
Abstract
Introduction
Epistaxis or nasal hemorrhage is a common and potentially-serious condition in patients with traumatic injuries.1,2 The lifetime incidence of epistaxis is 60%, with a subset requiring medical intervention. 3 In the context of trauma, epistaxis can be an indication of coexisting injuries and prognostic indicator of mortality. The condition tends to be more severe in trauma cases, presenting complex challenges due to the involvement of various anatomical structures of the nose and face.4,5
In the trauma setting, epistaxis is particularly concerning, as it can signify underlying skull fractures or be associated with severe facial trauma, which may include multiple lacerations and fractures. 6 In such cases, epistaxis requires prompt recognition and management to prevent airway compromise and ensure adequate oxygenation, especially if the patient’s injury affects their ability to protect their airways. 3 Moreover, nasal bleeding in the context of craniofacial trauma may indicate the potential for significant vascular injury or coagulopathy, which could exacerbate blood loss and necessitate urgent surgical intervention. 7 Timely and efficient management of epistaxis in trauma cases is critical because delays can result in increased blood loss, hemodynamic instability, and development of complications that significantly increase morbidity and mortality rates.1,4
The management of epistaxis in trauma patients is influenced by factors such as the etiology, location, and severity of the hemorrhage, as well as coexisting injuries and patient stability.6,8 Conservative measures, such as nasal packing, and surgical interventions, such as arterial ligation or embolization, are among the treatment options. Prompt recognition and management of epistaxis in trauma settings are crucial to prevent airway compromise, ensure adequate oxygenation, and address potential vascular injuries or coagulopathy. 9 Of note, while conservative management may be appropriate for stable trauma patients with minor epistaxis, a high index of suspicion for more severe injuries and readiness to escalate care are essential in the management of posttraumatic epistaxis. 10 When determining the appropriate management strategy, the emergency physician should carefully assess the patient’s overall condition, including hemodynamic stability, airway patency, and response to initial treatment. Thus, understanding the pathophysiology of epistaxis in the context of trauma, along with the implementation of evidence-based treatment protocols, is paramount to improving clinical outcomes in these patients.11 -13
Despite the importance of epistaxis management in patients with trauma, there is limited research on the epidemiology, risk factors, and outcomes of this condition. Previous studies have identified several risk factors for epistaxis, including age, hypertension, anticoagulant use, and inherited bleeding disorders.14,15 However, the specific risk factors associated with traumatic epistaxis and their impact on outcomes have not been extensively studied.10,16,17 Similarly, while some studies have reported the outcomes of epistaxis in the general population, the outcomes of traumatic epistaxis, particularly in relation to different management strategies, remain largely unknown.16,18
The aim of this retrospective study was to examine the epidemiology of traumatic epistaxis and evaluate the association between risk factors and outcomes.
Methodology
This retrospective case-control study analyzed data from the National Trauma Data Bank (NTDB) from 2013 to 2015. The NTDB is a large database that contains information on trauma-related incidents in the United States. The inclusion criteria were patients with a primary diagnosis of posttraumatic epistaxis admitted to participating trauma centers between 2013 and 2015 who had data on demographics, injury characteristics, management strategies, and outcomes. Patients with incomplete or missing data were excluded. Patients with an ICD-9 code specific to nasal hemorrhage secondary to injury were included in the study regardless of the severity of their overall injuries or concomitant conditions. This allowed for an analysis of the spectrum of patients experiencing posttraumatic epistaxis, from mild to severe cases, and ensured that the study population represented a diverse range of patients who experienced epistaxis as a direct consequence of traumatic injury. While some patients in the study were comatose or had a high injury severity score (ISS), these conditions were not necessarily a direct result of the epistaxis itself, but rather a consequence of the severity of the overall traumatic injury. The presence of coma or high ISS does not preclude the possibility that epistaxis was a primary and direct consequence of the trauma.
Relevant variables, including patient demographics, nature, and severity of the trauma, were assessed using ISS, health and safety characteristics, past medical histories, clinical parameters, health service utilization, and complications related to epistaxis or its management. The primary outcome was mortality. Patients were divided into 2 groups based on the management approach used to treat posttraumatic epistaxis: conservative or operative treatment. The conservative treatment group included patients managed with noninvasive or minimally-invasive techniques, such as nasal packing, cauterization, or the use of hemostatic agents. The operative treatment group consisted of patients who underwent surgical interventions to control epistaxis, such as endoscopic cauterization, ligation of bleeding vessels, or embolization of the offending arteries. Selection bias was minimized by including a diverse range of patients with posttraumatic epistaxis from the NTDB. Information bias was addressed by excluding incomplete data and using standardized ICD-9 coding. Confounding bias was managed using multivariate analyses to control for confounders. Despite these efforts, some residual bias may remain due to the retrospective design.
