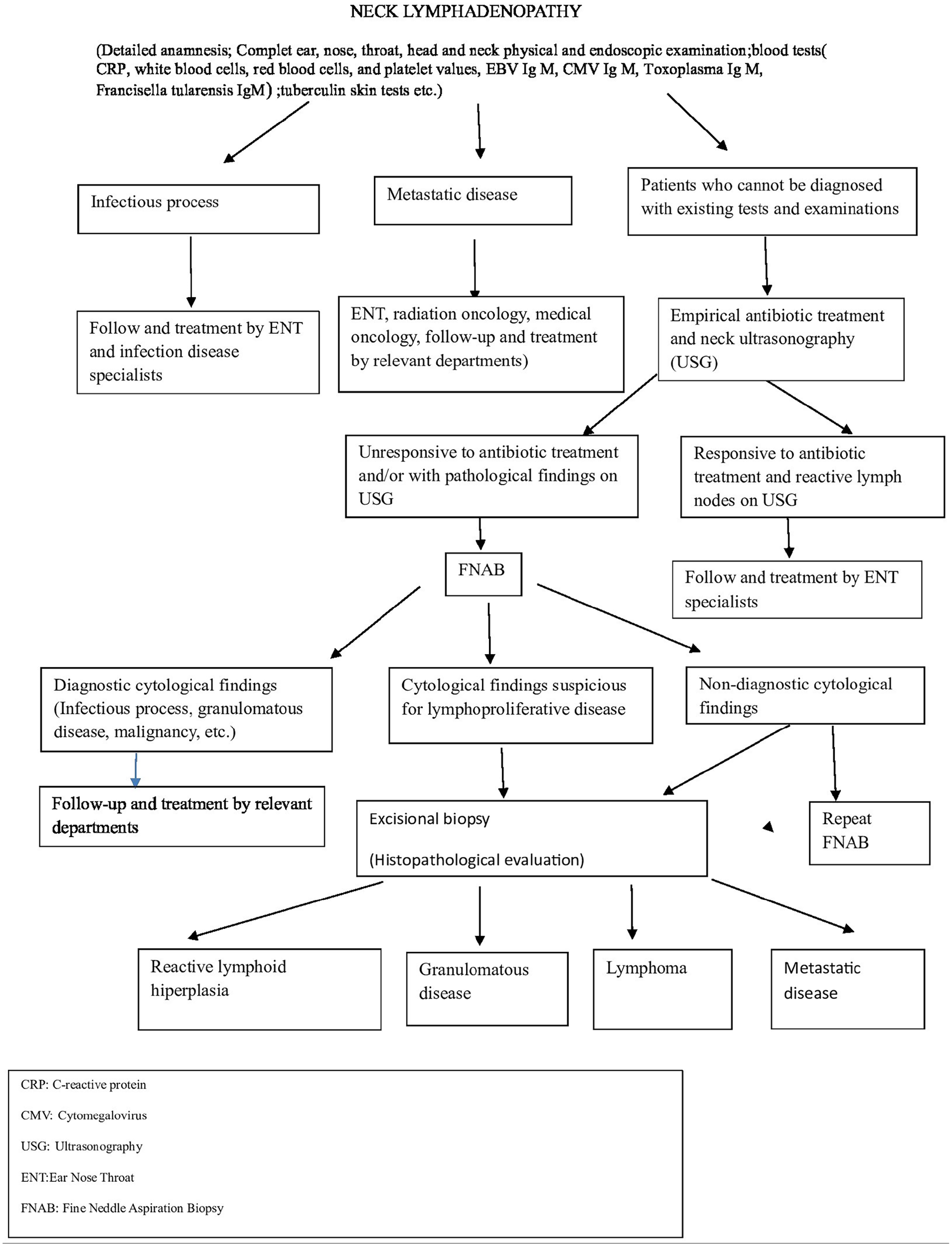
Diagnostic algorithm of patients with neck lymphadenopathy.
Analysis of Results
The pathological results were divided into 4 groups: (1) patients with reactive lymphoid hyperplasia; (2) patients with granulomatous disease; (3) patients with lymphoma; and (4) patients with metastatic disease.
All groups were compared in terms of age, gender, CRP level, albumin level, and CRP/albumin ratio.
Statistical Analysis
Statistical analyses were performed using the SPSS for Windows software (ver. 19.0; SPSS Inc, Chicago, IL, USA). The distribution of data was determined using the Shapiro-Wilk test. The chi-squared test was used to determine differences in categorical variables between groups. Continuous variables were expressed as mean ± standard deviation and categorical variables as frequencies and percentages. Continuous variables were compared between the 2 groups using the independent samples t-test or the Mann-Whitney U test. The Kruskal-Wallis test was used to determine differences among 3 or more groups. Repeated measures were compared using the paired-sample t-test or the Wilcoxon signed-rank test. Spearman’s analysis was performed to determine the relationships among continuous variables. A P-value of less than .05 indicated statistical significance in all tests (95 % confidence interval).
