
Abstract
Objective
This study was performed to examine the relationship between the C-reactive protein/albumin ratio (CAR) and the prognosis of patients with lung adenocarcinoma and thus provide a reference for evaluating the prognosis of lung adenocarcinoma.
Methods
The clinical data of 130 patients with lung adenocarcinoma were retrospectively collected and analyzed. The patients’ overall survival (OS) time was calculated, and the factors affecting OS were statistically analyzed.
Results
The CAR was correlated with sex, clinical stage, brain metastasis, S100 calcium-binding protein B (S100B), interleukin 17, myelin basic protein, squamous cell carcinoma antigen (SCC-Ag), and the lymphocyte count. The median OS was significantly shorter in the high- than low-CAR group (18 vs. 64 months, respectively). The CAR, clinical stage, brain metastasis, S100B, interleukin 17, SCC-Ag, C-reactive protein, albumin, and neutrophil count affected the OS of patients with lung adenocarcinoma. The CAR and clinical stage were independent risk factors for a poor prognosis in patients with lung adenocarcinoma.
Conclusions
The CAR and clinical stage are independent risk factors for OS in patients with lung adenocarcinoma.
Keywords
Introduction
According to the latest global cancer statistics in 2020, 1 4.568 million patients with newly diagnosed cancer were reported in China; among these patients, 815,000 (17.9%) had lung cancer. In total, 3.002 million of all these patients with newly diagnosed cancer died; among them, 715,000 (23.8%) died of lung cancer. The incidence and mortality of lung cancer still rank first in China 1 and are showing an upward trend. 2 Non-small cell lung cancer (NSCLC) is the most common pathologic type of lung cancer, accounting for 80% to 85% of primary lung cancers, and adenocarcinoma of the lung is the most common type of NSCLC. 3 In recent years, the diagnostic rate of lung cancer has been increasing on an annual basis because of the continuous improvement and promotion of clinical diagnosis and treatment methods and technologies. However, despite the developments in surgery, radiotherapy and chemotherapy, targeting, immunization, and other methods of active treatment intervention, the overall prognosis of patients with lung cancer is still not ideal; the 5-year survival rate is <15%. 4 Therefore, accurate evaluation of the prognosis of patients with lung cancer is of great significance for standardized clinical treatment. Lung cancer is usually accompanied by an inflammatory response and poor nutritional status, which is generally characterized by an elevated C-reactive protein (CRP) concentration and decreased albumin (ALB) concentration. The CRP/ALB ratio (CAR) is an indicator of the balance between systemic inflammation and the nutritional status. Therefore, this study was performed to analyze the relationship between the clinical characteristics and prognosis of 130 patients with lung adenocarcinoma and thus identify prognostic indicators in these patients.
Materials and methods
Patients
In this retrospective study, the clinical data of 130 patients with lung adenocarcinoma who were admitted to Taicang Affiliated Hospital of Soochow University from December 2018 to November 2020 (including 30 patients with and 100 without brain metastasis) were collected and analyzed. All cases of lung adenocarcinoma included in this study were confirmed by histopathology or cytology. No patients had brain injury, cerebral hemorrhage, cerebral infarction, myocardial infarction, heart failure, autoimmune disease, a concomitant second tumor, or concomitant infection at the time of either disease diagnosis or inclusion in the experimental study. All patient details have been de-identified.
Data collection
The clinical data of all 130 patients were collected from the medical record system and outpatient system of Taicang Affiliated Hospital of Soochow University. These data included the serum CRP and ALB concentrations, sex, age, TNM stage (8th edition of the UICC TNM Classification), routine blood indices (white blood cell count (WBC), neutrophil count (NE), lymphocyte count (LY), mononuclear cell count (MO), and platelet count (PLT)), and serum concentrations of S100 calcium-binding protein B (S100B), interleukin 17 (IL-17), myelin basic protein (MBP), and squamous cell carcinoma antigen (SCC-Ag).
Starting from the time of diagnosis, the study endpoint was death due to primary disease or follow-up to 30 November 2020. The overall survival (OS) time was defined as the duration of time from the beginning to the endpoint of the study and was expressed in months. The reporting of this study conforms to the STROBE guidelines. 5
Sample collection
Fasting peripheral blood (5 mL) was collected from all patients in biochemical tubes. The specimens were allowed to rest at room temperature for about 2 hours and then separated at 1065.6 × g for 10 minutes. The upper serum layer was stored in anticoagulant tubes for subsequent measurement of the study indicators and stored at −80°C in a cryogenic refrigerator.