Descriptive statistics were used to summarize the patient characteristics, injury severity, and outcomes. Univariate analyses were performed to identify factors associated with the outcomes of interest, and multivariate analyses, such as logistic regression, were conducted to identify independent predictors of outcomes while controlling for potential confounders. Odds ratios (ORs) with 95% confidence intervals (CIs) were considered significant predictors. All procedures adhered to ethical standards for research involving human subjects. However, the study was deemed exempt from Institutional Review Board approval due to the use of a de-identified national database.
Results
Demographic and Clinical Characteristics
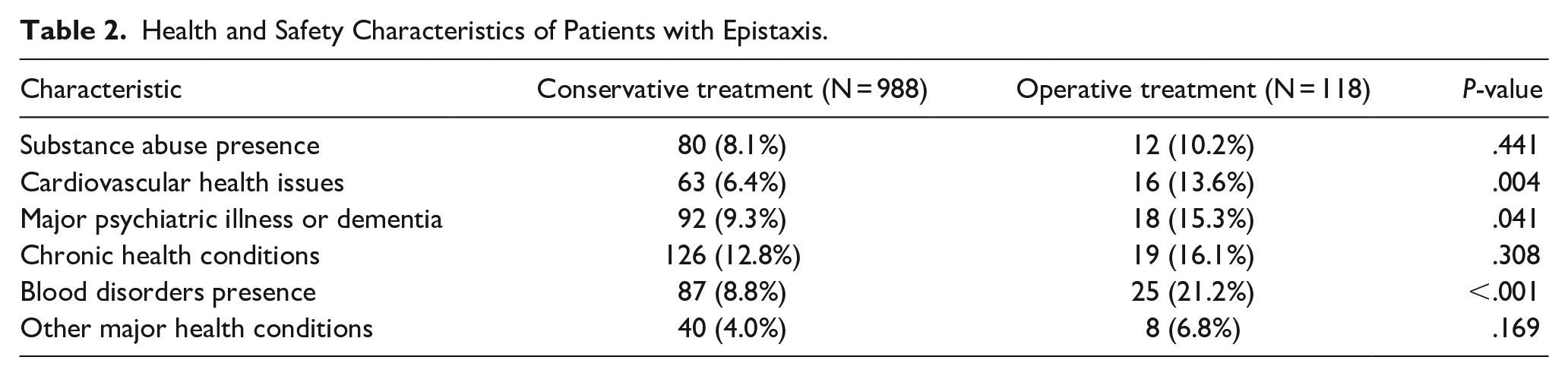
A total of 1106 patients were evaluated, with 988 (89.3%) receiving conservative treatment and 118 (10.7%) undergoing operative intervention. The operative group was significantly older (median age 65.0 years, IQR 32.0-80.0) than the conservative group (median age 44.0 years, IQR 23.0-65.0; P < .001). The operative group had a higher proportion of patients aged ≥65 years (50.8% vs 25.9%, P < .001). Sex distribution did not differ significantly between groups (P = .759) (Table 1). Falls were the predominant mechanism of injury in both groups but were significantly more common in the operative group (59.3% vs 39.6%, P = .001). The operative group showed a higher prevalence of cardiovascular health issues (13.6% vs 6.4%, P = .004), psychiatric illnesses including dementia (15.3% vs 9.3%, P = .041), and blood disorders (21.2% vs 8.8%, P < .001). No significant differences were observed in race, intent of injury, or substance abuse between the groups (Tables 1 and 2).
Demographic and Clinical Characteristics of Patients with Epistaxis.
