
Abstract
Background. In the early stages of severe burn cases, an increase in serum C-reactive protein (CRP) level and a decrease in serum albumin level can be observed. Objective. This study aimed to investigate whether the CRP/albumin ratio at the time of hospital admission in children exposed to severe burns would be an indicator for bacterial growth at the wound site. Method. A total of 137 pediatric patients who were treated in our hospital’s burn center due to third-degree burns of 30% or more of their body between January 2019 and October 2023 were included in the study. Results. The mean age was 3.69 ± 4.16 years. CRP/albumin ratio was found to be an independent risk factor for culture positivity (odds ratio: 1.162; P = .01). Conclusion. High CRP/albumin ratio in children with severe burns may provide important information about the development of wound colonization or infection, most likely due to prolonged hospital stay.
Introduction
In pediatric patients exposed to severe burns, skin integrity is disrupted over a wide area and to a great extent. Accordingly, the patient’s recovery time is prolonged, the risk of developing complications increases, the prognosis is worse, and the possibility of microorganism growth at the wound site increases.1-3
C-reactive protein (CRP) is a type of protein produced by the liver and indicates inflammation in the body. Normally, the CRP level in the blood is very low. However, when an infection, injury, burn, or other inflammatory condition occurs in the body, the CRP level increases rapidly. CRP measurements are used in many clinical situations, such as monitoring infections, monitoring chronic inflammatory conditions such as rheumatoid arthritis, lupus, or vascular diseases, as well as assessing the risk of infection after surgery.4-7
Edema may develop as a result of skin damage, increased vascular permeability and inflammation in burn patients. This condition can lead to leakage of body fluids into the tissues due to loss of the skin barrier and leaky vessels. Particularly large burns or severe burns can cause uncontrolled accumulation of body fluids in the tissue and lead to edema. Albumin is an important plasma protein produced by the liver and is the most common protein in the blood. Albumin helps maintain fluid balance in the body. The risk of edema may increase with a decrease in albumin level in burn patients.8-10
It has been shown that in cases of severe inflammation, there may be significant changes in the CRP/albumin ratio due to an increase in the CRP level and a decrease in the albumin level, and this ratio is informative in terms of prognosis in many diseases.11,12 To the best of our knowledge, a relationship between CRP-albumin level and burn wound infection has not yet been demonstrated in children with severe burns. This study aimed to investigate whether the CRP/albumin ratio at the time of hospital admission in children exposed to severe burns would be an indicator for bacterial growth at the wound site.
Methods
Patients and Tests
The study included 137 pediatric patients who were treated in our hospital’s burn center or burn intensive care unit due to third-degree or higher burns on 30% or more of their body between January 2019 and October 2023.
Patients aged 18 and over and patients who died during burn treatment were not included in the study. Patients who were hospitalized and discharged for the day were not included in the study. Inhalation burns and genital area burns were not included the study. Additionally, patients with autoimmune diseases, immunodeficiency, oncological and active rheumatological diseases were excluded from the study. Biochemistry and culture results of the patients’ first admission to the hospital were obtained by scanning backwards from the hospital records.
For the CRP/albumin ratio, the threshold value of 3.365 determined in the ROC analysis conducted in the study was used.
Statistical Analysis
The sample size in the study was calculated by power analysis using G-Power (version 3.1.9.6, Franz Faul, Universitat Kiel, Germany). Effect size 0.6; Type 1 error was taken as 0.05 and test power as 0.95, and the minimum required sample size was determined as 54.
All statistical analyzes in the study were performed using SPSS 25.0 software (IBM SPSS, Chicago, IL, USA). Descriptive data were given as numbers and percentages. Comparisons between groups in terms of categorical variables were made with Pearson’s Chi Square test and Fisher’s Exact Test. Whether continuous variables were normally distributed or not was analyzed with the Kolmogorov-Smirnov Test. Differences between groups in terms of non-normally distributed continuous variables were analyzed with the Mann Whitney U test. The relationship between continuous variables was evaluated with Spearman correlation analysis. The risk coefficients of the variables in terms of reproduction in wound culture were determined by logistic regression analysis. The predictive capacity of the CRP/albumin ratio for culture positivity was analyzed by ROC analysis. The results were evaluated within the 95% confidence interval and P-values <.05 were considered significant. Bonferroni correction was made where necessary.