Results
In total, 74 patients (40 females and 34 males) were included in this study. Patients were aged 3–87 years (mean 47.82 ± 21.513 years). Forty (54,1%) patients were women, and 34 (45.9 %) were men. Pathologically, 24 (32.4%) patients were diagnosed with lymphoid hyperplasia, 17 (23%) with granulomatous disease, 20 (27%) with lymphoma, and 13 (17.6%) with metastatic disease. The age, sex, CRP albumin, and CAR values of the patients are presented in Table 1.
Age, Gender, CRP, Albumin, CRP/Albumin Ratio Values of the Patients.
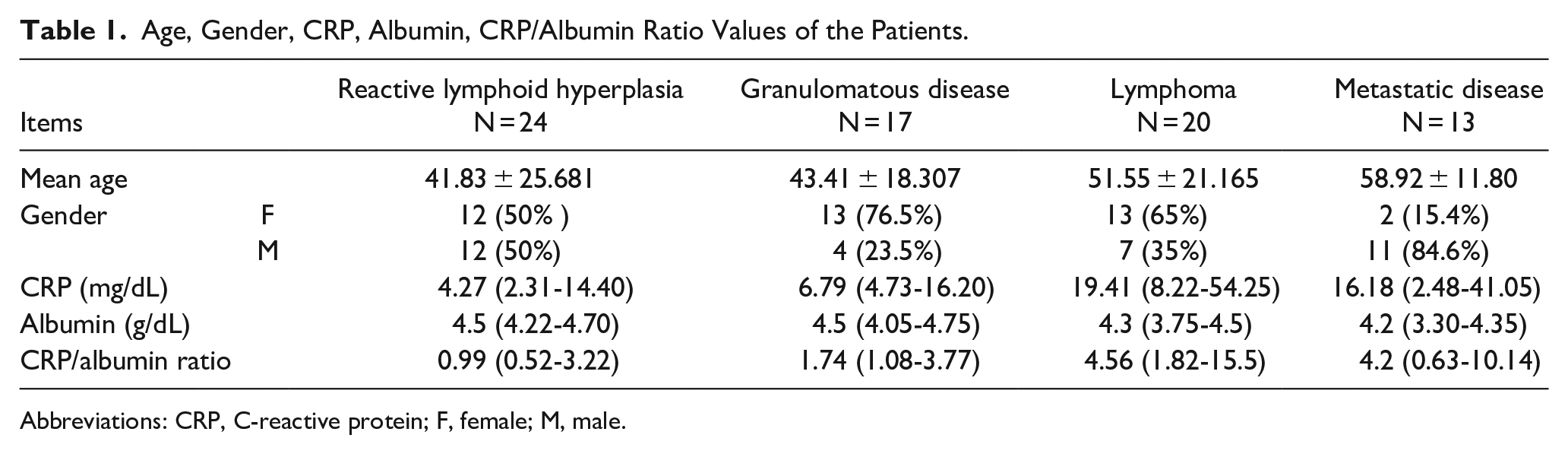
Abbreviations: CRP, C-reactive protein; F, female; M, male.
Age
When all groups were compared with each other in terms of age, no significant difference was found between the groups in terms of age.
Gender
All groups were compared in terms of sex, and it was observed that the male sex was significantly higher in the group diagnosed with metastatic disease than in the other groups (P = .005).
CRP
CRP values of the groups were compared, and CRP values were found to be significantly higher in the lymphoma group than in the lymphoid hyperplasia group (P = .007).
Albumin
When albumin values were compared between the groups, significantly-lower albumin values were found in the metastatic disease group than in the lymphoid hyperplasia group (P = .032).
CRP/Abumin Ratio
When the patients’ CRP/albumin ratios (CAR) were compared, a significant difference was found between reactive lymphoid hyperplasia and lymphomas. The CAR was significantly higher in lymphomas than in lymphoid hyperplasia (P = .006). P values are shown for CRP, albumin, and CRP/albumin ratios in Table 2. CAR values are shown graphically in Figure 2.
P values of CRP, Albumin, CRP/Albumin Ratios Between Groups.