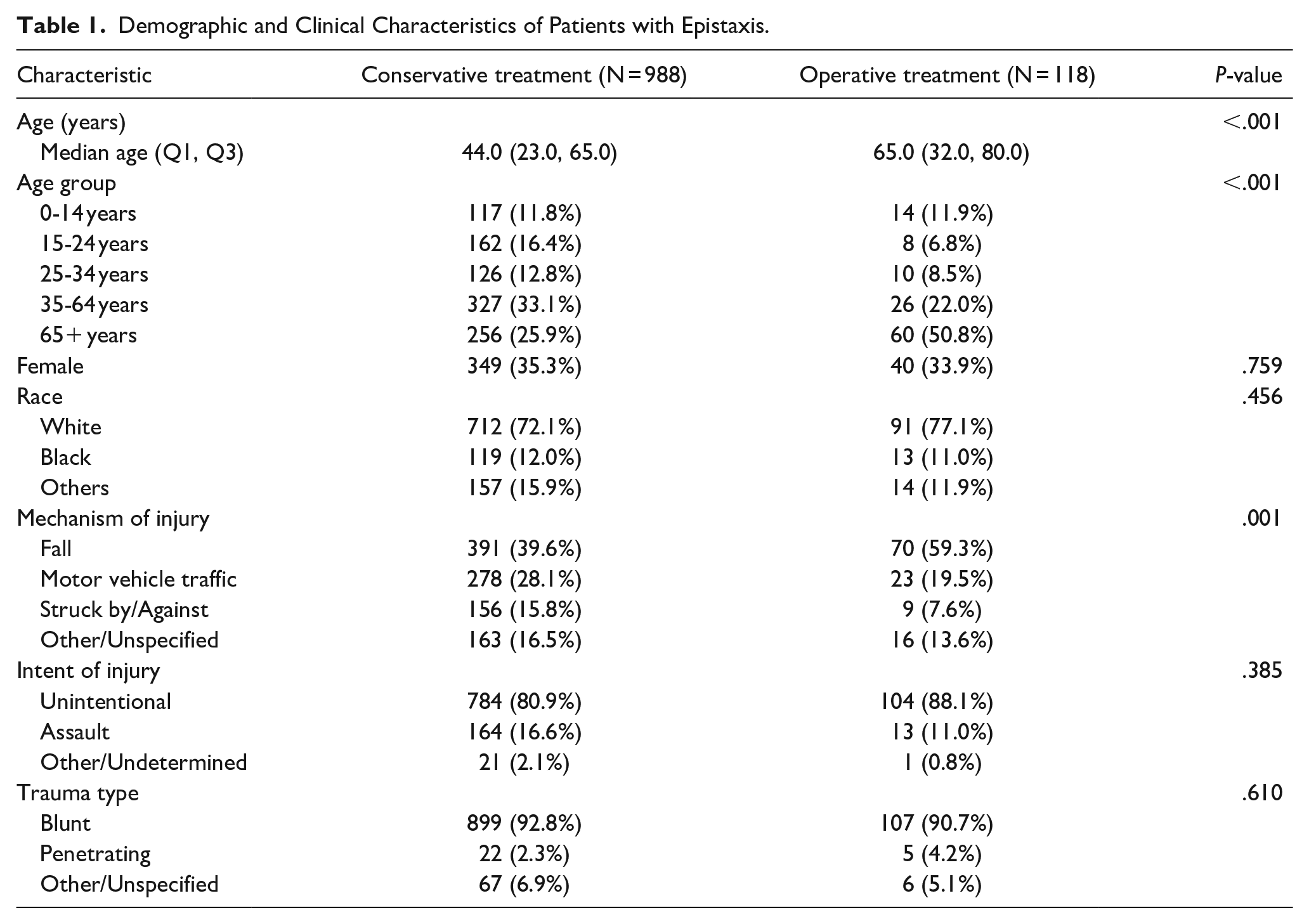
Health and Safety Characteristics of Patients with Epistaxis.
Clinical Parameters and Hospital Course
In the emergency department (ED), the operative group exhibited significantly-higher median systolic blood pressure (SBP; 142.0 mmHg, IQR 128.0-165.0) than the conservative group (136.0 mmHg, IQR 121.0-151.0; P = .031). Other vital signs, including heart rate and respiratory rate, and Glasgow Coma Scale (GCS) scores did not differ significantly between groups (Table 3).
Clinical Parameters in Epistaxis Patients.