Ethical Approval and Informed Consent
This retrospective cohort study was approved by the local ethics committee number SÜKAEK 2023 20/8 date 26.10.2023. Informed consent was not needed.
Results
A total of 81 (59.1%) of the patients were male. No significant difference was found between genders in terms of culture positivity (P = .198) and the distribution of bacterial species growing in culture (P > .101) (Table 1). The distribution of isolates with positive growth is shown in Table 1.
Distribution of Culture Results According to Gender.

The comparison between culture-negative and culture-positive groups.
The comparison among the culture results regarding the microorganism growth. Chi square test was used.
The mean age of the patients was 3.69 ± 4.16 years, and the mean hospital stay was 19.99 ± 20.02 days. In the culture-positive group, mean hospital stay (48.91 ± 40.12 vs 17.45 ± 15.02; P = .001), CRP level (86.67 ± 42.94 vs 54.07 ± 48.24; P = .011) and CRP/albumin ratio (17.95 ± 19.03 vs 4.78 ± 5.47; P = .026) were found to be significantly higher than the culture-negative group (Table 2).
Comparison Between Culture-negative and Culture-positive Groups in Terms of the Mean Values of Some Variables.

Mann-Whitney U test was used.
Abbreviations: SD, standard deviation; CRP, C-reactive protein.
In the ROC analysis, the sensitivity and specificity of the value of 3.365 for the CRP/albumin ratio for its capacity to predict culture positivity were determined to be 75.0% and 55.2%, respectively (Area under curve = 0.695; P = .026; lower bound = 0.528; upper bound = 0.861 ) (Figure 1).
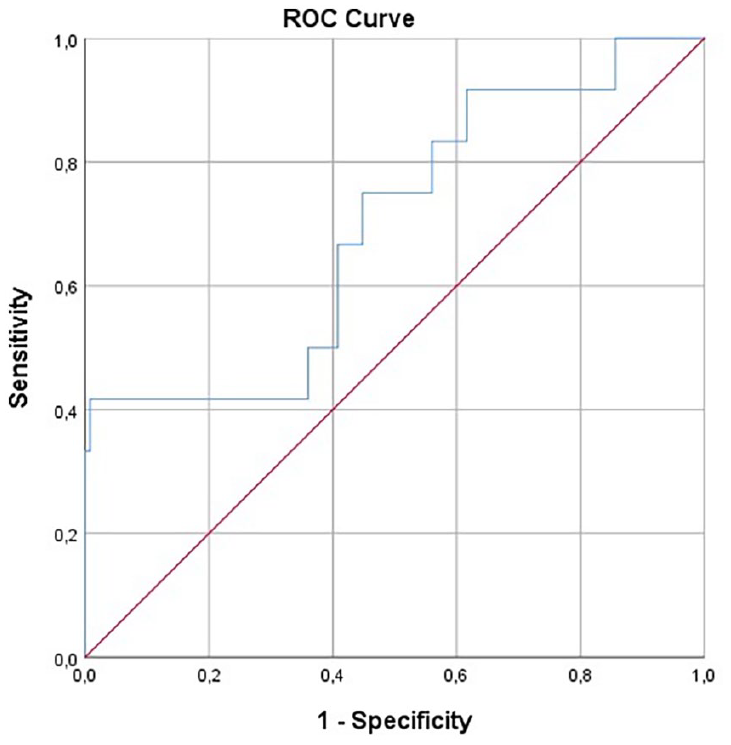
In the ROC analysis, the sensitivity and specificity of the value of 3.365 for the CRP-albumin ratio for the predictive capacity of culture positivity were determined to be 75.0% and 55.2%, respectively (Area under curve = 0.695; P = .026; lower bound = 0.528; upper bound = 0.861).