Statistical analysis
The clinical data of all 130 patients with lung adenocarcinoma were recorded in Excel data files (Microsoft Corp., Redmond, WA, USA) and statistically analyzed using IBM SPSS Statistics for Windows, Version 23.0 (IBM Corp., Armonk, NY, USA) and X-tile 3.5.0 software (Yale School of Medicine, New Haven, CT, USA). The results of the data analysis are expressed as mean ± standard deviation. The chi-square test was performed to assess the association between the CAR and clinical features. The Kaplan–Meier method was used to plot the survival curves of all 130 patients with lung adenocarcinoma, and the differences between the survival curves were analyzed using the log-rank method. A Cox proportional risk regression model was used to analyze the age, sex, CAR, and other clinical characteristics of patients with lung adenocarcinoma to determine the factors affecting OS. A P value of <0.05 was considered statistically significant.
Ethics approval and consent to participate
This study was conducted with approval from the Ethics Committee of Taicang Affiliated Hospital of Soochow University (No. 2021-KY-156) and in accordance with the Declaration of Helsinki. All patients provided written informed consent.
Results
Cutoff values of CAR and clinical indicators
The CRP and ALB concentrations were collected from all 130 patients at the time of initial diagnosis, and the CAR was calculated. The WBC, NE, LY, MO, PLT, S100B, IL-17, MBP, SCC-Ag, and other indicators were recorded, and X-tile software was used to calculate the cutoff value of each indicator (Table 1).
Cutoff values of each indicator.

CAR, C-reactive protein/albumin ratio; CRP, C-reactive protein; ALB, albumin; S100B, S100 calcium-binding protein B; IL-17, interleukin 17; MBP, myelin basic protein; SCC-Ag, squamous cell carcinoma antigen; WBC, white blood cell count; NE, neutrophil count; LY, lymphocyte count; MO, mononuclear cell count; PLT, platelet count.
Correlation between CAR and clinical characteristics
The 130 patients were divided into two groups according to the CAR cutoff value: the high-CAR group (CAR of >1.1) and low-CAR group (CAR of ≤1.1). They were also divided into two groups according to their median age of 65 years (>65 and ≤65 years). Moreover, the patients were divided into a stage I/II group and stage III/IV group according to the 8th edition of the AJCC TNM Staging Manual. Anemia was defined as a hemoglobin (Hb) concentration of <120.0 g/L in men and <110.0 g/L in women according to the Hematology Society of the Chinese Medical Association, and the patients were divided into two groups according to these