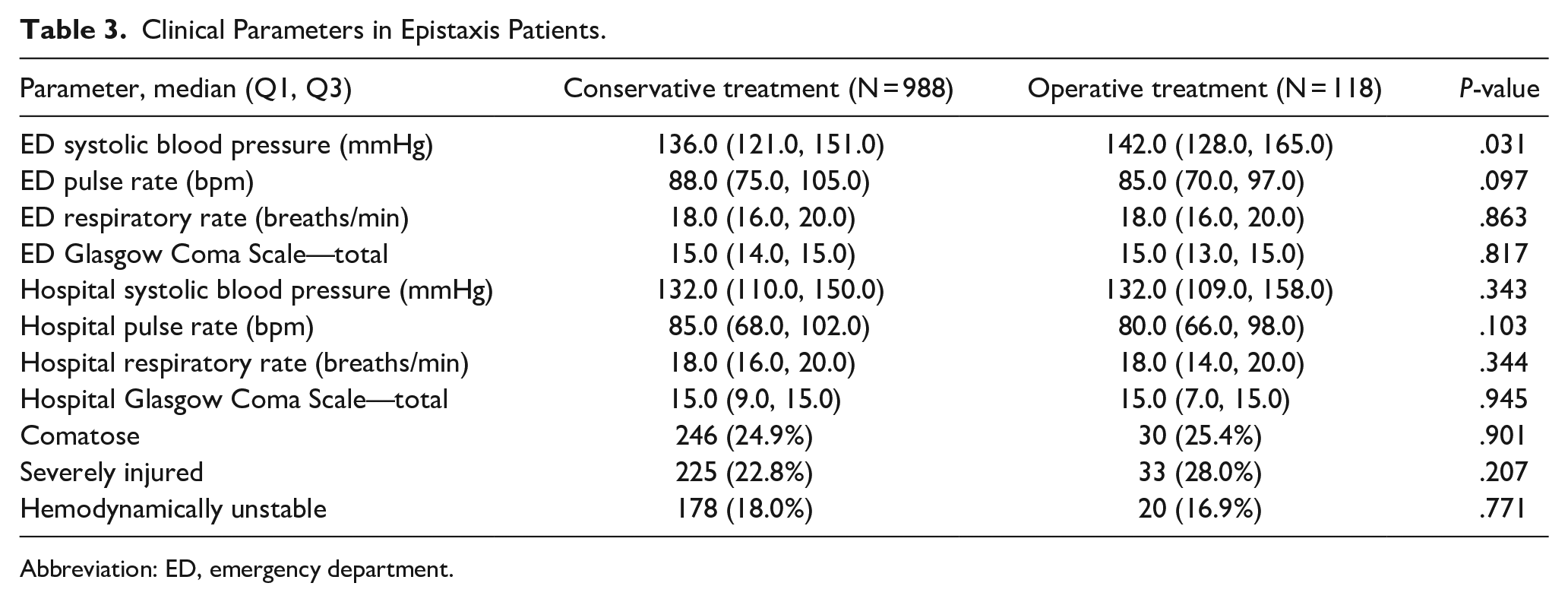
Abbreviation: ED, emergency department.
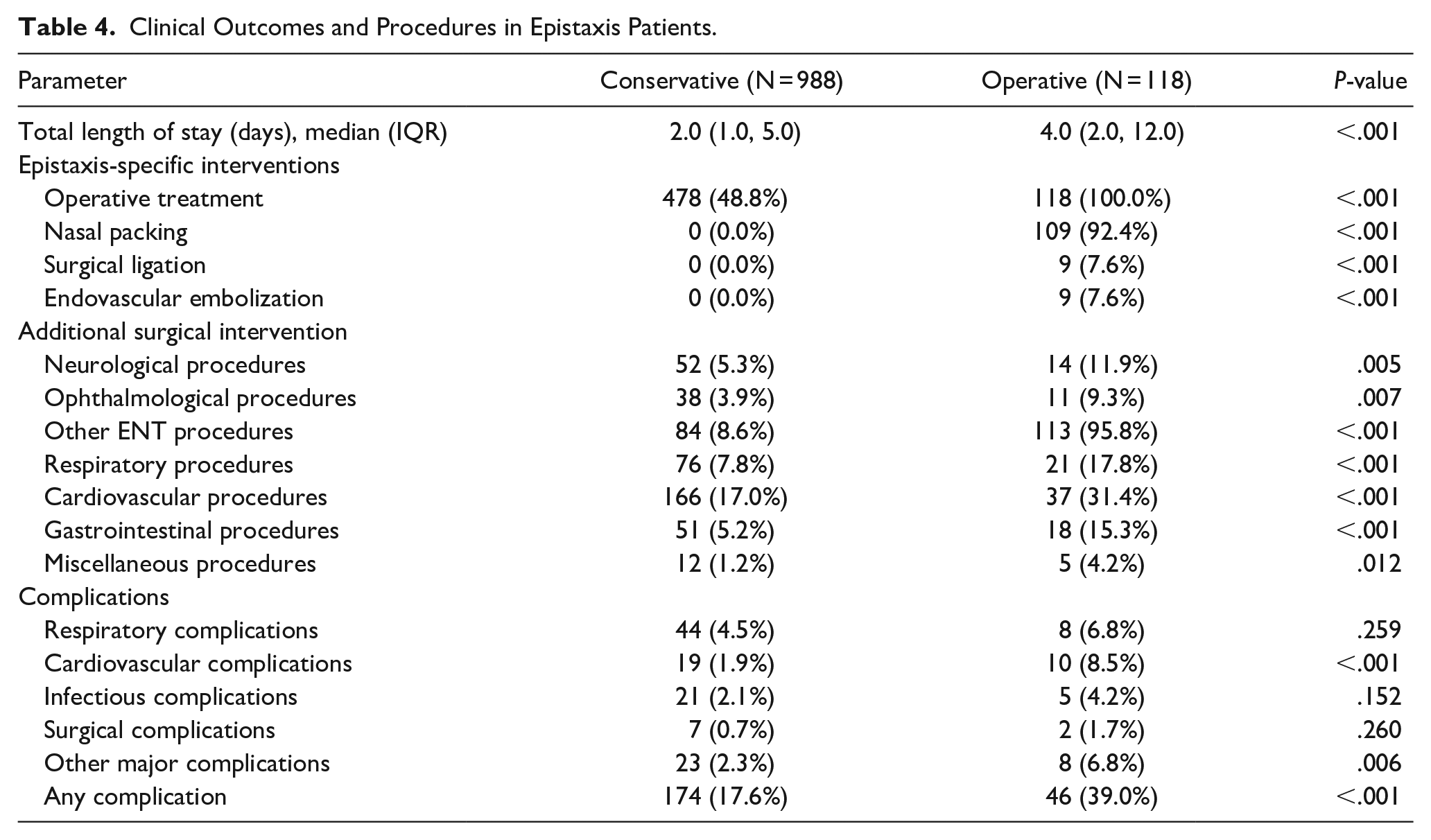
The operative group experienced longer hospital stays (median 4 days, IQR 2-12) than the conservative group (median 2 days, IQR 1-5; P < .001). Rates of comatose state, severe injury (ISS > 15), and hemodynamic instability were comparable between groups (Tables 3 and 4).
Clinical Outcomes and Procedures in Epistaxis Patients.
Interventions and Complications
The operative group underwent significantly-more epistaxis-specific interventions, including nasal packing (92.4%), surgical ligation (7.6%), and endovascular embolization (7.6%; all P < .001). They also had higher rates of additional surgical interventions across multiple systems, including neurological, ophthalmological, respiratory, cardiovascular, and gastrointestinal procedures (P < .001 to P = .012) (Table 4). The operative group experienced a higher overall complication rate (39.0% vs 17.6%, P < .001), with notably-higher incidences of cardiovascular complications (8.5% vs 1.9%, P < .001) and other major complications (6.8% vs 2.3%, P = .006). Respiratory complications, infectious complications, and surgical complications did not differ significantly between groups (Table 4).
Mortality Risk Factors
Logistic regression analysis revealed several factors associated with mortality (Table 5). The GCS total score was inversely associated with mortality [OR = 0.932, 95% CI (0.889–0.977), P = .003]), indicating that higher GCS scores were associated with lower mortality risk. Blood vessel injury [OR = 5.509, 95% CI (2.003–15.153), P = .001] and cardiovascular surgery [OR = 7.170, 95% CI (4.070–12.632), P < .001] were significantly associated with an increased risk of mortality. Age [OR = 0.996, 95% CI (0.991–1.002), P = .208] and SBP [OR = 0.999, 95% CI (0.994–1.004), P = .760] were not statistically-significant predictors of mortality. Other variables, such as ISS, sex, epistaxis management, and various mechanisms of injury (including falls, firearms, and motor vehicle traffic incidents), did not show a significant association with mortality.