The rate of those with CRP/albumin values above the threshold value of 3.365 determined by ROC analysis in this study in the culture-positive group was found to be significantly higher than the culture-negative group (75.0% vs 44.8%; P = .045) (Table 3).
Distribution of CRP/albumin Ratio Values According to the Groups.

Chi square test was used. The threshold value of 3.365 for CRP-albumin ratio was determined by ROC analysis. CRP: C-reactive protein.
The culture positivity rate was significantly lower in those hospitalized for 1 to 10 days than in those hospitalized longer (P = .047), and significantly higher in those hospitalized for more than 40 days (P < .001) (Table 4).
Distribution of Hospital Stay Groups According to the Culture Result Groups.

Chi square test was used.
Logistic regression analyzes revealed that hospital stay (P = .027) and CRP/albumin ratio (P = .01) were independent risk factors for culture positivity. Accordingly, prolonged hospitalization increased the risk of culture positivity by 1.047 (1.005-1.090) times. An increase in CRP albumin level could predict culture positivity 1.162 (1.037-1.303) times better (Table 5).
Logistic Regression Analyzes About Some Variables to Predict Culture Positivity.

Logistic regression analysis was used.
Abbreviations: CRP, C-reactive protein.
In the correlation analysis, CRP level (P < .001; r = .515) and CRP/albumin ratio (P < .001; r = .516) were found to be moderately positively and significantly correlated with the duration of hospitalization.
Discussion
Severe and large-area burns occurring in children are life-threatening clinical conditions. Significant impairment of skin integrity in these patients significantly increases the risk of colonization or infection at the wound site.1,2,13 In our study, it has been shown that the CRP/albumin ratio can be used as a predictor in terms of bacterial growth in the burn areas of these patients.
It has been stated that the bacteria that most commonly cause hospital-acquired colonization or infection are Acinetobacter and Pseudomonas.14,15 In our study, the bacterial species most frequently detected in wound cultures were Acinetobacter baumannii and Pseudomonas aeruginosa. These findings show that there is a high probability of developing hospital-acquired colonization or infection in burn patients who have to stay in the hospital for a long time. No significant difference was found between culture-positive and culture-negative groups in terms of mean age, total protein, albumin, CRP and CRP/albumin ratio values. These findings indicate that these values do not provide important information in predicting burn wound culture results.
In our study, no significant difference was found between genders in terms of culture positivity and distribution of bacterial species growing in culture. This shows that gender has no effect on culture positivity in children with severe burns.
It has been stated that the risk of developing hospital-acquired colonization or infection in burn wounds increases significantly as the duration of hospitalization increases.16,17 In our study, the mean hospital stay in the culture-positive group was found to be significantly higher than the culture-negative group (48.91 vs 17.45). In addition, the culture positivity rate was found to be significantly lower in patients hospitalized for 1 to 10 days than in those hospitalized for a longer period of time, and significantly higher in those hospitalized for more than 40 days. In the logistic regression analysis, length of hospital stay was determined to be an independent risk factor for culture positivity. Accordingly, it was observed that prolonged hospitalization increased the risk of culture positivity by 1.047 (1.005-1.090) times. All these findings show that as the length of hospital stay increases, the risk of colonization or infection at the burn wound site—most likely hospital-acquired—increases significantly.
Albumin, a major plasma protein, has an important role in regulating plasma colloid osmotic pressure. In cases of trauma to the skin, edema develops due to the decrease in albumin level. It has been reported that there are significant changes in albumin level in severe burn cases.18-20 However, it has been reported that low albumin level is informative in terms of poor clinical course in some diseases.21,22 In our study, the mean albumin level was found to be statistically similar between the culture-negative and positive groups (20.82 vs 16.16). This may be due to the low number of patients in the culture-positive group.