cutoff values. Similarly, they were divided into two groups according to the cutoff values of WBC, NE, LY, MO, PLT, S100B, IL-17, MBP, and SCC-Ag (Table 2). The results showed that the CAR was correlated with sex, clinical stage, brain metastasis, S100B, IL-17, MBP, SCC-Ag, and LY (all P < 0.05). However, there was no significant correlation of the CAR with Hb, WBC, NE, MO, or PLT, as shown in Table 2.
Correlations between CAR and clinical characteristics of patients with lung adenocarcinoma.
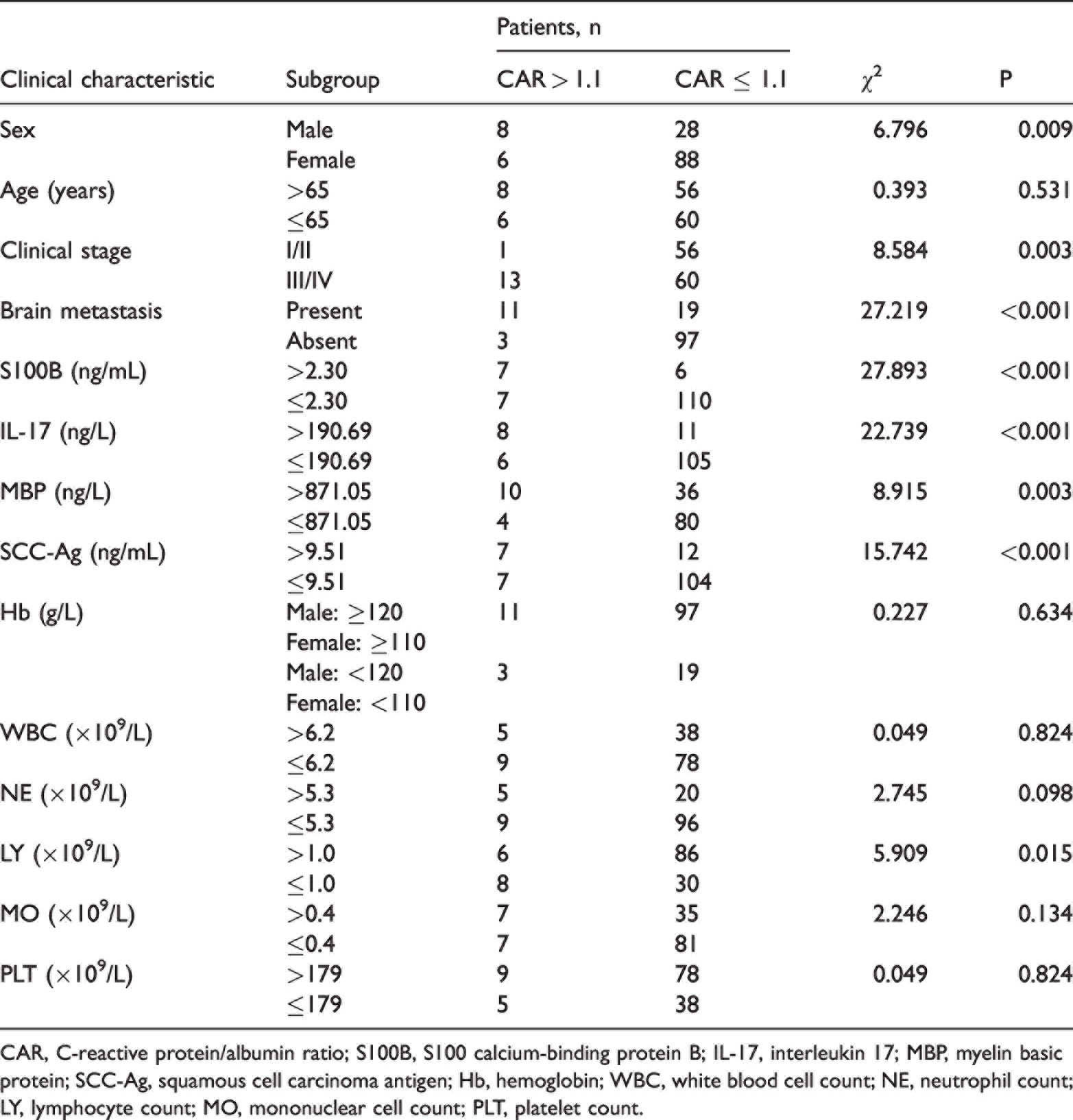
CAR, C-reactive protein/albumin ratio; S100B, S100 calcium-binding protein B; IL-17, interleukin 17; MBP, myelin basic protein; SCC-Ag, squamous cell carcinoma antigen; Hb, hemoglobin; WBC, white blood cell count; NE, neutrophil count; LY, lymphocyte count; MO, mononuclear cell count; PLT, platelet count.
Relationship between CAR and OS
The Kaplan–Meier method was used to plot OS curves of the high- and low-CAR groups, and the log-rank method was used to analyze the difference in OS between the two groups. The results showed that the median OS in the low-CAR group was 64 months (95% confidence interval (CI), 49.262–78.738), whereas the median OS in the high-CAR group was only 18 months (95% CI, 2.752–33.248). The difference in OS between the two groups was statistically significant (P < 0.001), as shown in Figure 1.

Overall survival curves of patients with high CAR (>1.1) and low CAR (≤1.1). CAR, C-reactive protein/albumin ratio.
Survival analysis
Cox univariate analysis showed that the CAR, clinical stage, brain metastasis, S100B, IL-17, SCC-Ag, CRP, ALB, and NE significantly influenced the OS of patients with lung adenocarcinoma (P < 0.001, P = 0.020, P = 0.0010, P = 0.002, P = 0.010, P = 0.025, P < 0.001, P = 0.025, and P = 0.027, respectively). However, sex, age, MBP, WBC, LY, MO, Hb, and PLT had no significant correlation with OS in patients with lung adenocarcinoma, as shown in Table 3.
Cox univariate and multivariate analyses of overall survival in patients with lung adenocarcinoma.

HR, hazard ratio; CI, confidence interval; S100B, S100 calcium-binding protein B; IL-17, interleukin 17; MBP, myelin basic protein; SCC-Ag, squamous cell carcinoma antigen; Hb, hemoglobin; WBC, white blood cell count; NE, neutrophil count; LY, lymphocyte count; MO, mononuclear cell count; PLT, platelet count; CRP, C-reactive protein; ALB, albumin; CAR, C-reactive protein/albumin ratio.
Cox multivariate analysis showed that the CAR and clinical stage were independent risk factors for OS in patients with lung adenocarcinoma (P = 0.001 and 0.045, respectively), as shown in Table 3.