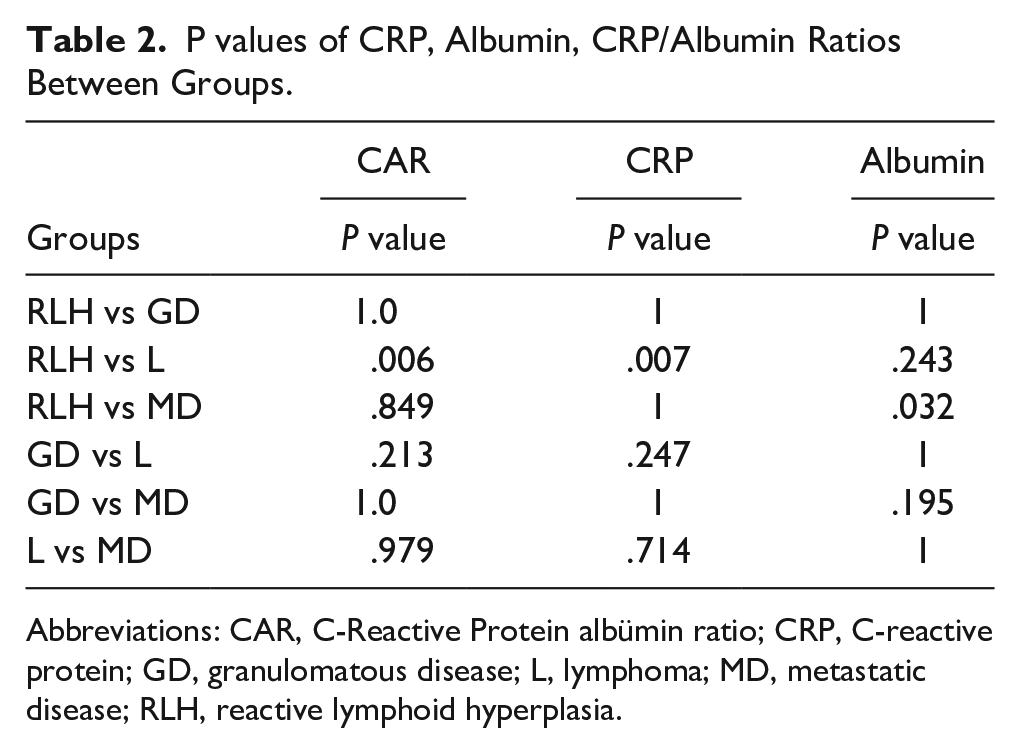
Abbreviations: CAR, C-Reactive Protein albümin ratio; CRP, C-reactive protein; GD, granulomatous disease; L, lymphoma; MD, metastatic disease; RLH, reactive lymphoid hyperplasia.
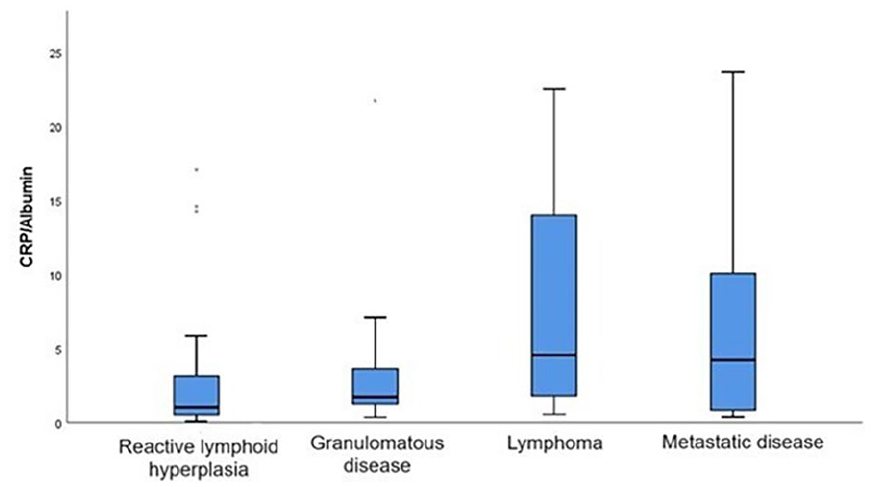
Graphical representation of CRP/albumin ratios between groups. CRP, C-reactive protein.