CRP begins to increase within the first 24 hours of the inflammatory process in cases where inflammation occurs due to conditions such as disease or trauma. High CRP levels are seen depending on the severity of the inflammation condition. The patient’s clinical course and response to treatment significantly affect CRP levels.5,23 It has been reported that high CRP levels in burn patients are a risk factor for the development of sepsis and have an impact on mortality. 24 In our study, the mean CRP level in the culture-positive group was found to be significantly higher than the culture-negative group (86.67 vs 54.07). This finding shows that the CRP level at hospital admission in children with severe burns may be informative in terms of bacterial growth at the wound site, possibly due to the prolongation of hospital stay.
It has been stated that high CRP/albumin ratios due to rising CRP and falling albumin levels in some serious disease and trauma cases can provide important information in terms of clinical course, prognosis and response to treatment. It has been reported that high CRP/albumin ratios can indicate poor prognosis in many diseases such as some infections, sepsis and cancer.25-31 Nosocomial infections, which are considered a significant challenge in the management of burn patients, seriously affect prognosis. In these patients, more than 40% of the total burned body surface area, full-thickness burns, and long hospital stays are reported to be serious risk factors for survival. 32 In our study, the mean CRP/albumin ratio in the culture-positive group was found to be significantly higher than the culture-negative group (17.95 vs 4.78). In the logistic regression analysis, CRP/albumin ratio was determined to be an independent risk factor for culture positivity. It was determined that an increase in CRP albumin level could predict culture positivity 1.162 (1.037-1.303) times better. In the ROC analysis, the sensitivity and specificity of the value of 3.365 for the CRP/albumin ratio for the predictive capacity of culture positivity were determined to be 75.0% and 55.2%, respectively. The rate of those whose CRP/albumin ratio was above the threshold value determined in this analysis was found to be significantly higher in the culture-positive group than in the culture-negative group (75.0% vs 44.8%). All these findings indicate that in children with severe burns, patients with high CRP/albumin ratios at the time of admission to the hospital are significantly more likely to develop colonization or infection at burn sites due to their longer hospital stay. It shows that it can provide important information about the development of infection.
There were some limitations in our study. The fact that the number of patients and the number of patients with positive culture results in samples taken from the burn wound site in the study was not high may have had a negative impact on the level of statistical significance in some analyses. Since the study also aimed to investigate the ability of CRP/albumin ratio to predict the development of colonization or infection in the wound site, only laboratory values at admission to the hospital were examined, changes in these values during the patient’s hospitalization were not included in the study, and their effects on the clinical course of the disease or treatment were not analyzed. Not to evaluate localization of the burned areas and the cause of the burns in patients can be considered as limitation.
Conclusions
In our study, as far as we could find, for the first time in the literature, although the number of monitored subjects were relatively low, the relationship between wound infection and CRP/albumin ratio in children with severe burns has been demonstrated. The findings obtained from our study show that the high CRP/albumin ratio due to high serum CRP levels and low albumin levels during hospital admission in children with severe burns may provide important information about the development of colonization or infection at the wound site, as it is most likely due to the prolongation of hospital stay. Accordingly, these patients with high CRP/albumin ratio during hospital admission should be monitored more closely for infection.
Footnotes
Acknowledgements
No.
Authors’ Note
Alper Ceylan is also affiliated with Samsun Training and Research Hospital, Department of General Surgery, Samsun, Turkey and Selim Görgün is also affiliated with Health Sciences University, Samsun Training and Research Hospital, Department of Microbiology and Clinical Microbiology Samsun, Turkey.
Author Contribution Statements
Literatural screening: SSB, SG, providing the data: SSB, AC, statistical analysis: SSB, SG, writing the manuscript: SSB, SG, reviewing the manuscript: SSB, AC, SG.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This retrospective cohort study was approved by the local ethics committee (Samsun University Faculty of Medicine) number SÜKAEK 2023 20/8 date 26.10.2023. Informed consent was not needed.