Discussion
In this study, we evaluated the relationship between the CAR and various clinical characteristics in 130 patients with lung adenocarcinoma. We found that the CAR was correlated with sex, clinical stage, brain metastasis, S100B, IL-17, MBP, SCC-Ag, and LY (all P < 0.05) but not with Hb, WBC, NE, MO, or PLT. The survival curve analysis showed that the median OS was significantly longer in the low- than high-CAR group (P < 0.001). The Cox univariate and multivariate analyses between clinical characteristics and OS showed that the CAR, clinical stage, brain metastases, S100B, IL-17, SCC-Ag, CRP, ALB, and NE significantly affected the OS of patients with lung adenocarcinoma (all P < 0.05). Among these factors, the CAR and clinical stage were independent risk factors for the prognosis of patients with lung adenocarcinoma and could be used as indicators for clinical evaluation of these patients’ prognosis.
Multiple studies6–8 have shown that the inflammatory response is the “seventh feature” of tumors and is closely associated with tumor development. The relationship between inflammation and tumors is two-fold: the continuous inflammatory state will produce various inflammatory factors, which on the one hand can induce tumor development by affecting the structure of DNA and causing gene instability and on the other hand can promote the occurrence of tumors by affecting the function and state of tumor suppressor genes or proto-oncogenes. Tumor growth causes tissue inflammation, which leads to high levels of inflammatory cytokines, 9 and secreted substances can further promote the development of tumors. CRP is a typical inflammatory factor. It is an acute-stage protein 10 that, along with IL-6 and other proinflammatory factors, promotes liver production and reflects the body’s level of inflammation. The results of the present experimental study suggest that the CRP concentration is associated with the prognosis in patients with lung adenocarcinoma, which is consistent with the findings reported by Masago et al. 11 Their results were similar to ours in that CRP was a poor prognostic factor in patients with nonsquamous NSCLC. Therefore, an elevated CRP concentration suggests a poor prognosis in patients with lung cancer.
Another indicator closely related to the survival of patients with cancer is the nutritional status. 6 About one-third of patients with cancer die of poor nutrition. In patients with cancer, poor nutrition during the disease course is due to psychological factors, the consumption by the disease itself, and cancer treatments such as surgery, radiotherapy, and chemotherapy. These factors result in insufficient nutrition or energy intake, nutrient digestion or absorption disorders, and excessive consumption, thus causing a nutritional deficiency of the body and even tumor cachexia 12 and adversely affecting patients’ survival time. ALB is the main index reflecting the body’s nutritional status. Ikeda et al. 13 analyzed the association between the ALB concentration and survival of patients with NSCLC and found that higher ALB concentrations were associated with better survival. The serum ALB concentration was also associated with the prognosis in patients with lung adenocarcinoma in the present study.
Although the serum CRP and ALB concentrations were both associated with the survival and prognosis of patients with lung adenocarcinoma in the present study, neither was an independent risk factor for the prognosis. The CAR is the ratio of CRP to ALB in serum and is an indicator of systemic inflammation. The CAR is reportedly an independent poor prognostic factor in patients with pancreatic tumours, 14 nasopharyngeal carcinoma, 15 and colon cancer.16,17 In the present study, the Cox multivariate and univariate analyses showed that patients with a high CAR had shorter OS than patients with a low CAR, which was an independent risk factor for a poor prognosis in patients with lung adenocarcinoma, consistent with the results of other studies.6,18–20
The prognosis of patients with tumors is closely related to the clinical stage. Clinical staging determines whether a patient can undergo surgery, the type of surgery, and whether additional adjuvant therapy is needed. Single tumors and metastatic lesions are relatively easy to control, but the prognosis becomes poor once multiple or distant metastases occur. In this study, 130 patients with lung adenocarcinoma were divided into two groups (stage I/II and stage III/IV) according to the TNM staging of the 8th edition of the UICC TNM Classification. The univariate and multivariate analyses revealed that the clinical stage was also an independent prognostic factor in patients with lung adenocarcinoma.
In conclusion, because of the poor prognosis of patients with lung cancer, early assessment of the prognosis of patients with lung adenocarcinoma may help to develop a more effective appropriate treatment plan to improve these patients’ survival time. In this study, Cox univariate and multivariate analyses showed that the CAR and clinical stage were independent risk factors for a poor prognosis in patients with lung adenocarcinoma. These findings may serve as a reference for clinicians to evaluate the prognosis of patients with lung adenocarcinoma in the clinical setting. However, this was a single-center study with a relatively small number of patients, potentially introducing some bias. We will therefore continue to expand the number of cases and unify the standards in our further research to clarify the significance of the CAR in predicting the prognosis of patients with lung adenocarcinoma.
Consent for publication
All participants provided written informed consent for publication of their data.
Footnotes
Data availability statement
The data of this study are authentic, valid, and available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.