Discussion
CRP, an acute-phase reactant, is a marker of inflammation synthesized in the liver and induced by proinflammatory cytokines, particularly IL-6. 6 Hence, it is good to mention this for a better statistical analysis. CRP plays a role in bacterial infections and the regulation of autoimmunity and atherogenesis. It is unclear whether its role is pro-inflammatory or anti-inflammatory. 7 CRP levels are elevated in infectious and inflammatory diseases, atherosclerosis, autoimmune diseases, diabetes, traumas, cancers, and depression. In our study, serum CRP levels were found to be elevated in all groups. Various studies have shown that CRP plays a role in both lymphomas and cancer pathogenesis.8-11 In addition, CRP has been reported to play an essential role in the adaptive immune response, apo, and even in the regulation of autoimmunity. 12 In our study, there were no significant differences in CRP elevation between the other groups. However, when lymphomas and reactive lymphoid hyperplasias were compared, CRP levels were significantly higher in lymphomas. Beguelin and Takahashi showed elevated CRP in lymphomas.10,11
Malnutrition is a common complication observed in 80% of patients with advanced cancer. 13 The changes in this feeding mechanism are not fully understood. Catabolic factors produced by cancer cells, the inflammatory response of the host, and increased energy demand may result in malnutrition. 14 Serum albumin is a well-known nutritional marker; however, its physiological role is also related to its anti-inflammatory function. 15 Low albumin levels increase the release of inflammatory cytokines (such as interleukin-6 and tumor necrosis factor-alpha) from cancer cells. 16 IL-6 is also a major cytokine in CRP increase. Therefore, the CAR is also increased in patients with cancer due to increased CRP levels and low albumin. In our study, the CAR was increased and albumin levels were decreased in the carcinoma group. When the reactive lymphoid hyperplasia group was compared with the metastatic disease group, the albumin level was significantly lower in the carcinoma group. This finding is consistent with the literature. Although low albumin levels in lymphomas have been reported in various studies, no significant low albumin levels were found in our study. 17 Low albumin levels were used for survey determination rather than diagnosis.18-20
In recent years, systemic inflammatory responses and the immune system have been shown to play essential roles in the tumor microenvironment. 21 Many parameters indicate systemic inflammation. The systemic immune-inflammation index, including the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, monocyte-to-lymphocyte ratio, and C-reactive protein-to-albumin ratio (CAR), is related to the survival of patients with tumors.
The CAR is a critical marker indicating the host’s nutritional index and systemic inflammation status. In recent years, it has been considered an independent parameter for the prognosis of small-cell lung cancer, esophageal squamous cell carcinoma, hepatocellular carcinoma, renal cell carcinoma, colorectal cancer, pancreatic cancer, nasopharyngeal carcinoma, and head and neck carcinoma.22-27 It is unclear whether a high CAR is a facilitator of carcinogenesis, a result of immunosuppression, or whether carcinomas increase this ratio. In a meta-analysis of 7080 patients by Luan et al., the CAR was identified as a significant prognostic marker for various head and neck cancers. In our study, the CAR was high in lymphomas and carcinoma metastases. The severity of systemic inflammation in lymphomas, inflammatory markers released from tumor cells, and nutritional problems of patients explain the increase in this ratio. When the ratios of patients with lymphomas and benign lymphoid hyperplasia were compared, the CAR in patients with lymphomas was significantly higher. This situation showed that systemic inflammation is quite high in lymphomas. Difficulty distinguishing between reactive lymphoid hyperplasia and lymphoma in neck lymphadenopathies. Many patients with doubt undergo excisional biopsy. In our study, after giving the lymphoid tissue result of FNAB, by observing the CAR, we can save time in terms of follow-up by avoiding excisional biopsy in cases in which this ratio is low or by protecting the patient from an invasive procedure. If the CAR is high, time can be saved by performing a quick excisional biopsy. More definitive results can be obtained by increasing the number of patients.
In our study, male sex was significantly more frequent in carcinoma metastases. Studies have shown that there is a male predominance in both head and neck cancers and lung and GIS tumors, whereas there is no gender distinction in lymphomas. 28 Head and neck SCC affects more males than females. Many studies have reported similar numbers of males.28-30 In granulomatous diseases, female predominance is known. 31 In our study, although the number of female patients was higher in the granulomatous inflammation group, no significant difference was found according to sex.
This exploratory study has several limitations. First, it included a small sample size and was retrospective. Larger prospective studies are needed to draw generally-applicable conclusions.
Conclusion
Neck lymphadenopathies are clinical conditions that can cause diagnostic difficulties. Sometimes, they are difficult to diagnose despite the results of all tests performed. In particular, when the FNAB results are reported as lymphoid cells, we perform an excisional biopsy to differentiate between reactive lymphoid hyperplasia and lymphoma. According to this study, we think that we can make a prediction by looking at the CRP/albumin ratio before excisional biopsy and that it can be a helpful factor that can move the patient to the excisional biopsy stage more quickly without reducing clinical time.
Footnotes
Clinical Trial Number
None.
Data availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Zonguldak Bülent Ecevit University Ethics Review Committee at Zonguldak Bülent Ecevit University approved our interviews (approval: 2020/25) on December 30, 2020. Respondents gave written consent for review and signature before starting interviews.
Informed Consent
Informed consent was obtained from all participants included in the study.