Logistic Regression Analysis of Factors Affecting Death Under Care.
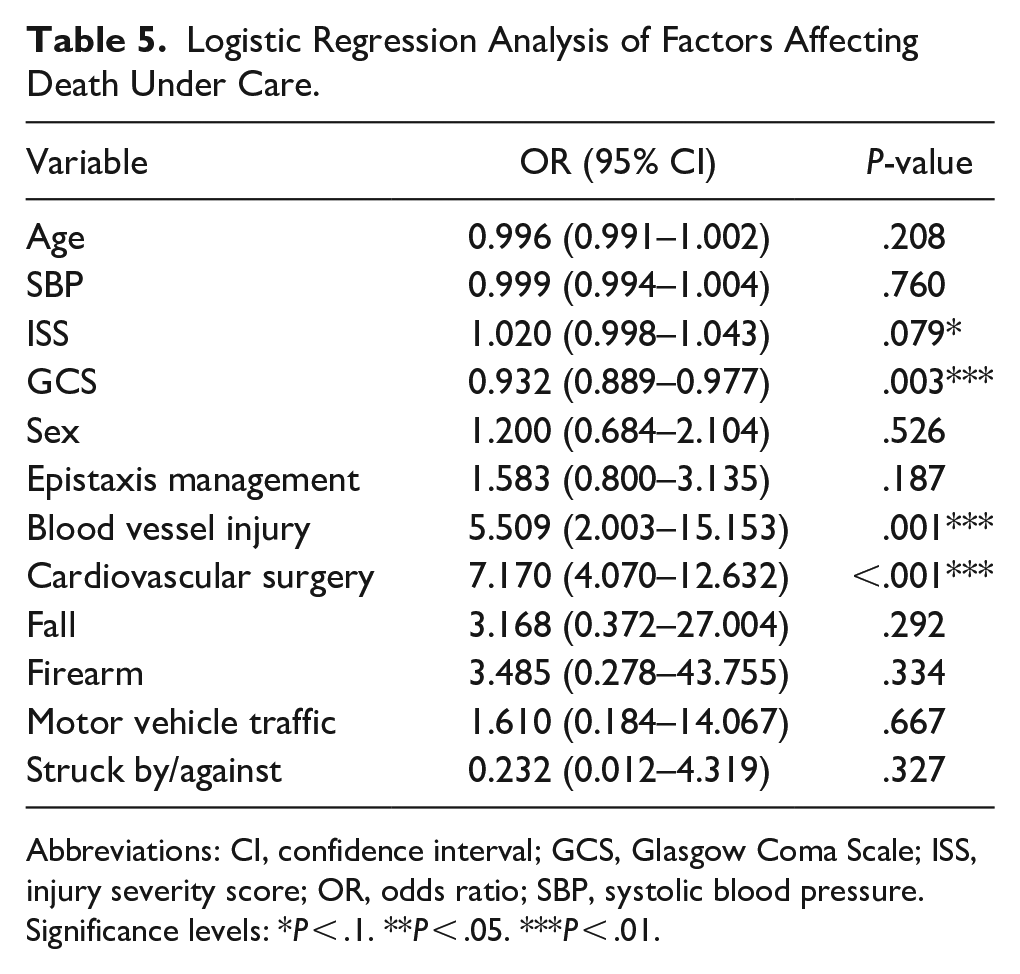
Abbreviations: CI, confidence interval; GCS, Glasgow Coma Scale; ISS, injury severity score; OR, odds ratio; SBP, systolic blood pressure.
Significance levels: *P < .1. **P < .05. ***P < .01.
Discussion
Our results substantiate the high success rate of conservative management in controlling epistaxis, which Gilyoma and Chalya 19 and Razdan et al 20 also noted to be effective. However, the necessity for operative intervention in selected cases suggests the need for a multidimensional assessment strategy before determining the treatment pathway.21 -24 The frequent initiation of operative treatments owing to the failure of conservative methods highlights the complexity of care decisions in clinical practice. The inclusion of longer hospital stays and a higher incidence of invasive procedures within the operative cohort reflects well-documented correlations, as seen in the studies by Carey and Sheahan 12 and Beck et al. 4 Our study further identified significant predictors of mortality, such as the GCS total score, and the intricate relationship with systemic factors, such as blood vessel injuries and cardiovascular surgeries. These findings resonate with those of earlier studies that showed the prognostic value of initial clinical assessments and intricate impact of comorbid conditions.5,25
The elevated prevalence of blood disorders in the operative group further indicates the likelihood that these patients present with more severe forms of epistaxis, requiring surgical intervention to achieve hemostasis.17,26 This critical relationship between patient demographics and clinical presentations forms a pivotal part of the discussion as it directly affects decision-making processes in emergency and surgical settings, shaping tailored treatment approaches for optimal patient outcomes. 27 Furthermore, this study elucidates the substantive role of injury mechanisms in the severity and subsequent management of epistaxis.28 -30 The higher incidence of falls reported in the operative group suggests a relationship between the nature of the traumatic event and the invasiveness of the required intervention. This may indicate that falls, particularly in the elderly, are associated with significant blunt force trauma to the head and face, leading to more profound vascular injuries that necessitate surgical management.31 -33
Moreover, despite a higher complication rate in the operative group, the lack of a significant difference in mortality rates between the 2 groups suggests that with sufficient expertise and resources, a wide spectrum of epistaxis severity can be effectively managed. It also underscores the necessity for vigilant postoperative monitoring to mitigate complications and rigorous selection of candidates for surgery, balancing the risks and benefits of operative intervention. 34 Hence, the discussion pivots toward considering the balance between intervention efficacy and healthcare resource management, highlighting an area ripe for further research and development within the field of trauma care.
The correlation observed between higher GCS scores and lower mortality rates suggests a prognostic value in assessing neurological status in cases of epistaxis management.35,36 This aligns with other trauma research that underscores the importance of early-neurological assessment in predicting patient outcomes. The integration of such scales into treatment algorithms may provide physicians with additional tools to assess the severity of trauma and make informed decisions regarding the aggressiveness of the intervention required. A noteworthy aspect of this study is the lack of impact of demographic factors, such as sex, and systemic health indicators, such as SBP, on mortality, indicating that these factors may not be major determinants of the prognosis of trauma-induced epistaxis. Instead, specific clinical factors, including the extent of blood vessel injuries and the need for cardiovascular surgery, have emerged as more substantial predictors of mortality. This finding reinforces the importance of a nuanced approach to patient evaluation, focusing on clinical presentation and specific injury characteristics rather than on broad demographic criteria. 36
This study has several key limitations. As a retrospective analysis using the NTDB, it is subject to potential selection and information bias. The NTDB may not capture all cases, particularly from smaller institutions, potentially skewing the representation of patient demographics and treatment approaches. Reliance on ICD-9 coding introduces the risk of misclassification errors. The simplification of interventions into conservative and operative categories may not fully reflect the complexity of clinical decision-making. The lack of long-term follow-up data limits our understanding of outcomes and recurrence rates. While we controlled for many confounders, unmeasured variables could still influence results. Importantly, the NTDB does not distinguish between anterior and posterior epistaxis, potentially obscuring differences in management and outcomes. The absence of data on specific airway protection strategies also limits our analysis of epistaxis severity and complications. Lastly, the 2013 to 2015 data collection period may not reflect current practices, and the use of aggregated data prevented access to individual patient records and imaging studies. Future research should address these limitations by including more detailed, case-specific information, long-term follow-up data, and more recent clinical practices to enhance our understanding of trauma-related epistaxis management.
Conclusion
A comprehensive analysis of epistaxis management within the trauma population revealed critical insights into the demographic and clinical factors influencing treatment preferences and outcomes. A significant finding of this study is the stark age-related divergence in treatment modalities, with older patients noticeably predisposed to receiving operative interventions. This trend emphasizes the complex interrelation between age, coexisting health conditions, and the severity of epistaxis, underscoring the need for an individualized approach to patient care in traumatic instances of epistaxis. The study’s findings support the development of well-defined and evidence-based guidelines to optimize the management of epistaxis in trauma settings. Such guidelines should focus on patient-specific factors, including age and comorbid health status, to ensure the most effective and efficient use of health care resources.
Footnotes
Acknowledgements
Author Contributions
Ahmad K. Alnemare conceived the idea, developed the concept, and performed the data analysis and manuscript writing.
Availability of Data and Material
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study employed de-identified data sourced from the NTDB, adhering to the ethical standards established by institutional and national research committees. Given that the NTDB data are de-identified and not generated by the author, this study did not require ethical review, written informed consent, and approval according to applicable institutional guidelines.